Arrhythmia is diagnosed when the regularity of contractions of the heart muscle is disrupted. The most common type of arrhythmia is tachycardia, which can be caused in the ventricles of the heart (ventricular arrhythmia) or in the atria (supraventricular arrhythmia). What are the symptoms of arrhythmia? What is the removal procedure? Arrhythmia is not an isolated disease. This term describes a heart rhythm disorder that can cause the heart to beat too fast, too slow, or irregularly. In other words, the heart rhythm may be disrupted. An abnormal heart rhythm can be a symptom of cardiovascular disease (coronary heart disease, heart valve disease, hypertension) or the effect of disorders such as hormonal or electrolyte imbalances. Therefore, the patient needs to find out the causes of the arrhythmia and, if they require treatment, undergo appropriate therapy.
How does arrhythmia occur?
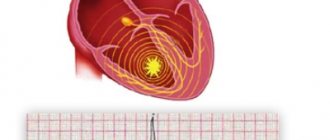
To understand the mechanism of arrhythmia, it is necessary to recall basic information about the structure and function of the heart in the body. This organ consists of two atria and two ventricles, which contract and relax in a strictly defined rhythm. Thanks to these movements, blood is constantly pumped into every cell of the body, providing it with nutrients and oxygen. But what makes the heart beat so regularly? The heart is equipped with a natural "pacemaker", that is, the sinus node, located in the right atrium. It is thanks to him that the heart “beats” even when it is removed from the chest. The sinus node produces electrical impulses that move the entire muscle. The work of the heart is a series of complex bioelectrical processes that occur in each of its cells. Cardiac arrhythmias occur when abnormalities occur at some point in this complex process. The pulse source may fail or problems may arise at the conduction stage. In both cases, arrhythmia will occur.
Prevention
- Elimination of cardiac pathology.
- Exclusion of extracardiac factors of arrhythmia or blockade (intoxication, autonomic dysfunction, stress, etc.).
- Limit intake of caffeine-containing products and alcohol.
We will help make a diagnosis at an early stage of the development of blockade, tachycardia or other disorders and provide timely treatment for cardiac arrhythmia. Further observation will allow maintaining a good quality of life. For questions regarding the treatment of cardiac arrhythmia in Moscow, please contact us by dialing the number +7.
Types of arrhythmias
There are many types of arrhythmias, as well as divisions in medicine depending on the accepted classifications. The most common forms of cardiac arrhythmia include:
- sinus tachycardia,
- bradycardia,
- atrial fibrillation,
- ventricular fibrillation,
- additional supraventricular and ventricular contractions,
- tachycardia: supraventricular and ventricular.
Each of these disorders is actually a separate disease that has different causes and also requires different treatments.
Symptoms of arrhythmia
The most common symptoms of arrhythmia include:
- fast or irregular heartbeat,
- tachycardia,
- bradycardia,
- strong heartbeat,
- feeling of lumps in the chest,
- dyspnea,
- chest pain,
- heat,
- weakness,
- fainting.
Ventricular arrhythmia
Ventricular arrhythmia is one of the most common. Their classification includes: ventricular tachycardia, flutter and ventricular fibrillation and accelerated ventricular rhythm. The older the patient and the more damaged the heart, the more often they occur.
Ventricular Arrhythmia - Cardiac Factors Factors that cause or exacerbate ventricular arrhythmia can be classified as cardiac or non-cardiac. When this type of arrhythmia occurs, the following cardiac factors are especially likely:
- cardiac ischemia,
- cardiomyopathy,
- congenital long QT syndrome,
- Brugada syndrome,
- mitral valve prolapse.
Ventricular arrhythmia - non-cardiac factors Non-cardiac factors include disorders such as:
- polymyositis,
- sarcoidosis,
- amyloidosis,
- diseases of the nervous system,
- hormonal disorders,
- metabolic disorders,
- electrolyte disturbances.
In addition, the condition is affected by the use of stimulants (coffee, smoking, alcohol).
What are the symptoms of ventricular arrhythmia?
Symptoms of ventricular arrhythmia depend on the type of arrhythmia. In mild forms, patients may not experience arrhythmias. Palpitations may be accompanied by chest discomfort and anxiety. In complex disorders (ventricular tachycardia, ventricular flutter, ventricular fibrillation), shortness of breath, loss of consciousness and sudden cardiac arrest occur.
