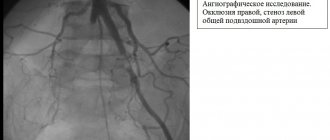
Classification of forms of the disease
(Reference: narrowing of the arteries - stenosis, complete blockage - occlusion)
- stenosis and occlusion of the internal carotid artery,
- stenosis and occlusion of the common carotid artery,
- stenosis and occlusion of the vertebral artery,
- stenosis and occlusion of the subclavian artery.
Narrowing of these arteries that supply blood to the brain leads to chronic cerebrovascular insufficiency (CCI) or stroke (cerebral infarction).
KhNMK
- a state of constant lack of blood in the brain, continuous oxygen starvation of brain tissue, forcing brain cells to be in constant tension of all intracellular systems and intercellular connections, which leads to disruption of the normal functioning of both brain cells and the organ as a whole.
The main classification of chronic cerebrovascular insufficiency (CHF), used in Russia (according to A.V. Pokrovsky), contains 4 degrees:
- I degree
- asymptomatic course or absence of signs of cerebral ischemia against the background of proven, clinically significant cerebral vascular damage; - II degree
- transient ischemic attack (TIA) - the occurrence of focal neurological deficit with complete regression of neurological symptoms within up to 1 hour; transient cerebrovascular accidents (TCI) - the occurrence of focal neurological deficit with complete regression of neurological symptoms within up to 24 hours; - III degree
- the so-called chronic course of SMN, i.e. the presence of cerebral neurological symptoms or chronic vertebrobasilar insufficiency without a history of focal deficiency or its consequences. In neurological systematizations, this degree corresponds to the term “dyscirculatory encephalopathy”; - IV degree
- previous, completed or complete stroke, i.e. the existence of focal neurological symptoms for more than 24 hours, regardless of the degree of regression of the neurological deficit (from complete to no regression).
Dry statistics cannot fully reflect the tragedy of the situation when a cerebral infarction occurs - a stroke... But stroke ranks second in the structure of overall mortality of the population, second only to cardiac pathology. 35% of patients who have had a stroke die within the first month, and approximately 50% of patients die within a year, i.e. every second. Think about these numbers: stroke affects about 6 million people in the world every year, and in Russia - more than 450,000, i.e. Every 1.5 minutes, one of the Russians suffers a stroke for the first time. In St. Petersburg, 12 thousand cases of stroke are registered annually.
Atherosclerosis of cerebral and peripheral arteries: issues of therapy
Atherosclerosis is a chronic disease of elastic and muscular-elastic vessels, that is, large arteries. The main pathogenetic events of atherosclerosis are lipid infiltration of the inner membrane of blood vessels and the proliferation of connective tissue in the vascular wall. At the first stages of the pathological process, lipid infiltration takes the form of a so-called fatty stripe, which does not rise above the surface of the vascular wall. However, further proliferation of connective tissue leads to the formation of an atherosclerotic plaque, which reduces the lumen of the vessel. Closure of the vessel lumen by 70% or more is considered a hemodynamically significant stenosis, in which the risk of ischemic complications is very high. In the presence of a large atherosclerotic plaque, the risk of violating the integrity of the vascular wall with the subsequent development of thrombosis is very significant. Atherosclerosis is an almost universal pathological process that develops in the vast majority of people. At the same time, according to pathoanatomical research methods, the first signs of atherosclerosis are often detected already at 15–20 years of age. The main risk factors for atherosclerosis are listed in Table 1 [2,4]. Clinical picture of atherosclerosis of the cerebral arteries Of the main arteries of the head, atherosclerosis most often affects the carotid arteries. In particular, the typical location of an atherosclerotic plaque is the bifurcation of the common carotid artery into the internal and external carotid arteries. A physical sign of a stenotic process in this localization is a systolic murmur, which is heard during auscultation of the carotid arteries. It should, however, be noted that when the artery is completely blocked, there is no systolic murmur. More reliable methods for diagnosing atherosclerosis are ultrasound duplex scanning of the main arteries of the head, magnetic resonance or x-ray