Ventricular septal defect (VSD) is a congenital heart defect in which there is a violation of the integrity of the septum between the right and left ventricles. As a result, blood from one ventricle enters the other and disrupts the normal functioning of the heart and blood circulation in the body. Sometimes the septum is completely absent. VSD is formed as a result of a violation of embryonic development in the womb. Often the disease is accompanied by other heart defects. VSD in adults can appear when the interventricular septum is ruptured during acute myocardial infarction.
Causes of ventricular septal defect
As stated earlier, a VSD is formed during the embryonic stage. It is important for expectant mothers to be careful about their health and the health of the developing fetus. Therefore, it is necessary to protect yourself and your unborn child from the effects of negative factors, such as:
- nicotine and tar released when smoking;
- alcohol;
- uncontrolled use of medications;
- stressful situations;
- physical exercise;
- inflammatory diseases;
- premature birth.
Reviews of doctors providing the service - Endovascular closure of atrial septal defect
I fell into the hands of the best phlebologist - Malakhov Yuri Stanislavovich.
Explains everything clearly, to the point, and is always open to questions. After the operation, we kept in touch via SMS. I was satisfied and, most importantly, healthy. Read full review Daria Alexandrovna B
08.12.2021
Many thanks to Dr. Malakhov Yuri Stanislavovich for the RFO operation performed on my mother in June 2021. Mom no longer complains of pain in her leg, cramps or leg fatigue. She works a lot in the garden, walks several kilometers without getting tired, although she is already over 70. Good health to you... Read full review
Svetlana Vladimirovna Ch
06.12.2021
Symptoms of ventricular septal defect
Because the threshold is congenital, the first symptoms may appear during the first days of life:
- lack of appetite, sluggish sucking with frequent breaks;
- slow weight gain;
- fatigue (children sleep a lot);
- the appearance of shortness of breath;
- swelling in the legs and abdomen;
- tachycardia.
With small defects, external symptoms may not appear and are detected only by listening to the heart.
Pathology may not make itself felt until adulthood. The symptoms in an adult are almost the same as in a child. Additionally, there may be complaints about:
- deterioration in performance;
- fatigue.
If you notice similar symptoms in your child or yourself, contact your doctor. The cardiology center of the Federal Scientific and Clinical Center of the Federal Medical and Biological Agency conducts comprehensive heart research programs. Make an appointment with a cardiologist to promptly stop the disease and prevent the development of the disease.
Department of Cardiac Surgery and Intensive Care of the Children's Hospital named after. N.F. Filatova
On the one hand, there is a cardiologist who believes that an operation should be performed because he sees indications for this, on the other hand there is a cardiac surgeon who believes that we need to wait a little longer...
I kindly ask specialists in the field of cardiology and cardiac surgery to respond and write their professional opinion about our problem.
On the fourth day of life (in the maternity hospital), my daughter was diagnosed with congenital heart disease: ASD 1 cm. They said that the defect was large, there was almost complete absence of a septum. However, they said that we would watch and that there was a chance that the defect could close or at least decrease. At 5 months, we did another ultrasound of the heart, which showed that the defect had not changed in 5 months. The cardiologist and cardiac surgeon agreed that we will continue to monitor, since there is no deterioration observed. For the next 3 months we lived a normal life: we learned to sit, stand up, talk, gave up breastfeeding, etc... However, we began to notice that the child began to get tired very quickly, began to sweat a lot (when he eats, sleeps, plays, cries and etc., i.e. almost all the time), appetite has deteriorated very much (she stopped eating any complementary foods: no porridge, no puree, and the formula in our current 9 months eats about 100 ml, and then refuses), breathing has become rapid at times (we ourselves and our cardiologist noticed), the skin is pale, sometimes I notice a bluish appearance of the nasolabial triangle, my daughter has practically stopped gaining weight (lately, in order not to lose weight, I have to practically forcefully push porridge into her - at least a little spoons, give the mixture more often; and taking this into account, over the last month we have not gained weight, but have lost 150 grams of weight). At 8 months we again did an ultrasound of the heart. The cardiologist at the clinic saw indications for surgical treatment. However, the cardiac surgeon did not believe these results (not their institution). We had another ultrasound with them. The cardiologist again saw the indications for surgery, but for some reason the cardiac surgeon did not want to perform the operation. He says that there is hope to close