Development mechanism and reasons
The disease spreads not only to the walls of the aorta, but also to the aortic valve of the heart.
According to statistics, every fifth valve defect is caused by calcification. This acquired pathology of the aortic valve is also called true stenosis. Aortic calcification leads to changes in the structure of the valve, fusion of the leaflets, which provokes its insufficiency. This phenomenon causes a sharp pressure drop to occur as blood flows from the left ventricle to the aorta. In the ventricular cavity, blood pressure is increased, but at the mouth of the aorta it decreases sharply. Because of this, the ventricular cavity loses its elasticity, and its walls hypertrophy. This phenomenon causes a weakening of the functions of the left ventricle and a decrease in the volume of blood ejected from it. The hemodynamic overload from which the left ventricle suffers extends to the atrium and the vessels of the pulmonary circulation.
Due to the accumulation of calcium in the body, a person may develop calcification of not only the aortic valve, but also the mitral valve. In this case, calcium is deposited on the annulus fibrosus of the valve. Many people with calcification do not have valve dysfunction, but they are at risk of developing mitral regurgitation, which occurs when blood flows from the left ventricle into the left atrium during systole.
The causes of excessive calcium accumulation in the blood are:
- Age: In older people, calcium is washed out of the bones and enters the blood.
- Kidney disease: The inability of the excretory system to remove calcium allows it to accumulate in the body.
- Increased absorption of calcium in the intestines.
- Disturbance in the process of calcium absorption by bone tissue.
- Diabetes.
- Heart defects.
- Obesity.
- Unhealthy Lifestyle.
- Heredity.
- Atherosclerosis.
- Rheumatic valvulitis.
Material and methods
The open comparative study included patients aged 50 to 75 years with a high risk of developing cardiovascular complications according to the SCORE scale (more than 5%), atherosclerosis of the brachiocephalic arteries and decreased BMD.
Patients with normal BMD formed the control group. The patients underwent a comprehensive examination of the cardiovascular system at the Scientific Dispensary Department of the National Medical Research Center for Cardiology: general clinical examination, biochemical blood test, study of the levels of 25-hydroxyvitamin D (25 (OH)D) and parathyroid hormone (PTH), OPG, and also applanation tonometry, volumetric sphygmography, dual-energy X-ray absorptiometry (DEXA), multislice computed tomography (MSCT) of the coronary arteries (CA) and thoracic aorta. The study did not include patients with coronary artery disease who had suffered a cerebrovascular accident, transient ischemic attack, as well as those with secondary causes of AP, diabetes mellitus, taking medications that affect bone metabolism, and statins within the last 6 months. A biochemical blood test was performed on an Architect C8000 selective analyzer (Abbot, USA), including determination of total cholesterol (TC), low-density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), triglyceride levels (TG), calcium, phosphorus, creatinine with calculation of glomerular filtration rate (GFR) using the MDRD formula. The content of 25 (OH)D and PTH in the blood plasma was determined by the immunochemical method with electrochemiluminescence detection (ECLIA) on the ELECSYS 2010 analyzer. The concentration of OPG in the blood serum was determined by the enzyme-linked immunosorbent assay (ELISA) in all 68 patients with impaired BMD and in 5 patients with normal BMD. BMD. Applanation tonometry to determine the parameters of central pressure (systolic - SBP, diastolic - DBP and pulse - PBP in the aorta, augmentation index - AI) and pulse wave velocity in the carotid-femoral segment (PWVcf), reflecting the stiffness of the aorta, was performed using the Sphygmocor device (“ AtcorMedical, Australia) using a high-quality Millar applanation sensor using a standard method (direct distance measuring method · 0.8). Pulse wave velocity at the brachiomalleolar segment (PWV) was measured using volumetric sphygmography, which was performed using a VaseraVS-1000 device (FukudaDenshi, Japan). DEXA of the femoral neck (FNC) and lumbar spine to determine BMD was performed using a HologycDiscovery device (USA) according to standard methods. According to the Russian recommendations for the diagnosis and treatment of AP, the diagnosis of “osteopenia” was established when the T-criterion for BMD in the lumbar spine or BBC was from –1 to –2.5 SD, AP – when the T-criterion was –2.5 SD and below. T-scores up to –1 SD from peak bone mass corresponded to normal BMD. To determine the calcium index (CI) of the coronary artery and thoracic aorta, MSCT was performed on a 64-spiral computed tomograph (Toshiba Aquilion, Japan) using a standard patient position on the basis of the tomography department of the National Medical Research Center of Cardiology (headed by Academician of the Russian Academy of Sciences, Prof. S. K. Ternova). CI of the coronary artery and thoracic aorta was assessed from the aortic root (above the origin of the coronary artery) to the apex of the heart according to the standard method. Calculation K.I. were performed according to Agatson using special computer software. For each patient, CI in the coronary artery and thoracic aorta was determined for the area of the calcified area if its density was more than 130 HU. When CI=0, the absence of aortic calcification and CCA was stated. Statistical calculations were carried out using the Statistica 8.0 software package. The main parameters of the studied indicators are presented in the form of a median and values of the lower (25%) and upper (75%) quantiles. A distribution in which the Kolmogorov–Smirnov difference criterion from the theoretically normal Gaussian distribution was more than 0.05 in significance was accepted as normal. Comparison of two groups was carried out using the Mann-Whitney test. Associations between variables were identified using Spearman's correlation coefficient. Differences at p
<0.05 was considered statistically significant.