angiography [2,4]. Hemodynamically significant atherosclerotic stenosis is one of the main causes of cerebrovascular disorders, such as transient ischemic attacks, ischemic stroke and dyscirculatory encephalopathy (Table 2) [2,4,23]. Transient ischemic attack (TIA) is a transient disorder of cerebral circulation, which is based on local cerebral ischemia, leading to the formation of short-term neurological deficit. By definition, TIA symptoms resolve within 24 hours (either alone or with therapy); otherwise it is an ischemic stroke. The risk of TIA increases with a combination of hemodynamically significant atherosclerosis and systemic hemodynamic disorders (fall in blood pressure, cardiac output), which lead to decompensation of cerebral blood flow. In addition, TIAs can develop as a result of microembolism with fragments of an atherosclerotic plaque or thrombotic masses when the integrity of the vascular wall in the area of stenosis is violated [2,4,23]. A variant of ischemic stroke associated with atherosclerosis of the main arteries of the head is called atherothrombotic stroke. As can be seen from this term, it is based on two pathological processes: atherosclerosis, which, when the integrity of the vascular wall is violated, is complicated by thrombosis. The development of thrombosis leads to complete occlusion of the main artery or to arterio-arterial embolism. Atherothrombotic stroke is often preceded by TIA in the same pool. Complete occlusion of a large artery often develops gradually over several hours (the so-called progressive stroke) and leads to the formation of large cortical infarcts with significant neurological symptoms [2,4,23]. Along with acute disorders, atherosclerosis is one of the main causes of chronic cerebral vascular insufficiency, which in domestic neurological practice is referred to as dyscirculatory encephalopathy (DE). The expressions “chronic cerebral ischemia”, “ischemic cerebral disease”, “angioencephalopathy” and some others are sometimes used as a synonym for DE. From our point of view, the term “dyscirculatory encephalopathy” is the most accurate, since it reflects the localization of the lesion (encephalopathy) and its nature (dyscirculation, acute or chronic) [4,23]. During DE there are three main stages (Table 3). At the third stage of this disease, in most cases, vascular dementia syndrome is observed, and the neurological status is determined by a combination of pseudobulbar, pyramidal, extrapyramidal and ataxic syndromes (often in combination with pelvic disorders) [5,27,28]. Peripheral arterial insufficiency Cerebrovascular disorders are only one of the manifestations of systemic atherosclerosis and, as a rule, are combined with damage to other target organs. In particular, cerebrovascular accidents are often combined with peripheral arterial insufficiency, the main manifestation of which is vasogenic intermittent claudication. Population studies indicate that the incidence of vascular intermittent claudication in the age range from 55 to 74 years is 4.5%. Another 8% of people in the same age group have asymptomatic atherosclerotic stenoses of the abdominal aorta and vessels of the lower extremities [37]. Atherosclerosis of the lower extremities is combined with coronary heart disease in 70% of cases and with cerebral vascular insufficiency in 25% of cases [7,19]. Basic principles of therapy for atherosclerosis The main methods of treating atherosclerosis of the cerebral and peripheral arteries are vascular surgery, antiplatelet, lipid-lowering therapy and effects on the microvasculature. To prevent stroke and other cerebrovascular disorders in the presence of hemodynamically significant stenosis of the main arteries of the head, carotid endarterectomy or stenting of the carotid arteries is performed. Currently, the preventive effect of surgery is considered proven in patients with TIA, minor stroke, or stroke with minimal history of neurological deficit. A more complex question is about the advisability of surgical treatment of asymptomatic (before the development of TIA or stroke) stenosis of the cerebral arteries. In these cases, convincing data confirming the preventive effect of surgery has not yet been obtained [2,4]. For atherosclerosis of the vessels of the lower extremities, the indication for surgical treatment is 2B and later stages of the pathological process according to the A.B. classification. Pokrovsky (Table 4) [7, 20]. The presence of atherosclerotic stenosis of large arteries is an absolute indication for the prescription of antiplatelet drugs. Drugs with proven antiplatelet activity include acetylsalicylic