the defect with an occluder, and that they perform these operations when the child weighs at least 14 kg. He says to wait until 2-3 years. But the deterioration is obvious! Both the cardiologist and the cardiac surgeon saw them! The heart surgeon said that all negative symptoms and consequences will go away almost immediately after the operation, so he says to wait. He said: “If you tell me “do the operation!”, I won’t go anywhere, I will prepare the documents for the operation and we will do it. But if there is a chance to have surgery using an occluder, then I would wait...” Now I’m completely at a loss. On the one hand, there is a cardiologist who believes that an operation should be performed because he sees indications for this, on the other hand there is a cardiac surgeon who believes that the deterioration is not critical and that we can wait until we gain at least 14 kg. But we hardly eat! Almost no weight gain! Deterioration is visible on ultrasound (including the defect has increased!). What kind of critical deterioration must we wait for before we are sent for surgery? Will we face irreversible consequences (pulmonary hypertension, heart failure, etc.)? What would you recommend in our situation? I am very afraid of missing the opportune moment for surgical treatment of our congenital heart disease. PS The results of the three heart ultrasounds discussed in the message can be viewed in the forum at the following link: https://forum.dearheart.ru/5/19365/ — Sincerely, Katya’s Mom ‹ Large secondary ASD ASD 8 mm ›
Diagnostics
It is possible to diagnose VSD in an embryo during pregnancy already in the second or third trimester when performing screening ultrasounds. Knowing about heart defects, parents understand in advance what examinations the child will need to undergo after birth:
- Ultrasound of the heart with duplex examination (study of blood flow);
- chest x-ray;
- pulse oximetry – measurement of oxygen concentration in the blood;
- MRI of the heart.
For an adult patient who does not know about his diagnosis, the doctor conducts an initial survey and examination. Blood pressure is measured and the heart is listened to. After collecting anamnesis, a referral is issued for laboratory tests and instrumental examination. To the above may be added:
- ECG;
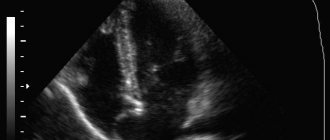
- Echocardiography;
- cardiac catheterization - insertion of a catheter with a radiopaque substance.
Advantages of the endovascular technique
The endovascular method of closing the defect compares favorably with the operation of suturing the ASD. The latter requires artificial maintenance of blood circulation during surgery, has more contraindications and a significant rehabilitation period. Despite the fact that surgical treatment has become firmly established in practice and has been used for a long time, it is now giving way to the endovascular method.
The main advantage is that endovascular surgery is minimally invasive surgery. There are no scars left behind and the procedure does not require incisions or open access. The endovascular method has an extremely low rate of postoperative complications. Patients do not require long-term hospitalization and rehabilitation.
At the moment, endovascular surgery is a generally recognized world standard that meets all safety and effectiveness requirements.
Prevention
There are no special requirements for the prevention of VSD. Doctors can give several recommendations to pregnant women to prevent the development of the disease in their unborn child:
- Healthy food;
- avoid excessive physical activity;
- spend more time outdoors;
- to refuse from bad habits;
- consult a doctor for any ailments or illnesses;
- do not take medications on your own;
- Visit a doctor to monitor the progress of your pregnancy in a timely manner.
If detected early, the pathology can be easily treated. Don't waste a minute! Get your heart checked to prevent complications.
Complications
A ventricular septal defect can lead to various diseases, such as heart rhythm disturbances or valvular pathology, but the most common are:
- Heart failure.
It is a consequence of constant overload of the heart and leads to blood stagnation, resulting in hypoxia of tissues and organs. - Stroke.
As blood passes through the hole in the interventricular septum, a constant turbulent current occurs, which can lead to the formation of blood clots. By causing blockage of blood vessels in the brain, they cause a stroke. In this case, the main risk group consists of patients with a large defect size. - Endocarditis.
It is an inflammation of the inner lining of the heart. In the absence of timely and professional intervention, it can lead to more serious complications. - Eisenmenger syndrome.
This is severe and irreversible pulmonary hypertension. It occurs due to hypertrophy of the right ventricle and expansion of the pulmonary artery. Eisenmenger syndrome in VSD is rarely diagnosed.
Treatment of ventricular septal defect
If a ventricular septal defect is detected in an embryo, treatment may be delayed for up to a year, because there is a possibility that the violation will go away on its own. In other cases, treatment is necessary.