REASONS FOR THE DEVELOPMENT OF PAROXYSMAL VENTRICULAR TACHYCARDIA
Reasons for the development of PVT:
1. severe diseases of the cardiovascular system:
- myocardial infarction
- cardiomyopathy
- heart defects
- heart failure
- myocarditis (severe)
2. toxic factors:
- frequent alcohol consumption in significant quantities
- inhalation of glue fumes
- narcotic substances
3. cardiac injury
4. medications: cardiac glycosides, antidepressants, flecainide, fluoroquinolones
5. congenital anomalies of the cardiac conduction system (Brugada syndrome)
6. idiopathic VT – the cause of development is unclear
What tests should be taken for ventricular arrhythmia?
To correctly identify ventricular arrhythmia and accurately differentiate the type of ventricular arrhythmia, it is necessary to perform an ECG. If arrhythmia occurs intermittently, perform a Holter test (24-hour ECG recording). You can also monitor your heart rate for longer, such as three days or even 2-3 weeks. In this case, it is necessary to wear an Event-Holter device, which the patient activates only when symptoms appear, such as:
- cardiopalmus,
- deterioration of health,
- dizziness.
An invasive electrophysiological study is performed when the site of ventricular arrhythmia is identified and an attempt is made to destroy the arrhythmogenic focus. The following methods are used in the treatment of ventricular arrhythmias:
- antiarrhythmic drugs,
- percutaneous high-frequency ablation,
- implantation of a cardioverter-defibrillator.
The doctor decides what treatment to take when he determines what type of ventricular arrhythmia the patient has.
LITERATURE
- Peppard PE, Young T, Barnet JH, et al. Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 2013. 177(9):1006-1014. doi: 10.1093/aje/kws342
- Marin JM, Carrizo SJ, Vicente E., Agusti AG Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005. 365(9464):1046-1053. doi: 10.1016/S0140-6736(05)71141-7
- Guilleminault C., Connolly SJ, Winkle RA Cardiac arrhythmia and conduction disturbances during sleep in 400 patients with sleep apnea syndrome. Am. J. Cardiol. 1983. 52(5):490-494. doi: 10.1016/0002-9149(83)90013-9
- Vizzardi E., Sciatti E., Bonadei I., et al. Obstructive sleep apnoea-hypopnoea and arrhythmias: new updates. J. Cardiovasc. Med. 2017. 18(7):490-500. doi: 10.2459/JCM.0000000000000043
- Pevzner A.V., Bayrambekov E.Sh., Litvin A.Yu. et al. Results of the use of therapy with the creation of continuous positive air pressure in the upper respiratory tract in the treatment of patients with atrial fibrillation and obstructive sleep apnea syndrome. Russian Journal of Cardiology. 2021. (7):111-116. https://doi.org/10.15829/1560-4071-2017-7-111-116
- Kirchhof P, Benussi S, Kotecha D, et al. ESC Scientific Document Group. 2021 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016. 37(38):2893-2962. doi: 10.1093/eurheartj/ehw210.
- Raghuram A., Clay R., Kumbam A., et al. A systematic review of the association between obstructive sleep apnea and ventricular arrhythmias. J. Clin. Sleep Med. 2014.10(10):1155-60. doi: 10.5664/jcsm.4126
- Almeneessier AS, Alasousi N, Sharif MM, et al. Prevalence and Predictors of Arrhythmia in Patients with Obstructive Sleep Apnea. Sleep Sci. 2021. 10(4):142-146. doi: 10.5935/1984-0063.20170025
- Tsareva V.M., Novitsky N.I. The relationship between ventricular arrhythmias and sleep-disordered breathing in postmenopausal women with coronary artery disease. Transbaikal Medical Bulletin. 2021. (3): 78-86.