acid in doses of 50–100 mg per day and clopidogrel in a dose of 75 mg per day. According to statistics, antiplatelet therapy reduces the risk of myocardial infarction, ischemic stroke and peripheral thrombosis by 20–25%. However, wide variability in individual response to antiplatelet therapy is known. In particular, in some patients (especially women), when acetylsalicylic acid is prescribed, a paradoxical increase in the aggregation of blood cells is observed. Therefore, after prescribing antiplatelet therapy, laboratory testing of the state of hemostasis is necessary to monitor its effectiveness [2,4]. In the presence of hemodynamically significant stenosis of cerebral or peripheral vessels, the need to use lipid-lowering drugs to prevent further increase in atherosclerosis can be discussed. Currently, lipid-lowering drugs from the group of statins are most widely used. These drugs are certainly indicated in the presence of hypercholesterolemia that cannot be corrected by diet. In some cases, it is practiced to prescribe statins even with normal levels of atherogenic cholesterol in the presence of a high risk of developing ischemic complications (in particular, in patients with diabetes mellitus, coronary heart disease, etc.) [32]. In the presence of cerebral or peripheral atherosclerosis, it is necessary to correct other existing vascular risk factors, such as arterial hypertension, smoking, alcohol abuse, diabetes mellitus, obesity, physical inactivity, etc. However, caution should be exercised when administering antihypertensive therapy to patients with severe stenosis of the main arteries of the head . In these cases, an excessively rapid and pronounced decrease in blood pressure does not reduce, but on the contrary, increases the risk of ischemic stroke [2,4]. Correction of microcirculatory disorders An important strategy for the treatment of atherosclerosis is drug optimization of blood circulation in the microcirculatory bed. The impact on microcirculation is justified in both cerebral and peripheral arterial insufficiency. For this purpose, so-called vasoactive (“vascular”) drugs are used. These include phosphodiesterase inhibitors (theophylline, pentoxifylline, vinpocetine), calcium channel blockers (cinnarizine, flunarizine, nimodipine) and α-blockers (nicergoline). One of the most promising vascular drugs for the treatment of cerebral and peripheral arterial insufficiency is Tanakan, which has a multidirectional positive effect on microcirculation and neuronal metabolism [9,35,39]. Tanakan is a standardized and titrated extract from natural raw materials. The drug acts on all parts of the vascular bed (arterioles, capillaries, venules). The experiment proved that when using the drug, spasmodic or sclerotic microvessels expand to a greater extent, that is, the “stealing effect” does not develop [35]. Evidence of the positive effect of Tanakan on microcirculation was obtained both in experimental and clinical studies using capillaroscopy and radionuclide research methods [1,6,11,12,14,15,24,39,41]. Clinical experience in using Tanakan spans more than 20 years and is based on a reliable evidence base. In Western European countries, the effectiveness of Tanakan for chronic cerebral vascular insufficiency was studied in detail in the 80–90s of the 20th century. It has been shown that with the use of Tanakan, there is an improvement in memory and other cognitive functions in patients with vascular dementia and less severe cognitive impairment. The positive effect of therapy was recorded using clinical, neuropsychological and electrophysiological research methods [9,30,36,38,40]. It should be especially emphasized that, according to the EPIDOS retrospective study, elderly people using Tanakan for a long time are characterized by a significantly lower risk of developing dementia than those who take other vascular drugs or are not treated at all [31]. In Russia, to date, sufficient experience has also been accumulated in the use of Tanakan both for cerebral and peripheral circulatory disorders. In 1998 N.N. Yakhno et al. used this drug in patients with early forms of chronic disorders of cerebral blood flow [26]. The therapy has been shown to have a positive effect on memory, concentration and attention span, associative processes, and psychomotor functions. According to electrophysiological research methods, after treatment, a significant decrease in the relative power of slow-wave activity was recorded. The effect of therapy was quite stable, as evidenced by follow-up observations of some patients [22]. The effectiveness of Tanakan in cerebral vascular insufficiency has been studied in Russia and the CIS countries in at least 10 clinical studies [1,3,6,11,14,15,17,21,35]. In total, more than 500 patients took part. Of these, 100 had a history of surgical interventions on the main arteries of the head (study by L.A. Dzyak et al. [6]), 90 patients had been exposed to penetrating radiation in the past (study by G.M. Rumyantseva et al. [21], B L. Malygina et al. [15]). 