Angioplasty and stenting of the heart arteries is a method of treating coronary heart disease (CHD), which is performed without incisions under X-ray control and consists of restoring the patency of blocked coronary vessels. The essence of coronary angioplasty is to install a special catheter with a small balloon in the narrowing area. After inflation of the balloon, the lumen of the coronary artery is restored. To maintain the lumen of the coronary artery, it is necessary to install a metal frame - a stent.
Coronary angioplasty is a treatment that saves thousands of lives in patients with acute myocardial infarction. The advent of this technology has made it possible to reduce the mortality rate of a heart attack by 10 times and improve the quality of life in most patients with coronary artery pathology.
Long-term results of coronary angioplasty and stenting depend on follow-up and the stents used. Modern stents significantly improve the prognosis of the further course of the disease.
The endovascular clinic of the Innovative Vascular Center has achieved excellent results in emergency and planned operations for coronary heart disease. To correct stenoses and occlusions of the coronary arteries, we use the most modern endovascular instruments (balloons and stents). Every month, the clinic performs about 100 interventions on the coronary arteries in patients with acute coronary syndrome and elective angina.
- Our surgeons managed to achieve a minimum number of adverse outcomes in patients with myocardial infarction, and this figure remains the lowest in the Moscow region over the past years.
- Coronary angioplasty is performed using the latest Philips Allura Xper FD20 angiographic unit.
- Our endovascular surgeons use the safest radial approach on the arm.
- Our cardiac stenting technology often eliminates the need for coronary artery bypass grafting.
- We use the best stents to achieve optimal results.
- We have the most understandable and affordable prices for cardiac stenting.
Preparation for coronary angiography
To plan the operation, it is necessary to obtain information about the condition of the coronary arteries and heart function. For this purpose, diagnostic tests are carried out, which in an emergency include an ECG and laboratory diagnostics, and in a planned case, a more detailed examination is necessary.
Examination before elective surgery includes:
- ECG (including Holter monitoring)
- Echocardiography (including with load)
- MSCT coronary angiography or preliminary coronary angiography
- Gastroscopy (EGD)
- X-ray of the lungs
Before surgery, you may be given a loading dose of antithrombotic drugs to avoid early thrombotic complications.
How is coronary angioplasty and stenting performed?
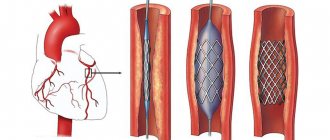
Coronary angioplasty is performed without incisions through a small puncture in the artery. The main approaches to the artery for coronary stenting are femoral (in the groin area) and radial (at the wrist). This area is treated with an antiseptic. After the artery is punctured, a thin tube is installed into it - an introducer. The main work on angioplasty and stenting is carried out through it.
A thin guide is placed inside the artery, which goes to the coronary vessels and should overcome the blockage. Together with it, a catheter is passed to the heart, through which a contrast agent is injected for orientation inside the vessel. A series of coronary angiograms are performed and the location of the arterial blockage is determined. To perform angioplasty, the guidewire must be passed past the site of the coronary artery blockage. After this, we proceed to the angioplasty procedure itself.
To do this, a special balloon is passed through the conductor in a folded state and installed at the site of the narrowing. Using a special device, this balloon is inflated and opens the lumen of the artery. The procedure lasts a few seconds to avoid causing severe chest pain due to blockage of blood flow in the coronary artery.
Stenting is the installation of a special metal mesh to maintain the artery wall in an inflated state. Stenting can improve the immediate and long-term results of endovascular surgery. Currently, stenting is performed in most cases of endovascular interventions on the coronary arteries.
The stent is permanently in the artery and can overgrow over time, so it is advisable to use drug-coated stents, which overgrow much more slowly and last much longer.
Our clinic successfully uses the absorbable Absorb stent, which is made of a material that undergoes self-disintegration over time. When using such a stent, after 2 years there is no longer a foreign body left in the coronary artery. The use of Absorb can significantly improve long-term results of coronary stenting.
After stenting, the surgeon conducts a control angiographic study and, making sure that the result is good, removes the entire instrument. A pressure bandage is applied to the access site or a special device is used to close the puncture.
Cost of the operation
The price of the operation depends on which clinic and in which country the patient chooses. Also, the pricing policy will be influenced by the degree of complexity of the upcoming intervention and the number of affected vessels. The main cost component of surgical vasodilation is the price of the dilation device, which will remain inside the patient's body.