- May AM, Van Wagoner DR, Mehra R. OSA and Cardiac Arrhythmogenesis: Mechanistic Insights. Chest. 2021. 151(1):225-241. doi: 10.1016/j.chest.2016.09.014
- Selim BJ, Koo BB, Qin L, et al. The Association between Nocturnal Cardiac Arrhythmias and Sleep-Disordered Breathing: The DREAM Study. J. Clin. Sleep Med. 2021. 12(6):829-837. doi: 10.5664/jcsm.5880
- Shepard JW Jr, Garrison MW, Grither DA, Dolan GF. Relationship of ventricular ectopy to oxyhemoglobin desaturation in patients with obstructive sleep apnea. Chest. 1985. 88(3):335-40. doi: 10.1378/chest.88.3.335
- Ryan CM, Juvet S, Leung R, Bradley TD. Timing of nocturnal ventricular ectopy in heart failure patients with sleep apnea. Chest. 2008. 133(4):934-40. doi: 10.1378/chest.07-2595
- Marinheiro R, Parreira L, Amador P, et al. Ventricular Arrhythmias in Patients with Obstructive Sleep Apnea. Curr Cardiol Rev. 2019;15(1):64-74. doi: 10.2174/1573403X14666181012153252
- Roche F, Xuong AN, Court-Fortune I, et al. Relationship among the severity of sleep apnea syndrome, cardiac arrhythmias, and autonomic imbalance. Pacing ClinElectrophysiol. 2003. 26(3):669-77. doi: 10.1046/j.1460-9592.2003.00116.x
- Mehra R, Benjamin EJ, Shahar E, et al. Sleep Heart Health Study. Association of nocturnal arrhythmias with sleep-disordered breathing: The Sleep Heart Health Study. Am. J. Respira. Crit. Care Med. 2006. 173(8):910-916. doi: 10.1164/rccm.200509-1442OC
- Patil SP, Ayappa IA, Caples SM, et al. Treatment of Adult Obstructive Sleep Apnea with Positive Airway Pressure: An American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2021. 15(2):335-343. doi: 10.5664/jcsm.7640
- Harbison J, O'Reilly P, McNicholas WT. Cardiac rhythm disturbances in the obstructive sleep apnea syndrome: effects of nasal continuous positive airway pressure therapy. Chest. 2000.118(3):591-595. doi: 10.1378/chest.118.3.591
- Seyis S, Usalan AK, Rencuzogullari I, et al. The Effects of Continuous Positive Airway Pressure on Premature Ventricular Contractions and Ventricular Wall Stress in Patients with Heart Failure and Sleep Apnea. Can Respir J. 2021. 2021:2027061. doi: 10.1155/2018/2027061
- Craig S, Pepperell JC, Kohler M, et al. Continuous positive airway pressure treatment for obstructive sleep apnoea reduces resting heart rate but does not affect dysrhythmias: a randomized controlled trial. J Sleep Res. 2009 Sep;18(3):329-36. doi: 10.1111/j.1365-2869.2008.00726.x
- Roche F, Barthélémy JC, Garet M, et al. Continuous positive airway pressure treatment improves the QT rate dependence adaptation of obstructive sleep apnea patients. Pacing ClinElectrophysiol. 2005. (8):819-825. doi: 10.1111/j.1540-8159.2005.00188.x
Supraventricular arrhythmia
Atrial fibrillation and atrial flutter is one of the types of supraventricular arrhythmia. The most common symptoms include rapid heartbeat, shortness of breath, and even fainting. The best results are achieved by combining pharmacological treatment with diagnostic procedures. Supraventricular cardiac rhythm disturbances are caused by electrical impulses originating in the sinus node or atrioventricular focus.
Supraventricular arrhythmia - types
Supraventricular arrhythmias include:
- additional, single stimulation,
- supraventricular tachycardia,
- pre-excitation syndromes,
- atrial tachycardia,
- atrial fibrillation,
- atrial flutter,
- sinus tachyarrhythmias.
Supraventricular arrhythmia - symptoms
Each of the arrhythmias listed above has different causes and symptoms. Each of them is treated differently. First of all, it is necessary to determine what diseases cause supraventricular arrhythmia, what symptoms accompany it, what is the patient's prognosis and how to treat it. Symptoms that are typical of supraventricular arrhythmia include:
- cardiopalmus,
- fatigue,
- dyspnea,
- fainting,
- dizziness,
- chest discomfort.
There are often no symptoms with supraventricular accessory beats.
