Atherosclerosis and narrowing (stenosis) of the renal artery can lead to several different clinical syndromes, ranging from difficult-to-control hypertension to recurrent pulmonary edema (shortness of breath due to fluid filling of the lungs), ischemic nephropathy (kidney dysfunction due to impaired arterial blood flow) and renal failure . Renal artery stenosis most often occurs due to the buildup of atherosclerotic plaque in the renal arteries (usually in people over 50 years of age), but can be caused by fibromuscular dysplasia, more commonly seen in women under 50 years of age.
Renal artery stenting is a procedure to open the renal arteries (large blood vessels that carry blood to the kidneys) when they are blocked by atherosclerotic plaque. Stenting allows you to restore normal blood flow. Balloon-expandable stents are most often used for this procedure. The stenting procedure allows you to restore the patency of the vessel without damaging the tissue, quickly and painlessly.
Preparing for treatment
If your stent surgery is scheduled for the morning, do not eat or drink after midnight (you can take the medicine with a sip of water in the morning). If the procedure takes place in the afternoon, do not eat after 10 am.
Tell your doctor about all the medications you take; about pregnancy; about allergies and sensitivities to medications, local anesthesia, latex, contrast dye, or iodine.
You may have a blood test to determine how long it takes for your blood to clot.
Diagnostic tests should be performed to determine whether renal artery stenting is required in this case. Among these tests:
- Angiography. During this test, a catheter is inserted through the groin into the aorta. The study allows you to see how well blood flows through the renal vessels and detect any other vascular pathology.
- Magnetic resonance angiography. This test is similar to a regular magnetic resonance imaging scan, which uses a large magnet to create images inside the body. In magnetic resonance angiography, contrast dye is injected into the blood to better visualize the vessels.
- Computed tomographic angiography. Uses a series of cross-sectional X-rays to create a three-dimensional image of the inside of the body. In our clinic, this is an indispensable method of accurate diagnostics, allowing us to accurately diagnose the pathology of the renal vessels and determine the indications for stenting.
- Duplex Doppler ultrasonography. This test uses sound waves to measure the size of the narrowed area and the speed of blood flow in the renal arteries.
Diagnosis of arterial renal anomalies
To identify the nature of arterial stenosis and the degree of narrowing of the vessel, various methods of examining the kidney are used:
· General blood and urine tests.
· Biochemistry of blood.
· Doppler ultrasound of the kidney (ultrasound studies the blood flow - its acceleration in the stenotic area - using color Doppler mapping).
· Angiography (study of blood flow by injecting a contrast agent into an artery).
· Scintigraphy (radioisotope method for studying the renal vessel).
· CT, MRI.
When using an angiographic technique, the doctor sees the pathological area of the vessel and can assess the degree of narrowing or widening of the artery walls, and determine all the necessary parameters of the renal artery anomalies.
Angiography is a very informative diagnostic method, but today visualization of large renal vessels through the use of multislice CT or MRI is a more informative and less invasive technique.
Possible complications
Restenosis is more common in people whose renal vessels were very narrow to begin with, in patients over 65 years of age, women and smokers. Sometimes another stenting procedure may be needed to re-unblock the artery.
Risks of renal artery stenting include:
- Bruising in the area where the catheter was inserted
- Bleeding at or around the injection site,
- Damage to the vessel
- Thrombosis,
- An allergic reaction to the dye used during the procedure,
- Stent displacement
- Kidney failure
- Urinary tract infection.
Causes of development of renal artery stenosis
Among the diseases that provoke renal artery stenosis, the most common are atherosclerosis and fibromuscular dysplasia .
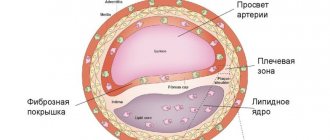
Atherosclerotic, that is, accompanied by the formation of plaques in the arteries from pieces of tissue detached from the walls, renal artery stenosis is usually a companion to diabetes mellitus, coronary heart disease or arterial hypertension.
In this case, plaques in most cases are concentrated in the area of the aorta, which is fraught with the most severe consequences for the patient.
Fibromuscular dysplasia as a cause of stenosis is often a hereditary pathology and is much more common in women aged 30-45 years. This disease is a thickening of fibrosis or muscle tissue covering the tissue of artery walls.