In Russia, prices range from 85,000 to 200,000 rubles. This is how much the operation itself, the necessary medications, and hospital stay will cost. The stent itself will cost from 45,000 to 150,000 rubles. Treatment, for example, in Israel is somewhat more expensive. Additionally, the patient will have to pay for flights, food and accommodation.
Possible risks of coronary angioplasty
Although angioplasty is less invasive than bypass surgery, the procedure still carries some risks. Risks may be associated with the procedure itself and its long-term outcomes.
Early risks:
- Bleeding. There may be bleeding in the leg or arm where the vessel was accessed. Usually it just develops as a bruise, but sometimes there is serious bleeding that may require a blood transfusion or surgery.
- Heart attack. Coronary circulation disorders develop very rarely during surgery, but sometimes, due to technical reasons, a rupture or dissection of the coronary artery may develop. These complications may require emergency coronary artery bypass surgery.
- Kidney problems. The contrast agent used in angioplasty and stent placement can cause kidney damage, especially in people who already have kidney problems. If you are at higher risk, your doctor may take steps to protect your kidneys, such as limiting the amount of contrast material and increasing fluid intake to dilute the contrast.
- Ischemic stroke. During angioplasty, a stroke can occur if pieces of plaque break off as the catheter is passed through the aorta. Stroke is an extremely rare complication of coronary angioplasty. To prevent it, drugs that reduce blood clotting are prescribed.
- Heart arythmy. During the procedure, the heart may beat too fast or too slow. Such arrhythmias are usually short-lived, but sometimes a temporary pacemaker is required.
Late complications
- Repeated narrowing of the artery (restenosis). With angioplasty without stenting, the rate of restenosis is approximately 30% of cases. Stents have been developed to reduce restenosis. The use of plain metal stents reduces the risk of restenosis to 15%, and the use of drug-eluting stents reduces the risk to less than 10%.
- Stent thrombosis. Blood clots (thrombi) can block an artery, causing a heart attack. To reduce the risk of thrombosis, it is important to take aspirin, clopidogrel (Plavix), which helps reduce the risk of blood clots forming in the stent. Never stop taking these medications without talking to your doctor.
Literature
- DORMANDY JA, MAHIR MS. The natural history of peripheral atheromatous disease of legs. In: Greenhalgh RM, Jamieson CW, Nicolaides AN, (ed.), Vascular surgery. Issues in current practice. London, Grune & Stratton, 1986 pp 3-17.
- MARTY-ANE C, ALAUZEN M, MARY H. L'expectative medicale dans les lesions obstructives isolees de l'art e re femorale superficielle. In: B ranche reau A, Jausseran JM, (eds), Traitement des lesions obstructives de l'artere femorale superficielle. Marseille, CVN, 1992 pp. 13-17.
- JOFFRE F, ROUSSEAU H, MEITES G, CHEMALI R. Resultats a long terme des angioplasties femoro-poplitees. In: Branchereau A, Jausseran JM, (eds), Traitement des lesions obtructives de l'artere femorale superficielle.Marseille, CVN, 1992 pp 39-51.
- JOHNSTON KW. Femoral and popliteal arteries: reanalysis of results of balloon angioplasty. Radiology 1992; 183: 767-771.
- HUNINK MGM, DONALDSON MC, MEYEROVITZ MF et al. Risks and benefits of femoropopliteal percutaneous balloon angioplasty. J Vasc Surg 1993; 17: 183-194.
- BECQUEMIN JP, CAVILLON A, HAIDUC F. Surgical transluminal femoropopliteal angioplasty: multivariate analysis outcome. J Vasc Surg 1994; 19: 495-502.
- MATSI PJ, MANNINEN HI. Impact of different patency criteria on long-term results of femoropopliteal angioplasty: analysis of 106 consecutive patients with claudication. J Vasc Interv Radiol 1995; 6: 159-163.
- STANLEY B, TEAGUE B, RAPTIS S et al. Efficacy of balloon angioplasty of the superficial femoral artery and popliteal artery in the relief of leg ischemia. J Vasc Surg 1996; 23: 679-685.
- COURBIER R. Le traitement des lesions de l'artere femorale superficielle. In: Branchereau A, Jausseran JM, (eds), Traitement des lesions obtructives de l'artere femorale superficielle. Marseille, CVN, 1992 pp XIII-XIV.
- DIETHRICH EB, PAPAZOGLOU K. Endoluminal grafting for aneurysmal and occlusive disease in the superficial femoral artery: early experience. J Endovasc Surg 1995; 2: 225-239.