Research structure.
Based on the results of densitometry in accordance with the T-criterion, patients with a high risk of developing CVD complications were divided into 3 groups: 1st group consisted of 18 patients with normal BMD, 2nd - 48 with osteopenia and 3rd - 20 with O.P. . After further examination, a comparative group analysis was carried out.
Symptoms and degrees of calcification
An increase in the concentration of free calcium in the blood serves as a provoking factor not only for calcification of the heart valves, but also for the development of pathologies such as heart failure, heart attack, and stroke. In this case, the symptoms of calcification are combined with signs of concomitant diseases.
Degree of development of calcification of heart valves
| Degree of disease | Signs of mitral valve pathology | Signs of aortic valve pathology |
| Compensated | An increase in the level of calcium in the blood, calcification of the valves. The tissues are compacted, there is a slight deterioration in hemodynamics | Difficulties arise with the opening of the valves, but the compensation mechanisms of the left ventricle keep the situation under control. During physical activity, minor heart pain is possible, which increases as the disease progresses. |
| Subcompensated | Shortness of breath during physical activity, tachycardia, arrhythmia, wet cough (sometimes with blood clots), hoarseness | Shortness of breath during physical activity, heart pain. Over time, signs of respiratory failure and aortic narrowing occur at rest |
| Decompensated | It develops rarely - with long-term ignoring of symptoms or an avalanche-like progression of the pathology. Pronounced weakness, shortness of breath with little physical activity. Cough with scarlet sputum, pale skin. Requires emergency medical attention | Signs of increased volume of both ventricles. Severe heart failure. The condition is extremely dangerous |
Aortic valve calcification
Patients do not feel any noticeable discomfort for a long time. Signs of pathology appear with stenosis of the aortic valve opening up to half of its passage. The progression of heart failure is accompanied by:
- dizziness;
- angina attacks;
- fainting with a sudden change in body position;
- shortness of breath at night;
- attacks of cardiac asthma and pulmonary edema (in severe cases).
- Aortic valve insufficiency: symptoms, diagnosis, treatment
The combination of heart pain and asthmatic attacks is very unfavorable. If left untreated, aortic valve calcification can cause bleeding in the lower digestive tract. If the valve opening is severely narrowed, sudden cardiac arrest may occur in elderly patients.
Mitral valve calcification
When blood stagnates in the pulmonary circulation, caused by calcification of the mitral valve, respiratory failure occurs, accompanied by characteristic symptoms. In case of serious damage, wheezing and shortness of breath at rest (to alleviate this, you need to sit down with your legs down) are observed, as well as pulmonary edema, characterized by:
- suffocation;
- wet wheezing when breathing;
- chest pain;
- fear of death.
Sometimes pinkish foam appears when exhaling. In such a case, the patient should be seated comfortably, with all the windows in the room opened, and tourniquets applied to his legs. You can hold a cotton swab soaked in alcohol to your nose and offer diuretics. Further therapy should be carried out exclusively in a hospital. Mitral valve calcification is similar in symptoms to signs of cardiosclerosis, rheumatism, and hypertension, so calcification often remains untreated, provoking the development of mitral valve insufficiency and stenosis.
results
Among the patients included in the study, there were 76 (88%) women aged 65 years suffering from hypertension (HTN), with achieved target levels of SBP and DBP (average blood pressure 125/77 mm Hg), hyperlipidemia (TC level 6, 0±1.2 mmol/l). Patients in the comparison groups did not differ in age, gender, smoking status, blood pressure level, heart rate and LDL cholesterol concentration in the blood plasma. At the time of inclusion in the study, patients with hypertension were on selected standard antihypertensive therapy with angiotensin-converting enzyme inhibitors, angiotensin II receptor antagonists, diuretics, and β-blockers (Table 1).