In some cases, renal artery stenosis can be provoked by arterial aneurysms, arteriovenous shunts, nonspecific aortoarteritis, thrombosis or embolism of the renal arteries, compression of the renal vessels by a foreign body or tumor, and nephroptosis.
Observation after treatment
Call your doctor if you have:
- Fever,
- Breathing problems
- Rash,
- The area where the catheter was inserted becomes red, swollen and painful, or oozes blood.
- Pain in the abdomen or side on the side of the treated kidney.
- Very low pressure.
After renal artery stenting, you should avoid vigorous physical activity for at least 24 hours and drink plenty of fluids to wash out the contrast dye.
You can perform light activities the next day, but should avoid heavy physical labor or strenuous activities for five days. Stenting of the renal arteries is a modern high-tech method for the treatment of renovascular hypertension and is significantly superior in safety to open interventions on these vessels.
Symptoms
Signs of arterial pathologies may vary for different anomalies.
For example, the main signs of stenosis (the most common pathology of the artery in the kidney - up to 2/3 of all cases of such kidney diseases), in addition to high blood pressure, are:
· Pain: headache, behind the sternum, in the lower back, in the eyes.
· Feeling of noise in the ears.
· Shortness of breath.
· Tachycardia.
· Presence of a small amount of protein in the urine.
· Uneven pressure on the right and left sides of the body.
The presence of aneurysm may have no symptoms at all until the dilation becomes very large or the aneurysm ruptures. If the dilatation is large, the ureter is compressed, the functioning of the kidney is significantly impaired, and infection with urinary toxins occurs. There is weakness, headache, and the smell of acetone.
When an aneurysm ruptures, the renal artery becomes blocked. If the patient is not immediately taken to the vascular surgery department, there is a high risk of death.
Treatment of major renal vascular abnormalities
Stenosis, the basic symptom of which is very high blood pressure, requires complex drug therapy. Typically these are blood pressure lowering drugs and diuretics.
The use of medications, as a rule, is additional to surgical techniques , since the very cause of the disease does not eliminate the use of drugs, and the disease progresses. Stenosis confirmed by diagnostic measures is an indication for surgical intervention. Most often these are the following operations:
· Shunting . Shunts create blood flow that bypasses the pathological area of the artery.
· Angioplasty . An inflating balloon is inserted into the artery to widen it.
· Stenting. The vessel is expanded with stents - springy or mesh devices.
· Prosthetics . The operation is performed if it is impossible to perform angioplasty or stenting. The narrowed area is excised and an implant is placed in its place.
· Nephrectomy . During this operation, the indication for which is multiple stenosis, a practically non-functioning kidney is removed.
If stenosis is not treated, a third of patients are likely to die from strokes, heart attacks, and acute renal failure.
If an aneurysm , surgery is usually performed. In the most severe cases, the kidney is removed. But if the aneurysm does not grow, doctors resort not to open traditional operations, but to minimally invasive techniques. For example, during obliteration, a catheter with a special substance is inserted into the aneurysm, which immediately hardens, “bricking up” the pathological section of the artery.
Publications in the media
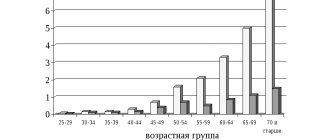
Vasorenal arterial hypertension (AH, renovascular hypertension) is symptomatic (secondary) hypertension caused by ischemia of the kidney(s) due to narrowing of the renal artery or its branches, rarely due to bilateral damage. Statistical data. The prevalence is 1–2% (up to 4–16% according to specialized clinics) among all types of hypertension.
Etiology
• The most common cause of renal artery stenosis is atherosclerosis (reported among all types of renal artery stenosis in 62%). Localization of atheromatous plaques •• Proximal segments of the renal artery near the aorta (74% of cases) •• Middle segments of the renal artery (16% of cases) •• Near the bifurcation of the renal artery (5% of cases) •• Distal branches of the renal artery (5% of cases).
• Less commonly (in 24% of patients), a congenital disease is noted - fibromuscular dysplasia. The lesion is localized in the middle third of the renal artery. The following types of process are distinguished: •• Proliferation of the inner membrane ••• Primary ••• Secondary •• Dysplasia of the middle layer ••• Hyperplasia of the middle layer ••• Perimedial fibrous dysplasia ••• Dysplasia with the formation of microaneurysms ••• Dissection of the middle layer •• Subadventitial fibroplasia.