In the cardiology center of the Federal Scientific and Clinical Center of the Federal Medical and Biological Agency, treatment of VSD in adults (over 18 years of age) is carried out with the help of medications or surgical intervention. Drug treatment can be carried out on an outpatient basis or under the supervision of specialists in the therapeutic department of our center. The prescription of drugs depends on the degree of damage to the septum and the presence of concomitant ailments. These may be beta blockers, drugs that reduce the load on the heart. The list of drugs and their dosage is determined strictly by the attending cardiologist.
VSD can be radically eliminated surgically. Endovascular correction is considered the safest and least traumatic. A special device (occluder) is passed through the catheter to the heart muscle, which covers the site of the defect with a patch; over time, the defect heals. After the correction, the patient is transferred to the intensive care unit for 24 hours for observation, and the next day he is released home. No post-operative rehabilitation is required - quick recovery and return to normal life.
The second method is plastic surgery of the defect. Open heart surgery is performed by opening the chest. Before the procedure begins, the patient is connected to a heart-lung machine. The heart is cut and the defect is sutured using a patch of artificial or native pericardium, which is fixed with sutures along the edges of the defect. The method is more traumatic and requires longer rehabilitation, about a month. If VSD occurs in the acute period of myocardial infarction, then surgical treatment is performed either on the first day or in the subacute period, which is safer.
Publications in the media
Ventricular septal defect (VSD) is a congenital heart defect with communication between the right and left ventricles.
Etiology • Congenital malformations (isolated VSD, part of a combined congenital heart disease, for example, tetralogy of Fallot, transposition of the great vessels, truncus arteriosus, tricuspid valve atresia, etc.) • There is evidence of autosomal dominant and recessive types of inheritance. In 3.3% of cases, this defect is also found in direct relatives of patients with VSD • Rupture of the interventricular septum due to trauma and MI.
Statistical data • VSD accounts for 9–25% of all congenital heart defects • Is detected in 15.7% of live-born children with congenital heart disease • As a complication of transmural myocardial infarction - 1–3% • 6% of all VSDs and 25% of VSDs in infants are accompanied by a patent ductus arteriosus, 5 % of all VSDs - coarctation of the aorta, 2% of congenital VSDs - aortic valve stenosis • In 1.7% of cases, the interventricular septum is absent, and this condition is characterized as a single ventricle of the heart • The ratio of male to female sex is 1:1.
Pathogenesis. The degree of functional impairment depends on the amount of blood discharge and total pulmonary vascular resistance (TPVR). When shunting from left to right and the ratio of pulmonary minute volume to systemic blood flow (Qp/Qs) is less than 1.5:1, pulmonary blood flow increases slightly, and no increase in PVVR occurs. With large VSDs (Qp/Qs more than 2:1), pulmonary blood flow and pulmonary blood flow significantly increase, and pressures in the right and left ventricles are equalized. As the blood volume increases, the direction of blood discharge may change - it begins to occur from right to left. Without treatment, right and left ventricular failure and irreversible changes in the pulmonary vessels (Eisenmenger syndrome) develop.
Variants of VSD • Membranous VSD (75%) are located in the upper part of the interventricular septum, under the aortic valve and the septal cusp of the tricuspid valve, often close spontaneously • Muscular VSD (10%) are located in the muscular part of the interventricular septum, at a considerable distance from the valves and conduction system , are multiple, fenestrated and often close spontaneously • Supracrestal (VSD of the right ventricular outflow tract, 5%) are located above the supraventricular crest, often accompanied by aortic regurgitation of the aortic valve, do not close spontaneously • Patent AV canal (10%) is found in the posterior part of the interventricular septum, near the site of attachment of the rings of the mitral and tricuspid valves, often found in Down syndrome, combined with ASD of the ostium primum type and malformations of the leaflets and chords of the mitral and tricuspid valves, does not close spontaneously • Depending on the size of the VSD, small ones are distinguished (Tolochinov-Roger disease ) and large (more than 1 cm or half the diameter of the aortic orifice) defects.
Clinical picture
• Complaints: see Atrial septal defect.
• Objectively • Pallor of the skin • Harrison's furrows • Increased apical impulse, trembling in the area of the left lower edge of the sternum • Pathological splitting of the second tone as a result of prolongation of the ejection period of the right ventricle • Rough pansystolic murmur at the left lower edge of the sternum • With supracrestal VSD - aortic diastolic murmur insufficiency.
