Sokolov Lion index how to calculate
According to the recommendations in force in 2014, LVMH according to ECG data is determined by only two criteria, despite the fact that previously doctors used more than ten signs.
We will take the golden mean, consider 3 criteria, but still start with the main ones, the identification of which almost 100% indicates LVMH and is confirmed by ultrasound data. All other criteria have unsatisfactory specificity.
Sokolov-Lyon Index (SLI)
Sokolov-Lyon index (SLI) = SV1 (mm) + RV5 (mm) or RV6 (mm).
Normal: up to 48 mm in persons under 40 years of age and up to 38 mm in persons over 40 years of age
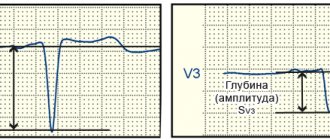
To determine this index, it is necessary to add the amplitude (depth) of the SV1 tooth to the amplitude (height) of RV5 or RV6. The resulting figure, expressed in millimeters, will be the index.
Cornell voltage product (CVP)
Cornell voltage product (CVP) = [RaVL(mm) + SV3 (mm)] × QRS (ms)
Normal: less than 2440 mm/ms.
The Cornell voltage product is calculated a little more complicated: it is necessary to multiply the duration of the QRS complex, expressed in milliseconds, by the sum of R -aVL (mm) + S -V3 (mm). The difficulty is that you have to multiply large numbers and you can’t do it without a calculator. If the obtained value exceeds 2440, then we are talking about LVMH.
Other criteria
RV4 RV6 or RV4
Now we will discuss the criterion of LVMH determined by the dynamics of the R wave in the precordial leads. The fact is that in non-hypertrophied myocardium the total excitation vector is directed to the apex, therefore the highest R wave will be recorded in lead V4.
In the case of hypertrophy, (but not always) the vector will shift to the left, partly due to thickening of the lateral wall of the left ventricle, and partly due to changes in the boundaries of the heart.
Because of this, the maximum R begins to be determined not in V4, as is normal, but in lead V5 or V6.
Many “old school” cardiologists consider this sign to be the most important, however, this is not so.
The reason lies in the fact that cardiologists are accustomed to seeing mostly sick people who have hypertrophy in 80%-90%, but if they examine the entire population, then an erroneous conclusion about LVMH will be given to every second patient with such changes on the ECG.
So, be careful with this criterion, although it has greater sensitivity than the above indices (ISL and KVP), but its specificity is no more than 60%, while for the above indices it approaches 100%.
Left ventricular systolic overload
A separate concept in the LVMH section is “systolic overload of the left ventricle.”
It must be said that in fact, the ventricle does not experience any special overload either at the time of ECG recording or during any other period of time, except for that which is associated with high blood pressure. There are situations when a person with blood pressure is 150/90 mm Hg.
we see “systolic overload”, but in others, even with a pressure of 220/120 mm Hg, there is no hint of such changes. In addition, normalization of blood pressure never led to the disappearance of “overload”.
Systolic overload as an ECG phenomenon occurs in the case of severe hypertrophy, which leads to disruption of the repolarization wave, but we will not go into details, the main thing is that you understand the meaning of this term and do not confuse hemodynamics with electrical activity.
Yes, so how does this “phenomenon” manifest itself? And it manifests itself in the form of disturbances in the repolarization processes of a very specific type (see further on the ECG), occurring in the area of the lateral wall of the left ventricle, always in combination with high R waves or, more often, in combination with positive criteria for LVMH (ISL or CVP).
In conclusion, it is worth noting that in my (and not only my) opinion, in the presence of positive criteria for ISL and CVP, we need to talk about quantitative signs of hypertrophy, while a shift of the transition zone to the left should be called qualitative signs of hypertrophy.
Limitations of criteria, IMPORTANT! IMPORTANT! IMPORTANT!
1. In the presence of complete or incomplete blockade of the left leg, the criteria do NOT work!
2. In the presence of complete blockade of the right leg, the criteria do NOT work!
3. If there are scar changes, the criteria do NOT work!
4. If the criteria are negative, this does NOT mean that there is no hypertrophy! Low sensitivity.
Determining LVMH despite points 1-3 is a gross mistake, which is nevertheless very common even among cardiologists!