CASE DESCRIPTION
A 51-year-old man, an office worker, was sent for consultation to the somnology office of the University Clinical Hospital No. 1 in September 2021 due to predominantly nocturnal heart rhythm disturbances detected in him.
At the time of treatment, he complained of shortness of breath during physical activity of moderate intensity (fast walking), and also, upon targeted questioning, noted the presence of loud snoring during sleep and daytime sleepiness, which manifested itself as uncontrollable falling asleep while watching TV shows or when riding in transport as a passenger .
From the anamnesis it is known that the patient has been suffering from stage 2 hypertension for a long time, stage 3 high blood pressure (BP), with a very high risk of cardiovascular complications, controlled by taking antihypertensive drugs and type 2 diabetes mellitus. An increase in blood pressure has been observed for more than 10 years with its maximum rises to 190/110 mm Hg. Art. In recent years, he has been carefully monitoring blood pressure numbers; while taking perindopril 10 mg, indapamide 2.5 mg in the morning and amlodipine 5 mg in the evening, blood pressure has stabilized within 135-145/85-90 mm Hg. Art., with rare rises to a maximum of 155/100 mm Hg. Art., usually in the morning immediately after waking up, which did not require additional therapy “on demand”. Type 2 diabetes mellitus was diagnosed 7 years ago. He receives therapy with long-acting metformin 1000 mg in the evening and alogliptin 25 mg in the morning, in accordance with the recommendations of his attending endocrinologist, he controls the level of fasting glycemia and glycated hemoglobin.
He has been snoring for about twenty years; in the last 3 years, against the background of a significant (more than 20 kg) weight gain, the snoring intensified, the patient began to notice shortness of breath when walking, daytime drowsiness and fatigue appeared, regardless of the duration of the previous night's sleep.
Denies smoking or alcohol abuse, there are no occupational hazards.
Upon examination, the condition is satisfactory. There is significant excess weight: with a height of 176 cm, the patient weighs 125 kg, body mass index 40.3 kg/m2, which corresponds to grade 3 obesity. On auscultation, no wheezing is heard over the lungs. Respiratory rate 18/min. Blood oxygen saturation, measured with a pulse oximeter, is 98% at rest; after brisk walking along the corridor, it decreases to 96% (when the norm is more than 95%), but quickly recovers to the original level at rest. Heart sounds are generally rhythmic; auscultation reveals rare extrasystole. Heart rate 80/min., blood pressure 140/85 mmHg. Art. The liver is not palpable. The symptom of effleurage is negative. The shins are pasty.
Shortly before contacting a somnologist, the patient underwent a routine outpatient examination.
According to the submitted medical documentation, the general blood test was unremarkable. In the biochemical blood test, no significant metabolic or electrolyte abnormalities were detected, with the exception of a tendency to increase total cholesterol levels: glucose 5.8 mmol/l (target level <6.0 mmol/l), potassium 4.1 mmol/l (normal 3.5–5.0 mmol/l) , creatinine 86 µmol/l (normal 74–110 µmol/l), total cholesterol 6.3 mmol/l (target level <4.5 mmol/l), an extended study of the blood lipid spectrum was not performed. HbA1C level 6.4% (target level <7.0%).
A resting electrocardiogram (ECG) showed sinus rhythm with a heart rate of 82 per minute, EOS deviation to the left, and no conduction abnormalities were detected; There are voltage signs of left ventricular hypertrophy and a single ventricular extrasystole.
According to the results of an echocardiographic study, the heart cavities are not dilated; there are signs of moderate left ventricular hypertrophy. The contractile function of the left ventricular myocardium is within normal limits, the ejection fraction is 61%. No zones of hypokinesia were identified, the valve apparatus was intact. There are signs of moderate pulmonary hypertension.
During 24-hour ECG monitoring, sinus rhythm was recorded with a heart rate of 41-126 per minute, an average heart rate of 79 per minute. Frequent single monomorphic ventricular extrasystoles (VCs), including those of the bigeminy type, were detected, mainly during sleep: a total of 1350 extrasystoles during the day and 3474 at night. Also, during sleep, two short (of 8 and 12 cycles) paroxysms of a regular rhythm with wide complexes with a heart rate of 65 per minute (most likely an accelerated idioventricular rhythm) were recorded. ST segment without significant dynamics.