30 patients, in addition to DE, suffered from obliterating atherosclerosis of the lower extremities (study by V.V. Shprakh et al., [24]). The effectiveness of Tanakan was assessed using formalized clinical scales and questionnaires, which quantified subjective and objective neurological symptoms, cognitive, emotional-affective and behavioral disorders. In addition, 5 studies used neuropsychological methods [1,6,15,21,24], 3 used Doppler ultrasound [6,14,24], and 2 studies used capillaroscopy of bulbar conjunctival vessels [6,10]. Tanakan was prescribed in doses of 120–160 mg/day. within 45–90 days. All studies showed a beneficial effect of Tanakan on the clinical condition of patients, indicators of psychometric scales and neuropsychological tests. A number of studies have noted an improvement in cerebral hemodynamics according to ultrasound data, optimization of the bioelectrical activity of the brain, and normalization of the capillaroscopic picture. The greatest effect was observed in non-severe neurological disorders, which indicates the advisability of the earliest use of Tanakan for DE [14,17]. The positive effect of Tanakan on cognitive functions was recently demonstrated again in a large-scale multicenter study in patients with mild cognitive impairment syndrome in old age (study coordinator - Academician of the Russian Academy of Medical Sciences, Prof. N.N. Yakhno). It has been shown that the use of this drug for 6 months contributes to a significant regression of the severity of memory, attention, dyspractical and intellectual impairments. Moreover, the severity of the positive effect at the 6th month of treatment was significantly greater compared to the 3rd month, which indicates the advisability of longer courses than is usually accepted in neurological practice [28]. It should be noted that, being a drug of natural origin, Tanakan is characterized by a favorable safety and tolerability profile, which allows it to be used for a long time without fear of causing any harm to health. Today there is also serious experience in using Tanakan for peripheral arterial insufficiency. U. Bauer investigated the effectiveness of Tanakan in obliterating atherosclerosis of the lower extremities in a double-blind, placebo-controlled study. Patients received the drug at a dose of 120 mg/day. within six months. After the course of treatment, a significant increase in the walking distance before the onset of pain was recorded compared to placebo [33]. Similar results were obtained in the work of ED Berndt and M. Kramar. At the same time, the superiority of Tanakan over buflomedil was shown [34]. The effectiveness of Tanakan in obliterating atherosclerosis of the lower extremities was also studied by V.M. Koshkin et al. The drug was prescribed at a dose of 160 mg/day. during three months. It has been shown that treatment with Tanakan helps to increase the distance of pain-free walking and reduce the frequency of cramps in the calf muscles. In addition, a decrease in the severity of dizziness and an increase in potency were noted [10]. The same Tanakan effects were shown in the work of A.V. Pokrovsky and A.V. Chupin, who used the drug at a dose of 80 mg/day. for 90 days in 30 patients with obliterating atherosclerosis of the lower extremities [18]. The positive effect of Tanakan in this pathology is also reported by Yu.V. Lukyanov [13]. In a number of studies, during Tanakan therapy, an increase in regional systolic pressure and systolic frequency according to Doppler ultrasound was noted, which indicates an increase in blood supply to the lower extremities [16,24,25]. O.A. Lobut et al. Tanakan was used at a dose of 120 mg/day. for 3 months in patients with ischemic lesions of the upper extremities. It has been shown that a course of therapy helps to reduce the severity of subjective symptoms, such as numbness of the fingers, cold hands, dry skin, and hyperhidrosis. Positive dynamics were also noted according to Doppler ultrasound data [12]. Thus, the results of the studies and many years of clinical practice confirm the undoubted feasibility of using long-term repeated courses of Tanakan in the management of patients with cerebral and peripheral arterial insufficiency.