Well, let's see how it all looks.
Example 1
This ECG can show almost all the criteria for left ventricular myocardial hypertrophy (LVMH).
1. Sokolov-Lyon index (ISL) = SV1 (19 mm) + RV5 (22 mm) = 41 mm (norm up to 38 mm)
2. Cornell voltage product (CVP) = [RaVL(13 mm) + SV3 (10 mm)] × QRS (100 ms) = 2300 ms*mm (the norm is up to 2440, this negative criterion was slightly missed)
3. Displacement of the transition zone - RV4 4. Systolic overload - we see ST depression in V5 and V6 and biphasic, predominantly negative, T, that is, a violation of repolarization processes.
Example 2
For this ECG, there are no generally accepted criteria for left ventricular myocardial hypertrophy (LVMH).
1. Sokolov-Lyon index (ISL) = SV1 (7 mm) + RV5 (12 mm) = 19 mm (norm up to 38 mm)
2. Cornell voltage product (CVP) = [RaVL(0 mm) + SV3 (4 mm)] × QRS (80 ms) = 320 ms*mm (normal up to 2440)
3. Displacement of the transition zone - present, RV4 RV6, that is, suspicions of LVMH are appropriate, but writing that it exists would be incorrect.
4. Systolic overload - we cannot talk about overload here, since there are no signs of hypertrophy. There is a slight depression of ST V5 and V6, which is within the normal range.
Source: https://glivec.su/2018/04/18/indeks-sokolova-lajona-kak-rasschitat/
Cornell voltage product (CVP)
Cornell voltage product (CVP) = [RaVL(mm) + SV3 (mm)] × QRS (ms)
Normal: less than 2440 mm/ms.
The Cornell voltage product is calculated a little more complicated: it is necessary to multiply the duration of the QRS complex, expressed in milliseconds, by the sum of R -aVL (mm) + S -V3 (mm). The difficulty is that you have to multiply large numbers and you can’t do it without a calculator. If the obtained value exceeds 2440, then we are talking about LVMH.
Left ventricular hypertrophy on ECG
Left ventricular hypertrophy.
In a healthy person, the mass of the left ventricle is three times that of the right. With left ventricular hypertrophy, these ratios increase to 4:1, 5:1 or more. This leads to the fact that the excitation vector of the left ventricle increases significantly, but the direction of these vectors does not change.
Due to hypertrophy of the left part of the interventricular septum of the heart, the excitation vector of the septum increases, which, as normal, is directed from left to right (1). This vector gives rise to the formation of the r wave in V1 and the q wave in V5-V6.
Next, the total excitation vector of the right and left ventricles is formed, which, due to the increase in the left ventricular component, is enlarged and directed from right to left towards V5-V6 (2).
This total vector will give rise to the formation of a deep S wave in V1 and a tall, somewhat widened R wave in V5-V6.
Thus, with left ventricular hypertrophy in V1, as normally, will have the rS formula, and V5-V6 the qR formula, but the S wave in V1 and the R wave in V5-V6, but the S wave in V1 and the R wave in V5 -V6 will be larger in amplitude than normal.
Left ventricular hypertrophy will also affect the appearance of other leads.
Those that reflect the right heart (III, aVF, V1-V2) will have deep S waves, and those that reflect the left heart (I, aVL, V4-V6) will have tall R waves.
With left ventricular hypertrophy, repolarization processes occur somewhat differently. The repolarization vector of the right ventricle does not change. The repolarization vector of the left ventricle changes its direction due to a significant increase in its mass. This occurs because the travel time of the excitation dipole from the endocardium to the epicardium increases.
This time begins to exceed the physiological delay time of the negative charge. In the subendocardial layer of the left ventricular muscle, a resting potential arises and the repolarization vector diametrically changes its direction, it turns from the epicardium to the endocardium (3). All these processes lead to a discordant (mirror) change in the final part of the ventricular complex.
The ST segment and T wave shift in the opposite direction from the main wave of the QRS complex. In V1 and other leads reflecting the right heart, the ST segment tends to rise, and in V5-V6 and other leads reflecting the left heart, it tends to fall.
Unlike coronary heart disease, in which the arc of such ST deviations is directed in the direction of the deviation, in left ventricular hypertrophy the arc is directed in the opposite direction.