• Other types of stenotic lesions of the renal arteries are observed in 6% of cases •• Congenital artery stenosis (the most common cause of hypertension in children) •• Renal artery aneurysm •• Traumatic thrombosis and embolism •• Coarctation of the aorta with renal artery stenosis •• Nonspecific aortoarteritis •• Compression of the vascular pedicle of the kidney from the outside by a tumor or foreign body.
Pathogenesis
• Constriction of the renal artery activates the juxtaglomerular apparatus due to a decrease in blood pressure in the poststenotic segment, which leads to the release of renin, and a decrease in sodium concentration in the nephron loop.
• Renin converts angiotensinogen coming from the liver into angiotensin I, which is converted under the influence of ACE into angiotensin II, which directly affects systemic arterioles and sharply increases peripheral resistance.
• Indirectly through the adrenal cortex, angiotensin II leads to hyperaldosteronism, sodium retention in the body and an increase in extracellular fluid volume.
• The results of surgical treatment are largely determined by whether one or both renal arteries are affected •• With unilateral stenosis, the cause of hypertension is the renopressor mechanisms of the ischemic kidney. However, over time, the contralateral intact kidney will switch to a new blood pressure regime and will maintain hypertension even when the original source of hypertension is removed or revascularized •• With bilateral renal artery stenosis, its gradual elimination usually leads to a decrease in blood pressure. The same is observed during revascularization of a single kidney.
Clinical manifestations
• Renal artery stenosis can be suspected when hypertension occurs unexpectedly or when previously benign hypertension suddenly worsens. Arterial hypertension occurs before age 30 or after age 50, usually in the absence of a family history of hypertension. Characterized by rapid progression of hypertension, high blood pressure, rapid target organ damage, and resistance to treatment.
• Complaints •• Characteristic of cerebral hypertension - headaches, a feeling of heaviness in the head, hot flashes, tinnitus, pain in the eyeballs, memory loss, poor sleep, irritability, flashing “floaters” before the eyes •• Associated with overload of the left parts of the heart and relative or true coronary insufficiency - pain in the heart, palpitations, shortness of breath, a feeling of heaviness in the chest •• Caused by urological pathology - a feeling of heaviness, or dull pain in the lumbar region, and in the case of a kidney infarction - hematuria •• Caused by ischemia of others organs, the main arteries of which can be affected simultaneously with the renal arteries ••• Symptoms of ischemia of the gastrointestinal tract ••• Ischemia of the upper or lower extremities ••• Signs of cerebral atherosclerosis •• Signs of an inflammatory reaction (with nonspecific aortoarteritis) •• Complaints typical for secondary hyperaldosteronism - muscle weakness, paresthesia, attacks of tetany, isohyposthenuria, polydipsia, nocturia.
• As with any renal hypertension, high levels of diastolic blood pressure are characteristic, reaching in some cases 170 mm Hg.
• Systolic murmur in the right or left upper quadrant of the abdomen and along the posterior wall of the chest. The murmur is usually low-intensity, in contrast to the murmur heard with arteriovenous fistula of the kidney or atherosclerosis of the abdominal aorta (rough and prolonged).
Laboratory and instrumental data
• Hypokalemia (due to excessive secretion of aldosterone).
• Determination of plasma renin activity, especially in combination with the captopril test (100% sensitivity and 95% specificity): an increase in plasma renin activity after taking captopril by more than 100% of the initial value indicates pathologically high renin secretion, and is a sign of renovascular hypertension
• X-ray contrast angiography is the “gold standard” in the diagnosis of renal artery stenosis. The transfemoral Seldinger method is preferable: stenosis of the renal artery and (distal to it) its fusiform expansion are detected •• With nephroptosis, the renal artery is tense, it departs from the aorta at an acute angle, its diameter is narrowed •• With atherosclerosis of the renal artery, the filling defect is most often located near the mouth renal artery. Often, an angiogram reveals signs of atherosclerosis of the aorta •• With fibromuscular dysplasia, a multifocal narrowing of the renal artery is determined, in most cases starting at a distance of 2 cm distal to the origin of the artery from the aorta •• With nonspecific aortoarteritis, weaselation of the walls of the abdominal aorta is found along with narrowing of the renal artery. Stenotic lesions of other branches of the aorta are often determined •• In case of thrombosis or embolism of the renal artery, the symptom of a “blind ending” of the trunk of the renal artery or one of its main branches is determined •• In case of an aneurysm of the renal artery, its saccular or fusiform expansion is located mainly in the area of the renal hilum. The walls of the aneurysm often become calcified.