Literature 1. Astapenko A.V., I.P. Antonov, V.B. Shalkevich, G.I. Ovsyankina. Application of tanakan in neurological practice. // Journal. Medical news. -Minsk. –1999. –No. 1–2. –P.32–33. 2. Warlow C.P., M.S.Dennis, J.van Geyn et al. Stroke. Practical guide for the management of patients // Transl. from English –SPb. –1998. –P.629 3. Gavrilova S.I., I.V.Kolykhalov, I.M.Milopolskaya, M.A.Morozova, N.D.Selezneva. Tanakan in the treatment of initial manifestations of cerebrovascular insufficiency. //Clinical gerontology. –1995. –No. 4. –P.22–23. 4. Damulin I.V., Parfenov V.A., Skoromets A.A., Yakhno N.N. Poor circulation in the brain and spinal cord. //In the book: “Diseases of the nervous system. A guide for doctors." Ed. N.N. Yakhno, I.V. Damulina. –M.: publishing house “Medicine”. –2001. –T.1. –P.239–302. 5. Damulin I.V. Alzheimer's disease and vascular dementia. //Ed. N.N. Yakhno. –M. –2002. –P.85. 6. Dzyak L.A., V.A. Golik, I.V. Rozhkova. Experience of using tanakan in the treatment of cerebral ischemia caused by pathology of the main arteries of the head in the postoperative period. Materials of the scientific and practical sympium “Tanakan”. – Kyiv. –1997. – Abstracts of reports. –P.5–6. 7. Zatevakhin I.I., Zolkin V.N., Stepanov N.V., Tsitsiashvili M.Sh. Obliterating diseases of the aorta and lower extremities. //Russian medical journal. –2001. –No. 3–4. –pp.126–131. 8. Zakharov V.V., I.V.Damulin, N.N.Yakhno. Drug therapy for dementia. Clinical pharmacology and therapy. –1994. –T.3. –No. 4. –P.69–75. 9. Zakharov V.V. Application of tanakan in neurogeriatric practice. //Neurological journal. –1997. –T.5. –P.42–49. 10. Koshkin V.M. Conservative treatment of chronic obliterating diseases of the arteries of the extremities.//Russian Medical Journal. –1997. –T.6. –No. 13. –P.820. 11. Lazebnik L.B., S.B. Malichenko, Yu.V. Konev. Tanakan in the treatment of initial manifestations of vascular dementia in the involutionary period. //Scientific and practical conference “Elderly patient. The quality of life". –M. –1996. – Abstracts of reports. –P.119. 12. Lobut O.A., N.P. Makarova. Clinical use of tanakan in patients with chronic ischemia of the upper limbs. //In: Tanakan: experience of application in medical practice in the CIS countries. –M. –2001. –P.77. 13. Lukyanov Yu.V. Evaluation of the effectiveness of treatment of patients with obliterating atherosclerosis of the lower extremities. //Materials of the anniversary conference for the centenary of St. Petersburg State. Honey. University. –S–Pb. –1997. – Abstracts of reports. –P.192. 14. Malakhov V.A., E.V. Kochueva. Comparative effectiveness of vinpocetine and tanakan (Egb 761) in monotherapy of patients with initial forms of cerebrovascular diseases. //Pharmacological information. -Kyiv. –chest 1997. –C50–52. 15. Malygin V.L., V.A. Zherebtsova, E.A. Atlas. //Tanakan in the treatment of cerebral vascular disorders in persons exposed to low doses of radiation. //6th Russian National Congress “Man and Medicine”. –M. –1999. – Abstracts of reports. –P.99. 16. Naumov S.S. Results of the use of tanakan in patients with chronic arterial insufficiency of the vessels of the lower extremities in a clinic. // In: Tanakan: experience of application in medical practice in the CIS countries. –M. –2001. –P.73–74. 17. Pirogova L.G., G.S. Nietkalieva. The use of tanakan in the treatment of patients with discirculatory encephalopathy stage II–III who have suffered minor strokes and lacunar infarctions. //News in Medicine and Pharmacy Newsletter. -Almaty. –1998. –No. 2. –P.4. 18. Pokrovsky A.V., A.V. Chupin, O.G. Gryaznov. Clinical trial of the drug tanakan in patients with atherosclerotic lesions of the arteries of the lower extremities. //International symposium “Conservative therapy in angiology. Experience in using Tanakan and Gingko Fort preparations.” –M. –1997. – Abstracts of reports. –P.37. 19. Pokrovsky A.V., Koshkin V.M., Kirichenko A.A. et al. Vasaprostan (prostaglandin E1) in the treatment of severe stages of arterial insufficiency of the lower extremities. //Manual for doctors. –M. –1999. –16C. 20. Pokrovsky A.V., Abramova N.N., Anbatiello S.G. Clinical angiology. Guide for doctors. //Ed. A.V. Pokrovsky. -Moscow. –2004. –T.1. –808С. 21. Rumyantseva G.M., I.M.Milopolskaya, A.V.Grushkov, O.V.Chinkina, T.M.Levina, T.N.Sokolova. The effectiveness of treatment with tanakan in patients with borderline psychoorganic syndrome who have received various doses of ionizing radiation in the past. //Russian Psychiatric Journal. –1999. –No. 1. –P.31–36. 