For electrocardiographic diagnosis of left ventricular hypertrophy, a number of calculated values are used, the main ones of which are given below.
According to WHO experts (1999), the most informative electrocardiographic indicators of left ventricular hypertrophy are:
Classification
Depending on whether the entire left ventricle is enlarged in volume or only some part of it, several types are distinguished:
Concentric, or symmetrical, hypertrophy is characterized by a uniform increase in the thickness of the walls of the ventricle. Eccentric hypertrophy usually affects the interventricular septum, but sometimes the apical or lateral wall region may be involved.
Depending on the effect on systemic blood flow, hypertrophy can be:
Without outflow tract obstruction. In this case, the effect on systemic blood flow is minimal. Most often, concentric hypertrophy of the left ventricular myocardium, in contrast to the asymmetric form, is not accompanied by obstruction.
With obstruction of the outflow tract, when during contraction of the ventricle, that is, in systole, compression of the aortic mouth occurs. This creates an additional obstacle to the flow of blood and closes the so-called vicious circle.
It further enhances hypertrophy
According to the degree of increase in the mass and thickness of the left ventricle, three stages are distinguished:
Severe hypertrophy is accompanied by an increase in thickness at the time of heart contraction of more than 25 mm. The average degree is observed with a myocardial thickness of 21-25 mm. Moderate left ventricular hypertrophy is diagnosed when the wall thickness is less than 21 mm, but more than 11 mm.
For quite a long time, symptoms of hypertrophy may be absent and it can only be detected through instrumental examination.
When increased myocardial mass begins to affect systemic blood flow, signs of disease gradually appear. At first they occur occasionally, only under significant loads. Over time, symptoms begin to bother the patient even at rest.
The most characteristic signs of left ventricular myocardial hypertrophy include:
- shortness of breath and feeling of lack of oxygen; heart rhythm disturbances (tachycardia, flicker, fibrillation, extrasystole), interruptions, pauses; characteristic anginal pain associated with a decrease in oxygen supply to the muscle cells of the heart; dizziness and fainting that occur when blood flow through the cerebral arteries is disrupted; heart failure, characterized by stagnation of blood in the respiratory circle (pulmonary edema, cardiac asthma).
Rarely, the first symptom of hypertrophy is cardiac death associated with circulatory arrest.
Diagnostic ECG criteria for LV hypertrophy
There are a lot of diagnostic criteria for LV hypertrophy, but the Sokolov-Lyon index and the Cornish voltage index are most often used.
For a reliable diagnosis of LV hypertrophy, voltage criteria must be supplemented by non-voltage signs.
Voltage criteria in standard leads:
- R wave in lead I + S in lead III > 25 mm
- R wave in lead aVL > 11 mm
- R wave in lead aVF > 20 mm
- S wave in lead aVR > 14 mm
Voltage criteria in chest leads:
- R wave in leads V5 or V6 + S wave in lead V1 > 35 mm (Sokolov-Lyon index)
- R in aVL + S in V3 > 28 mm in men and > 20 mm in women (Cornell Voltage Index)
- R wave in leads V4, V5 or V6 > 26 mm
- Highest R + deepest S in precordial leads > 45 mm
Non-voltage signs of LVH:
- Increasing the rise time of the R wave > 50 ms in leads V5 or V6
- ST depression and T wave inversion in the “left” leads (so-called signs of LV overload)
What else may indicate LVH:
- Signs of LA hypertrophy.
- EOS deviation to the left.
- The appearance of ST elevation in the “right” precordial leads (V1-3), discordant with deep S waves.
- Appearance of noticeable U waves proportional to increased QRS amplitude
Example 1: LV hypertrophy in a patient with hypertension
This ECG can detect several criteria for LV hypertrophy:
- Sinus rhythm, 78 beats. per minute, normal EOS (more about EOS)
- Sokolov-Lyon index = 37mm (depth S in V1 + height R in V5-V6 >35 mm)
- S wave in lead aVR > 14 mm
- Downward ST depression and T wave inversion in the “left” leads I, V5, V6 (so-called “signs of LV overload”)
Example 2: LV hypertrophy in a patient with atrial fibrillation
- Atrial fibrillation with a ventricular rate of 91 per minute. (60 - 125 beats/min.).