Instrumental diagnostics
• ECG: signs of hypertrophy and overload of the left parts, and with pulmonary hypertension - also of the right.
• Jugular venography: high-amplitude A waves (atrial contraction with a rigid right ventricle) and, sometimes, V wave (tricuspid regurgitation).
• EchoCG •• Hypertrophy and dilatation of the left parts, and in case of pulmonary hypertension - also the right ones •• Visualization of VSD in Doppler and B-mode •• Diagnosis of associated anomalies (valvular defects, coarctation of the aorta, etc.) •• Determine systolic pressure in the right ventricle , degree of shunt and Qp/Qs •• Transesophageal echocardiography is performed in adults.
• X-ray of the chest organs •• For small VSDs - a normal x-ray picture •• Bulging of the left ventricular arch, increased pulmonary vascular pattern •• With pulmonary hypertension - bulging of the pulmonary artery arch, expansion and lack of structure of the roots of the lungs with a sharp narrowing of the distal branches and depletion of the pulmonary vascular system drawing.
• Radionuclide ventriculography: see Atrial septal defect.
• Catheterization of the cardiac chambers •• Indicated for suspected pulmonary hypertension, before open-heart surgery and in case of conflicting clinical data •• Calculate Qp/Qs •• Tests with aminophylline and oxygen inhalation are performed to determine the prognosis regarding the reversibility of pulmonary hypertension.
• Left ventriculography, coronary angiography: visualization and quantification of shunt, diagnosis of CAD in the presence of symptoms or before surgery.
Drug treatment. With an asymptomatic course and normal pressure in the pulmonary artery (even with large defects), conservative treatment is possible for up to 3–5 years of life. If there is stagnation in the pulmonary circulation, use peripheral vasodilators (hydralazine or sodium nitroprusside), which reduce the discharge from left to right. For right ventricular failure - diuretics. Before and for 6 months after uncomplicated surgical correction of VSD - prevention of infective endocarditis.
Surgery
Indications • Asymptomatic - if spontaneous closure of the defect does not occur by 3–5 years of life, although better results are achieved with surgical treatment before the age of 1 year • Heart failure or pulmonary hypertension in young children • In adults, the Qp/Qs ratio is 1 .5 or more.
Contraindications: see Atrial septal defect.
Methods of surgical treatment. Palliative intervention - narrowing of the pulmonary trunk with a cuff, is performed when emergency surgery is necessary for children weighing less than 3 kg, with concomitant heart defects and little clinical experience in radical correction of the defect at an early age. In case of a traumatic defect in the area of the membranous part of the interatrial septum, suturing of the defect is possible. In other cases, the defect is repaired with a patch made of autopericardium or synthetic materials. In case of post-infarction VSD, plastic surgery of the defect is performed with simultaneous coronary bypass surgery.
Specific postoperative complications: infective endocarditis, AV block, ventricular arrhythmias, recanalization of VSD, tricuspid valve insufficiency.
Forecast. In 80% of patients with large VSDs, spontaneous closure of the defect occurs within 1 month, in 90% - before the age of 8 years, there are isolated cases of spontaneous closure of VSDs between the ages of 21 and 31 years. With small defects, life expectancy does not change significantly, but the risk of infective endocarditis increases (4%). With a medium-sized VSD, heart failure usually develops in childhood, and severe pulmonary hypertension is rare. Large VSDs without a pressure gradient between the ventricles lead to the development of Eisenmenger syndrome in 10% of cases; most of these patients die in childhood or adolescence. Emergency surgical intervention is required in 35% of children within 3 months after birth, 45% within 1 year. Maternal mortality during pregnancy and childbirth with Eisenmenger syndrome exceeds 50%. With post-infarction VSD, 7% of patients survive 1 year in the absence of surgical treatment. Hospital mortality after narrowing of the pulmonary artery is 7–9%, 5-year survival rate is 80.7%, 10-year survival rate is 70.6%. Mortality during surgical treatment of post-infarction VSD is 15–50%. In-hospital mortality during closure of isolated congenital VSD with low LVVR is 2.5%, with high LVVR - less than 5.6%.
Abbreviations. Qp/Qs is the ratio of the pulmonary minute volume of blood flow to the systemic one. TPVR - total pulmonary vascular resistance.
ICD-10 • Q21.0 VSD