22. Timerbaeva S.L., Z.A. Suslina, E.A. Bodareva, P.A. Fedin, O.S. Korepina, B.E. Pervozvansky. //Tanakan in the treatment of initial manifestations of insufficiency of blood supply to the brain: effectiveness, tolerability and long-term results.//J. Neurology and Psychiatry named after. S.S. Korsakov. –1999. –P.54–61. 23. Shmidt E.V. Classification of vascular lesions of the brain and spinal cord. // Journal of neuropathology and psychiatry. –1985. –No. 9. –P.1281–1288. 24. Shprakh V.V., V.V. Chernyavsky, M.B. Tatarinova, A.L. Tarabin, I.V. Shalamova. Features of the clinic, diagnosis and treatment of cerebrovascular diseases in persons with obliterating atherosclerosis of the main and peripheral arteries. //Collection of scientific and practical articles “Problems of clinical angiology and vascular surgery”. –Issue 1. -Irkutsk. –1998. –100–107. 25. Yanushko V.A. The use of tanakan for obliterating diseases of the vessels of the lower extremities. //Healthcare. -Minsk. –1999. –No. 6. –P.54–56. 26. Yakhno N.N., I.V.Damulin, V.V.Zakharov, M.N.Elkin, L.G.Erokhina, L.V.Stakhovskaya, N.S.Chekneva, Z.A.Suslina, S.L. Timerbaeva, P.A. Fedin, E.A. Bodareva, A.A. Skoromets, V.A. Sorokoumov, V.T. Ivashkin, Yu.V. Gigorev, B.E. Pervozvansky. The use of tanakan in the initial stages of cerebrovascular insufficiency: results of an open multicenter study. //Neurological journal. –1998. –T.3. –P.18–22. 27. Yakhno N. N., Levin O. S., Damulin I. V. Comparison of clinical and MRI data in dyscirculatory encephalopathy. Message 1: movement disorders // Neurol. magazine – 2001. – N 2. – pp. 10–16. 28. Yakhno N. N., Levin O. S., Damulin I. V. Comparison of clinical and MRI data in dyscirculatory encephalopathy. Message 2: cognitive impairment // Neurol. magazine – 2001. – N 3. – P. 10–19. 29. Yakhno N.N., Zakharov V.V., Lokshina A.B. et al. Tanakan (EGB 761) in the treatment of moderate cognitive impairment. //AND. neuropathology and psychiatry. -2007 (in print). 30. Arrigo A. Die Behandlung der chronischen zerebrovaskularen Insuffizienz mit Ginkgo biloba extrakt.//Therapiwoche. –1986. –V.36. –P.5208–5218. 31. Andrieux S, Amouyal K, Renish W, et al. The consumption of vasodilators and Ginkgo biloba (Egb 761) in a population of 7598 women over the age of 75 years. // Research and practice in Alzheimer's disease. –2001. –V.5. –P.57–68. 32. Baiqent C, Keech A, Kearney PM et al. Efficacy and safety of cholesterol lowering treatment: prospective meta–analysis of data from 90056 participants in 14 randomized trials of statins. //Lancet. –2005. –V.366. –N.9493. –P.1967–1978. 33. Bauer U. Etude clinic d L'EGb 761 dans l'artertedes members inferieurs. Essai a double insu face au placebosur 6 mois. //Arzneim Forsh Drug Res. –1984. –V.34. –N.6. –P.716–720. 34. Berndt ED, M. Kramar. Traiement medicamente ux des members inferieurs au stade 2b. //Therapiewoche. –1984. –V.187. –N.37. –P.2815–2819. 35. Clostre F. De l'organisme aux membranes cellulaires: lex differents niveuax d'actions pharmacologiques de l'extrait de Ginkgo biloba. //Presse Med; –1986. –V.15. P.1529–1538. 36. Dieli G., V. LaMantia, M. Saetta, E. Constanzo. Studio clinico in doppio cieco del Tanakan nell'insufficienza cerebrale cronica. //Lav Neuropsychiatr. –1981. –V.68. –P.3–15. 37. Fowkes FG, Housley E, Cawood EH et al. Edinburgh artery study: prevalence of asymptomatic and symptomatic peripheral arterial disease in the general population. //Int J Epidimiol. – 1991. –V.20. –P.384–392. 38. Israel L., E. Dell'Accio, G. Martin, R. Hugonot. Extrait de Ginkgo biloba et expercises d'entrainement de la memoire. Evaluation comparative chez des personnes agees ambulatoires. //Psychol Med. –1987. –V.19. –P.1431–1439. 39. Kleijnen J., P. Knipschild. Ginkgo biloba. //Lancet.–1992. –V.340: Nov 7.–P.1136–1139. 40. Pidoux B., C.Bastein, S.Niddam. Clinical and quantitative EEG double–blind study of GBE. //J Cerebral Blood Flow Metabolism. –1983. –V.3. –P.5556–5557. 41. Spinnewyn B. Ginkgo biloba extract (EGb 761) protects against delayed neuronal death in gerbil. //In: Y.Christen, J.Costentin, M.Lacour (eds): Effects of Ginkgo biloba extract (EGb 761) on the central nervous system. Advances in Ginkgo biloba Extract research. –Elsevier, Paris. –1992.–P.113–118.