The patient underwent overnight cardiorespiratory monitoring with synchronous recording of nasal airflow, snoring, respiratory efforts of the chest and abdomen, blood oxygen saturation and one ECG channel. According to the study results, the apnea-hypopnea index was 57 respiratory events per hour (norm <5 per hour) with a maximum duration of obstructive apnea of up to 74 seconds. The minimum oxygen saturation during sleep is 73% with an average overnight saturation of 91%. The ECG recorded frequent single monomorphic PVCs, including those of the bigemeny type, and one short (7 cycles) paroxysm of a regular rhythm with wide complexes with a heart rate of 60 per minute (most likely an accelerated idioventricular rhythm).
Based on the results of the cardiorespiratory study, most of the extrasystoles and paroxysms of accelerated idioventricular rhythm were associated with prolonged apneas leading to severe desaturation (Figures 1, 2 and 3). It was concluded that the patient had severe OSAS, severe nocturnal hypoxemia, and heart rhythm disturbances associated with obstructive apnea.
Rice. 1.
Cardiorespiratory monitoring (recording fragment 60 sec.). Frequent PVCs in the terminal part of obstructive apnea lasting 57 seconds.
Rice. 2.
Cardiorespiratory monitoring (recording fragment 60 sec.). Against the background of breathing restoration after obstructive apnea, which lasted 63 seconds, frequent PVCs (bigeminia) are recorded.
Rice. 3.
Cardiorespiratory monitoring (recording fragment 90 sec.). Short (7 cycles) paroxysm of a regular rhythm with wide complexes (accelerated idioventricular rhythm) in the final part of obstructive apnea, which lasted 60 sec.
This severity of breathing disorders during sleep is an absolute indication for CPAP therapy. Treatment was started using an Auto-CPAP device with an integrated pulse oximetry module, in the mode of automatic pressure titration in the range of 4–16 cmH2O. pillar The effectiveness of therapy was monitored using the standard software of the device. When assessed 7 days after the start of treatment, complete compensation of respiratory disorders during sleep was stated: the residual apnea-hypopnea index was 4 per hour, the average oxygen saturation at this time did not fall below 90% and averaged 94%. The patient himself noted the disappearance of daytime sleepiness.
During control Holter monitoring against the background of ongoing CPAP therapy, the number of single ventricular extrasystoles during sleep decreased almost by half, becoming equal to those observed during wakefulness—a total of 1275 during the day and 1476 at night. No episodes of accelerated idioventricular rhythm were detected.
The patient is recommended to continue CPAP therapy during night sleep on a regular basis, as well as further examination to rule out coronary artery disease and decide whether to prescribe adequate lipid-lowering therapy.
Treatment of supraventricular arrhythmias
First of all, it is important to have a detailed history of not only heart disease, but also general, rheumatological, metabolic and endocrine diseases. This usually starts with non-invasive tests such as: morphology, ECG, cardiac ECHO and Holter study. If necessary, invasive and complex tests such as electrophysiological studies are performed. Supraventricular arrhythmias are usually treated with medications. When this doesn't work, you can introduce ablation, for example. These two treatments can also effectively complement each other.
The article is for informational purposes only, self-medication is not acceptable. Be sure to consult with your healthcare provider.
Diagnostics
The diagnosis is made on the basis of an ECG. The wavy peaks of the QRS complexes are clearly visible on the film. The complexes themselves change their orientation around the isoline. An increased QT interval is present on the electrocardiogram outside of an attack. Normally, its value is within 0.44 s. You should pay attention to family history: if one of your relatives has an increased interval, then the risk of developing torsade de pointes increases.
- Example of tachycardia associated with digoxin toxicity
Such tachycardia often does not last long and goes away on its own, but sometimes leads to hemodynamic destabilization with subsequent collapse. It can also develop into ventricular fibrillation. In this case, immediate assistance will be required: indirect cardiac massage and stimulation of myocardial activity with an electric current discharge.
- Torsade de pointes resulting from hypokalemia
The ECG of a patient with hypokalemia is shown in the photo below: the patient experienced a brief self-terminating paroxysm of torsade de pointes with an “R on T” layering effect.
- Torsades de Pointes