- BERGERON P, PINOT JJ, POYEN V et al. Long-term results with the Palmaz stent in the superficial femoral artery. J Endovasc Surg 1995; 2: 161-167.
- AHN SS, RUTHERFORD RB, BECKER GJ et al. Reporting standards for lower extremity arterial endovascular procedures. J Vasc Surg 1993; 17: 1103 -1107.
- BRAY AE, LIU WG, LEWIS WA et al. Strecker stents in the femoral arteries: value of Duplex ultrasonography in restenosis assessment. J Endovasc Surg 1995; 2: 150-160.
- BECKER GJ, KATZEN BT, DAKE MD. Noncoronary angioplasty. Radiology 1989; 170: 921-940.
- MATSI PJ, MANNINEN HI, VANNINEN RL et al. Femoropopliteal angioplasty in patients with claudication: primary and secondary patency in 140 limbs with 1-3 year follow-up. Radiology 1994; 191: 727733.
- Guidelines for percutaneous transluminal angioplasty. Standards of Practice Committee of the Society for Cardiovascular and Interventional Radiology. Radiology 1990; 177: 619-626.
- MURRAY RR Jr, HEWES RC, WHITE RI Jr et al. Long-segment femoropopliteal stenoses: is angioplasty a boom or a bust ? Radiology 1987; 162: 473-476.
- CURRIE IC, WAKELEY CJ, COLE SE et al. Femoropopliteal angioplasty for severe limb ischemia. Br J Surg 1994; 81: 191-193.
- SIVANANTHAN UM, BROWNE TF, THORLEY PJ, REES MR Percutaneous transluminal angioplasty of the tibial arteries. Br J Surg 1994; 81: 1282-1285.
- BLAIR JM, GEWERTS BL, MOOSA Hetal. Percutaneous transluminal angioplasty versus surgery for limb-threatening ischemia. J Vasc Surg 1989; 9: 698-703.
- SEEGER JM. Laser angioplasty. A vascular surgeon's view. Circulation 1991; 83 (I): 97-98.
- SATIANI B, DAS BM, VACCARO PS, GAWRON D. Angiographic follow-up after laser-assisted balloon angioplasty. J Vasc Surg 1993; 17: 960-966.
- FISHER CM, FLETCHER JP, MAY Jetal. No additional benefit from laser in balloon angioplasty of the superficial femoral arter y. Eur J Vasc Endovasc Surg 1996; 11: 349-352.
- DALSING MC, HARRIS VF. Intravascular Stent. In: White RA, Fogarty TJ, (eds), Peripheral endovascular interventions. St Louis, Mosby, 1996 pp 315-339.
- HENRY M, AMOR M, HENRY I et al. Placement of Palmaz stent in femoropopliteal art eries: a six year experience. Factors influencing restenosis and longterm results. In: Abstract Book 6° International course on peripheral vascular intervention. Oct 1995, Nancy, France.
- WHITE GH, LIEW SCC, WAUGH RC et al. Early outcome and intermediate follow-up of vascular stents in the femoral and popliteal arteries without long-term anticoagulation. J Vasc Surg 1995; 21: 270-281.
- DO-DAI-DO, TRILLER J, WALPOTH BH et al. A comparison study of self-expandable stents vs balloon angioplasty alone in femoropopliteal artery occlusions. Cardiovasc Intervent Radiol 1992; 15: 306-312.
- HENRY M, AMOR M, HENRY I et al. Endoluminal bypass grafting in leg arteries with the Cragg Endopro System 1. A series of 105 patients. In Abstract book 6° International course on peripheral vascular intervention. Oct 1995, Nancy, France.
- G. Agrifiglio et al.1999
Prognosis after treatment
Coronary angioplasty significantly increases blood flow through a previously narrowed or blocked coronary artery. In this case, chest pain (angina) should usually decrease, and the physical capabilities of the body, on the contrary, should increase.
You need to understand that angioplasty and stenting do not cure coronary heart disease, but only eliminate specific circulatory disorders of the heart muscle. To achieve a stable result, you must lead a healthy lifestyle and take medications prescribed by your doctor.
If the symptoms of angina return, then you need to contact your doctor again, and if you have chest pain at rest that does not respond to nitroglycerin, then call an ambulance.
After coronary angioplasty and stenting, the quality of life improves in 95% of patients, with many of them maintaining the effect for more than 5 years.