Table 1. Clinical and demographic characteristics of the examined patients in the compared groups Note. Data are presented as median (25th percentile; 75th percentile) or absolute number of patients (%). Differences between groups in all parameters except BMI are statistically insignificant. * — p<0.05 for comparison of the normal BMD group with the osteopenia and OP groups. BMD—bone mineral density; OP - osteoporosis; BMI—body mass index; LDL cholesterol - low-density lipoprotein cholesterol; SBP—systolic blood pressure; DBP—diastolic blood pressure; HR—heart rate; BAB - β-blockers; ACE - angiotensin-converting enzyme; ARBs—angiotensin II receptor blockers.
There were regular statistically significant differences ( p
<0.01 for all groups) for BMD between patients without a decrease in BMD - 1.03 (0.971; 1.098) and 0.998 (0.906; 1.096) g/cm2, with osteopenia - 0.862 (0.823; 0.929) g/cm2, 0.729 ( 0.679; 0.792) and OD - 0.719 (0.652; 0.779) g/cm2 and 0.693 (0.627; 0.767) g/cm2 in the spinal column and lumbar spine, respectively.
The level of OPG did not differ in the compared groups, being 4.7 (3.9; 4.7) pmol/l in the group with normal BMD, 4.9 (3.9; 7) pmol/l in the group with osteopenia and OP 5. 0 (4.2; 6.3) pmol/l. In the correlation analysis, a relationship was observed between the level of OPG and the T-criterion for BMD in the lumbar spine in the examined patients ( r
=–0,28;
p
<0,05).
The levels of SBP and DBP in the aorta in patients with AP were statistically significantly higher than in patients with normal BMD and osteopenia. VA in AP, measured both on the brachial and carotid-femoral segments, was statistically significantly higher than in patients with normal BMD and with osteopenia. AI in patients with AP was statistically significantly higher than in patients with normal BMD (Table 2).
Table 2. VAS parameters in comparison groups Note. Data are presented as median (25th percentile; 75th percentile). The differences are statistically significant (p<0.05) for comparison between groups: * - with AP and normal BMD, ** - with osteopenia and AP. JAS—arterial wall stiffness; BMD—bone mineral density; OP - osteoporosis; cSBP—central systolic blood pressure; cDBP—central diastolic blood pressure; cPAP—central pulse arterial pressure; PWVpl—pulse wave velocity at the brachiomalleolar segment; CAVI (cardio-ankle vascular index) - cardio-ankle vascular index; PWVkf—pulse wave velocity at the carotid-femoral segment; AI—augmentation index.
The presence and severity of disorders of mineral metabolism of bone tissue did not affect the prevalence and severity of CCA and KGOA (Table 3).
Table 3. Severity and frequency of detection of CCA and thoracic aorta in the compared groups Note. Data are presented as median (25th percentile; 75th percentile) or absolute number of patients (%). The differences between the three groups are not statistically significant. BMD—bone mineral density; OP - osteoporosis; CCA—coronary artery calcification; KGOA - calcification of the thoracic aorta; CI—calcium index; CA - coronary arteries.
Patients with CCA, compared with patients without it, were statistically significantly older and had higher central SBP and PBP, SBP on the brachial artery and VA, assessed using PWVp, including an indicator that does not depend on the level of blood pressure - CAVI (cardio -ankle vascular index) - cardio-ankle vascular index, as well as a higher risk of major fractures and fractures of the ankle joint (Table 4).
Table 4. Comparative characteristics of the studied parameters in patients with and without CCA Note. Data are presented as median (25th percentile; 75th percentile). CCA—coronary artery calcification; SBP—systolic blood pressure; DBP—diastolic blood pressure; PAP—pulse arterial pressure; PWVpl—pulse wave velocity at the brachiomalleolar segment; CAVI (cardio-ankle vascular index) - cardio-ankle vascular index; PWVkf—pulse wave velocity at the carotid-femoral segment; 25 (OH)D - 25-hydroxyvitamin D; GFR—glomerular filtration rate; OPG—osteoprotegirin; SHB - neck of the femur.
The presence of aortic calcification was associated with older age, higher PWVpl, CAVI, OPG level, lower GFR, and, in addition, with the risk of major fractures and BCS fractures (Table 5).