Stroke
Stroke is the main cause of disability in the population. Only about 20% of surviving patients can return to their previous jobs. At the same time, a stroke imposes special obligations on the patient’s family members and places a heavy socio-economic burden on society.
Ischemic stroke
- This is the death of parts of the brain due to insufficient blood supply to them through the arteries. The brain receives nutrition from two carotid and two vertebral arteries. About 80% of ischemic strokes occur due to damage to the carotid or vertebral arteries in the neck. The vast majority of narrowings of the arteries arise due to the deposition of atherosclerotic plaques in the vessel wall, which not only cause insufficient blood flow to the brain, but are also destroyed with the formation of small or massive blood clots, causing either an extensive stroke or many small ones, leading to a significant decrease in intelligence and dementia.
The presence of atherosclerotic plaques in the vessels supplying the brain is often difficult to suspect, since the complaints are varied and inconsistent. The main precursors to the development of a major stroke are the so-called transient ischemic attacks (TIA), which occur when small fragments of an atherosclerotic plaque tear off and enter small vessels of the brain, causing brain death in a small area. In this case, transient paralysis of the arms and/or legs (from several minutes to several hours), speech impairment, transient or sudden blindness in one eye, memory loss, dizziness, and fainting are possible.
Presence of TIA
- This is an alarming warning signal that your brain is in serious danger and you need to undergo examination and begin treatment as soon as possible.
Modern capabilities of cardiovascular surgery make it possible to save life and improve its quality for most patients and to prevent ischemic disorders of cerebral circulation. The clinic's cardiovascular surgeons have modern equipment, unique plastic materials and surgical treatment technologies in their arsenal. In some cases, intravascular elimination of narrowing of the carotid artery is possible without anesthesia and an incision through a puncture of the artery and the introduction of a special instrument into its lumen under X-ray control.
Stenosing atherosclerosis MAG - what is it?
Stenotic atherosclerosis is a pathology of blood vessels. Fatty deposits, called cholesterol plaques, form on the inner walls of these vessels.
What is important is that the disease is not sudden. Its development occurs over a long period of time, with the slow formation of plaques.
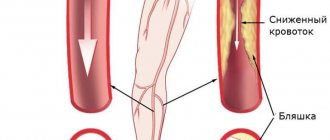
There is a process with the formation of calcifications and the gradual proliferation of connective tissues. The mechanism of occurrence and spread of the disease in the body comes down to the accumulation of low-density fats in the blood. Over time, they stick to the slightest irregularities inside the vessels and form plaques, which, as the disease progresses, lead to blockage of the arteries. As a result, the clearance for blood flow decreases to such an extent that the blood supply is completely disrupted, leading to ischemia of organs and tissues.
Basic methods of treating atherosclerosis of the brachiocephalic arteries
Unfortunately, there are no drugs yet that can “dissolve” or eliminate plaques in blood vessels. Some drugs, such as aspirin and cholesterol-lowering drugs, can only stop the growth of atherosclerotic plaques and reduce the likelihood of blood clots. The main and only effective method of treating narrowing and occlusion of the carotid, vertebral, and subclavian arteries is surgery. Numerous studies by scientists from various countries have indisputably proven the effectiveness of preventive surgical methods in preventing stroke.
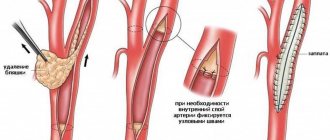
Open operations can be as follows:
- classic carotid endarterectomy with artery patch plasty,
- eversion carotid endarterectomy,
- internal carotid artery replacement,
- carotid-subclavian shunting.
Minimally invasive methods:
- carotid angioplasty with stenting,
- stenting of the subclavian artery,
- vertebral artery stenting.