- Horizontal EOS (maximum positive QRS sum - in lead I).
- Left ventricular hypertrophy (Sokolov-Lyon index is 37: R(V5)=24mm + S(V2)=13mm)
Treatment
Treatment of ventricular hypertrophy of the heart primarily involves eliminating the causes of this pathology. For example, if hypertrophy of the left cardiac ventricle has developed against the background of arterial hypertension, the patient is prescribed antihypertensive drugs to normalize blood pressure, as well as diuretics to remove excess fluid and prevent edema.
If gastric hypertrophy of the heart occurs due to diseases of the respiratory system, bronchodilators and anti-inflammatory drugs are used, depending on the original disease.
In cases where there are severe (congenital or acquired) heart valve defects, treatment will most likely be surgical, including replacing the diseased valve with a prosthesis. In particularly difficult situations, the only possible solution is organ transplantation.
For whatever reason, ventricular hypertrophy of the heart develops, any treatment involves combating myocardial damage - prescribing cardiac glycosides and drugs to stimulate metabolic processes in the heart muscle. If necessary, antiarrhythmic treatment is prescribed.
Sometimes, in addition to basic methods, the patient is prescribed a special diet that limits salt and fluid intake. If excessive body weight (obesity) occurs, it should be normalized.
In any case, the approach to heart treatment should be purely individual and should take into account all existing manifestations of heart failure, as well as the presence or absence of concomitant diseases in the patient and his general health.
It is quite possible to cure hypertrophy that is diagnosed in a timely manner, therefore, at the slightest suspicion of cardiac dysfunction, you should immediately consult a specialist. The doctor will conduct all the necessary studies and prescribe appropriate treatment, which will give the patient every chance of a long life.
Limitations of criteria, IMPORTANT! IMPORTANT! IMPORTANT!
1. In the presence of complete or incomplete blockade of the left leg, the criteria do NOT work!
2. In the presence of complete blockade of the right leg, the criteria do NOT work!
3. If there are scar changes, the criteria do NOT work!
4. If the criteria are negative, this does NOT mean that there is no hypertrophy! Low sensitivity.
Determining LVMH despite points 1-3 is a gross mistake, which is nevertheless very common even among cardiologists!
Well, let's see how it all looks.
Content:
The Sokolow Index is a criterion used to diagnose left ventricular chamber enlargement of the heart based on the measurement of the waves that represent the left ventricle on the electrocardiogram.
The electrocardiogram is printed on a millimeter sheet. From the sum of the small squares that the wave's amplitude occupies, its voltage is obtained. The Sokolov index is the result of the sum of the amplitude of the S wave in precordial vectors V1 plus the R wave in V5 or V6. Thus: S V1 + RV 5 or 6 = Sokolov index.
A result greater than 35 mm indicates that the patient has left ventricular hypertrophy, meaning that their left ventricular heart chamber is thicker than normal.
This type of abnormality is a consequence of diseases such as hypertension, which causes the heart muscle to become overworked due to the high pressure it must overcome to pump blood.
Sokolov and Lyon
North American cardiologists Maurice Sokolov and Thomas Lyon based their professional careers on the study of hypertension and its complications.
One of the most common conditions associated with this disease is left ventricular hypertrophy, which is nothing more than a thickening of the muscular wall of the left ventricle of the heart.
These specialists described a way to calculate the state of the heart muscle by measuring the voltage of certain waves on the electrocardiogram. The technique was published in 1949 in a scientific journal. American Heart Journal and it was called "Ventricular complex in left ventricular hypertrophy obtained with unipolar precordial and limb electrodes."
The method is called the Sokolow-Lyon Index, and is one of the criteria currently used to determine left ventricular hypertrophy in patients with heart disease, especially hypertension.
Importance and clinical significance
The gold standard for detecting ventricular hypertrophy is an echocardiogram. However, this research is expensive and requires trained personnel to conduct and analyze it.
The importance of the Sokolow index is that it is based on the measurement of the electrocardiogram, which is the basic test of clinical examination, and is also inexpensive, easy to perform, and can be analyzed by any physician.
Based on the electrocardiogram, the doctor diagnoses ventricular hypertrophy, and the patient is referred to a cardiologist for in-depth study.