Table 5. Comparative characteristics of the studied parameters in patients with CHOA and without calcification Note. Data are presented as median (25th percentile; 75th percentile). KGOA - calcification of the thoracic aorta; PWVpl—pulse wave velocity at the brachial-ankle segment; CAVI (cardio-ankle vascular index) - cardio-ankle vascular index; 25 (OH)D - 25-hydroxyvitamin D; GFR—glomerular filtration rate; OPG—osteoprotegirin; SHB - neck of the femur.
In the general group of patients, positive correlations were observed between the severity of CCA and age, levels of SBP in the brachial artery and aorta, aortic PBP, VA parameters - PWVp and CAVI. In the group of patients with osteopenia, in addition to the indicated relationships, a correlation of CI in the coronary artery with PWVcf was revealed. Similar relationships with the studied parameters of central blood pressure and blood pressure were also observed for the severity of aortic calcification. The severity of CCA was greater, the lower the level of 25 (OH)D in the blood. In patients with AP, the severity of CCA was associated with higher levels of parathyroid hormone ( r
=–0.45;
p
<0.05).
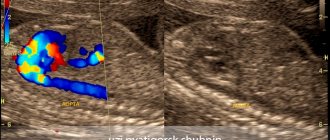
There was a negative correlation between the severity of CCA and GFR (Table 6; see Table 6. Correlation of the severity of CCA with the studied parameters in the examined patients. Note: CI - calcium index; CA - coronary arteries; SBP - systolic blood pressure; DBP - diastolic blood pressure; PAP - pulse arterial pressure; PWVp - pulse wave velocity in the brachial-ankle segment; CAVI (cardio-ankle vascular index) - cardio-ankle vascular index; 25 (OH)D - 25-hydroxyvitamin D; GFR - glomerular filtration rate; OPG — osteoprotegirin; ShBK — femoral neck. picture).
Relationship between OPG level and CI of the thoracic aorta.
Causes of the disease
The main causes of calcification of the valvular apparatus of the heart include:
- pathologies of the endocrine system;
- serious disturbances in intestinal activity, accompanied by decreased calcium absorption;
- hereditary disposition;
- negative changes in the activity of the kidneys, which ensure the utilization of microelement salts;
- rheumatism of the heart;
- endocarditis (inflammation of the inner lining of the heart muscle);
- hypertension;
- structural abnormalities of blood vessels;
- congenital heart defects (aortic stenosis, bicuspid aortic valve).
Additional risk factors that aggravate metabolic disorders and provoke the development of valve calcification are:
- bad habits;
- overweight;
- psycho-emotional overload;
- excess vitamin D;
- cancerous tumors;
- injuries of bones and soft tissues.
Often, calcification of the heart valves is combined with atherosclerosis.
Treatment of aortic calcification
Important for the success of treatment are determining the root cause of metabolic disorders and correcting the impact of negative factors. First of all, this is a change in diet and lifestyle. Drug therapy is aimed at improving blood circulation to prevent disruptions in the functioning of vital organs. Often the initial cause of the accumulation of calcium salts is increased cholesterol levels and the formation of atherosclerotic plaques. In this case, all means of treating atherosclerosis are used.
With calcinosis, complications may arise and symptoms of cardiac dysfunction may appear, then appropriate medications are prescribed:
- reducing blood pressure;
- improving blood circulation and relieving congestion;
- drugs that reduce blood thickness;
- remedies for ischemia and arrhythmia.
In advanced conditions, when treating aortic calcification with medications is ineffective, surgical intervention is used. This can be an open operation with cleaning of the vascular walls or manipulation using a catheter, as well as bypass surgery and prosthetics.
Symptoms of limescale formation
Despite the fact that calcification is quite common, its intravital diagnosis is difficult. There are no specific signs for this pathology, so it is mistaken for rheumatism, post-infarction cardiosclerosis, the consequences of the inflammatory process and hypertension.
Clinical symptoms that may occur when heart valves are desiccated include:
- the formation of an acquired defect of the mitral or aortic valve - calcification is likely after excluding rheumatism, endocarditis, and autoimmune diseases;
- murmur when listening to the heart in the absence of a defect, occurs during systole or diastole, rough;
- impaired conduction of impulses and myocardial excitability in the form of atrial fibrillation or blockade of the legs of His; with mitral calcinosis, complete atrioventricular block against the background of atrial flutter (Frederick's syndrome) often occurs;
- extrasystole, paroxysmal ventricular tachycardia;
- valve prolapse;
- heart failure (shortness of breath, tachycardia, swelling in the legs, severe weakness) in the absence of underlying diseases;
- formation of intracardiac blood clots with subsequent blockage of blood vessels.