The choice of treatment method is based on a comprehensive examination of the patient and is prescribed based on many factors, according to strict indications based on Russian national recommendations for the management of patients with vascular arterial pathology.
Causes and risk factors
The main cause of stenosing atherosclerosis is age-related changes occurring in the body.
The most obvious causes of the disease include:
- Hypertension.
- Diabetes.
- Genetic predisposition.
- Obesity (any degree of severity).
- Gender (men are more susceptible to developing stenotic atherosclerosis).
- Poor nutrition, consumption of large amounts of unhealthy, cholesterol-rich foods.
- Physical inactivity.
It is also important to keep in mind the existence of certain risk factors:
- Bad habits (smoking, drinking large amounts of alcohol).
- Nervous overload, constant state of anxiety, stress.
Reference! The disease can manifest itself in various parts of the body, but the lower extremities are most susceptible to negative changes as a result of the development of the disease.
To a large extent, this process is influenced by a person’s lifestyle and the conditions in which he works. The most obvious provocateurs of stenosing atherosclerosis of the lower extremities are considered to be injuries and severe hypothermia.
It is important to know!
- 70% of all strokes “live” in the carotid arteries.
- If you or your relatives have experienced symptoms of CNM, stroke, TIA, do not risk your life and consult a cardiovascular surgeon and doctors at the Department of X-ray Endovascular Diagnostics and Treatment - your family needs you!!!
- Stroke can and should be prevented.
- Atherosclerotic plaques do not dissolve!!!
- The benefit of surgery is always greater than the risk associated with it.
Varieties and its manifestations
There are several types of stenosing atherosclerosis:
Stenosing atherosclerosis of the main arteries of the head (MAG). One of the most serious types of stenosing atherosclerosis in its manifestation, since it can cause the development of brain failure. The manifestation of atherosclerosis MAG can be divided into 3 groups of symptoms.- The first (general cerebral symptoms) include: memory impairment, headaches, decreased brain activity.
- The second (manifestations of an ocular nature): attacks of sudden deterioration of vision or partial blindness.
- And finally, to the third (hemispheric symptoms): facial asymmetry, speech impairment, pain during movement.
Stenosing atherosclerosis of the brachiocephalic arteries (BCA). With the development of this type of disease, the following is observed:- dizziness;
- constant heavy snoring;
- bad feeling;
- pressure surges, etc.
Stenosing atherosclerosis of cerebral arteries. Manifests itself predominantly in a number of neurological symptoms:- headache;
- memory impairment;
- organic vision lesions (in some cases);
- impaired speech clarity and many other unpleasant symptoms of the disease.
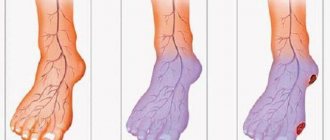
Stenosing atherosclerosis of the lower extremities. In the initial stages, there is a feeling of chilliness and tingling in the legs, numbness in some areas of the foot. As the disease progresses, lameness begins to clearly appear, eventually becoming pronounced. In the final stages of development of the disease, the feet swell, atrophic ulcers appear on them, which subsequently leads to the occurrence of gangrene.
Preventive measures
To prevent the development of the disease and the manifestation of its complications, it is necessary to strictly follow the doctor’s instructions. The following tips should be followed to prevent illness:
- Strict control over blood pressure.
- Carrying out regular (moderate) physical activity (fitness, yoga, swimming, running, walking in the fresh air, etc.).
- Refusal of bad habits (if any are present in life).
- A balanced, healthy diet rich in antioxidants and vitamins.
- Regular preventive examinations by a specialist.
How effective is treatment of the disease with folk remedies (herbs), read here; and how to deal with the disease - follow the link.
Consequences and complications
Late detection of the disease and lack of proper treatment can lead to irreversible and very serious consequences. For example, damage to the carotid arteries can provoke a stroke, and severe blockage of the main arteries of the head can lead to massive hemorrhages. There are a number of complications provoked by the rapid progression of the disease:
Spicy. The development of the disease can lead to serious disorders of cerebral and cardiac circulation (aortic aneurysm, gangrene, ischemia of the heart muscle, etc.).- Chronic. Insufficient blood circulation in the diseased parts of the body leads over time to functional and then organic (unfortunately, irreversible) changes. So, if atherosclerosis of the BCA was detected untimely or treatment was not prescribed on time, the patient will eventually develop a neurological disorder in the brain. Dementia often develops on this basis.