• Asymmetry of the kidneys on ultrasound.
• Doppler study of the renal arteries - acceleration of blood flow and its turbulence.
• Renal scintigraphy - decreased drug absorption, decreased drug delivery to the affected kidney, asymmetry of renographic curves. The optimal combination of renal scintigraphy and captopril at a dose of 25–50 mg orally. When taking captopril, the entry of the isotope into the kidney tissue decreases. A normal renal scintigram after taking captopril excludes hemodynamically significant renal artery stenosis.
• Excretory urography: the intensity of concentration of the contrast agent and the time of its appearance on the urogram may be reduced, as well as a decrease in the size of the kidney; however, the excretory urogram may remain normal, so the final diagnosis requires confirmation by aortography.
• MRI of the renal arteries is a modern method for verifying renovascular hypertension.
Differential diagnosis • Primary aldosteronism • Pheochromocytoma • Cushing's syndrome • Coarctation of the aorta • Diseases of the renal parenchyma, leading, for example, to chronic renal failure.
TREATMENT
General tactics. First of all, it is necessary to consider the possibility of radical treatment - percutaneous transluminal renal angioplasty, stenting of a stenotic artery, or radical surgical treatment. If such treatment is impossible or there are contraindications to it, drug therapy is prescribed.
Drug therapy is auxiliary, because a decrease in blood pressure with renal artery stenosis is non-physiological (leads to decompensation of blood circulation in the kidney and its shrinkage).
• Indications for long-term treatment are older age and systemic damage to the arterial bed, including the coronary arteries.
• Drugs of choice are ACE inhibitors, such as captopril. Additionally, other antihypertensive drugs are prescribed (see Arterial hypertension). Treatment begins with minimal doses of short-acting ACE inhibitors (for example, captopril at a dose of 6.25 mg). In the absence of collapse, the dose of captopril is increased or long-acting ACE inhibitors are prescribed. Monitoring of creatinine and GFR levels is necessary. ACE inhibitors are contraindicated in bilateral renal artery stenosis.
Balloon dilatation of the renal arteries
• Opinions about its effectiveness are controversial. In any case, this method is a good prognostic criterion for subsequent surgery: if after adequate dilatation even temporary normalization of blood pressure occurs, we can talk about a direct dependence of hypertension on renal artery stenosis.
• Indications •• Therapy-resistant hypertension in patients over 60 years of age with angiographically detected stenosis of the renal arteries •• Risk factors (stenosis of the carotid, coronary arteries, cardiac and respiratory failure) •• Renal failure caused by stenosis of the renal arteries •• Restenosis of the renal arteries after their revascularization or kidney transplantation •• As a diagnostic procedure to determine the relationship between renal artery stenosis and hypertension.
Surgery
• Organ-sparing operations •• Resection of the renal artery with reimplantation into the aorta •• Resection with end-to-end anastomosis •• Transaortic endarterectomy •• Autoplasty of the renal arteries with free grafts •• Creation of a splenorenal anastomosis •• Plastic surgery of the renal artery with synthetic antithrombogenic prostheses.
• Nephrectomy - if it is impossible to perform reconstructive surgery on the artery (the share of nephrectomies in the total number of operations is 16–20%).
• Contraindications •• Bilateral extended damage to the renal arteries •• Shrinkage of both kidneys •• Myocardial infarction and the period up to 6 months after it •• acute cerebrovascular accident •• End-stage chronic renal failure.
• Postoperative complications •• Internal bleeding •• Thrombosis of vascular anastomoses •• AKI.
• Results of operations •• Mortality is 0–6% •• Positive results with atherosclerosis of the renal artery are noted in 63% of patients, with fibromuscular dysplasia - in 73% •• The period of normalization of blood pressure after surgery can last up to 6 months.
• Postoperative management. Dispensary registration is recommended for patients. For residual hypertension, antihypertensive drugs are prescribed.
Reduction. AH - arterial hypertension.
ICD-10 • I15.0 Renovascular hypertension