- Aortic heart defects: causes, diagnosis and treatment
Changes in myocardial conductivity are explained by the fact that the valve leaflets pass into the septum between the ventricles, in which the cells of the conduction system are located. Valve calcification may also be accompanied by an inflammatory reaction of tissues, which spreads to neighboring areas of the heart.
The most common clinical form of aortic calcification is progressive valve stenosis. It is accompanied by the following symptoms:
- fast fatiguability;
- shortness of breath with slight exertion;
- feeling of strong and rapid heartbeat;
- dizziness;
- fainting conditions;
- heartache;
- attacks of suffocation at night;
- swelling;
- pain in the liver area.
Complications of stenosis include acute circulatory failure (cardiac asthma, cardiogenic shock, pulmonary edema), endocarditis, cerebral ischemia (transient attacks or stroke), complete blockade of impulse conduction, severe angina and myocardial infarction.
Folk remedies to help
Treatment with folk remedies is one of the ways to correct the disease and stabilize the level of calcium in the blood. Calcification is a consequence of the failure of metabolic processes occurring in the body. This is why it is quite logical that without a proper diet this cannot be advice.
The patient should limit the consumption of foods rich in this mineral. It should be excluded from the daily diet:
- dairy products;
- Herbs and most vegetables;
- Spicy dishes;
- smokes;
- sweets;
- cocoa;
- yeast products;
- Spices and spices.
The diet consists of consuming foods rich in magnesium. These:
- Porridge - buckwheat, oatmeal, barley, millet
- Leggear Boats - peas, beans.
- Brussels sprouts.
- Nuts - cashews, pine nuts, hazelnuts, peanuts.
Eating suitable foods helps reduce calcium levels and indicate balance.
Therapeutic infection can be used to clear plaque from blood vessels:
- Chamomile, English herbs and birch donuts will be needed for preparation. All 100 grams. All ingredients are crushed and mixed.
- Take 500 ml of boiling water and 1 tablespoon of this herbal harvest and mix everything.
- Leave this “cocktail” for 30 minutes. It is then filtered and divided into half: drink 1 tablespoon in the morning and evening. The duration of treatment is 14 days.
Diagnostic measures
It is extremely difficult to diagnose heart valve calcification, especially stage 1 of its development. Doctors are trying to visualize the cavities of the heart muscle. The most effective methods include:
- Ultrasound of the heart;
- cardiac catheterization;
- radiography;
- ventriculography;
- aortography;
- two-dimensional echocardiography;
- ELCG (electrocoagulography);
- ultrasonic densitometry.
More reliably and more often, calcification of the heart valves is detected using an electron-optical amplifier and X-ray television.
Diagnosis of aortic stenosis
If symptoms of aortic stenosis appear, you should contact a cardiologist or begin an examination with a general practitioner. Using a stethoscope, the doctor will listen for a murmur over the aorta as the left ventricle contracts. An electrocardiogram can reveal ventricular hypertrophy. Ventricular enlargement can also be detected using x-ray. An echocardiogram uses ultrasound to evaluate the condition of the valves and heart muscle.
Also, an information research method is cardiac catheterization (insertion of a catheter into an artery). Provides information about intracardiac pressure, the location of the narrowing, the concentration of oxygen in the blood, the condition of the valve and the presence of a defect.
The most informative diagnostic method for making a decision on surgical intervention is an angiocardiographic study. It takes place in two stages: ventriculography and oorthography.
Author of the article:
Mochalov Pavel Alexandrovich |
Doctor of Medical Sciences therapist Education: Moscow Medical Institute named after. I. M. Sechenov, specialty - “General Medicine” in 1991, in 1993 “Occupational diseases”, in 1996 “Therapy”. Our authors
Calcification of the aortic walls: therapeutic diet
Conservative treatment will not be effective without following a special diet aimed at normalizing metabolic processes. Specific recommendations should be developed by the attending physician, taking into account the medical history and the reasons that caused the pathology. But there are a number of general principles for developing a diet for aortic calcification:
- Avoid foods rich in calcium.
- Consumption of foods containing magnesium.
- Limit salt.
- Reduce calories.
- Avoid fatty and fried foods.
Prohibited foods for aortic calcification include dairy products, fatty meats, spices, yeast baked goods, desserts, herbs, and cocoa. It is recommended to consume bran, nuts, buckwheat and barley. It is also necessary to strictly monitor the amount of food eaten, avoid excess weight and lead an active and healthy lifestyle.