What it is
Sudden contractions of the left or right ventricles of the heart are associated with the appearance of foci of excitation in the Purkinje fibers or in the distal areas after the branching of the His bundle branches. This phenomenon can be observed in severe diseases of the heart muscle caused by intoxication, overexcitation, and congenital characteristics of the conduction system of the heart.
Single ventricular extrasystoles are observed normally in completely healthy people. They usually do not manifest themselves clinically and do not require special treatment. With age, their number increases.
Complications
Pathological ventricular extrasystole, especially without properly selected treatment, if all medical prescriptions are not followed, can lead to serious complications. Why is it dangerous:
- may lead to changes in the ventricles of the heart;
- worsen the functioning of the heart - it becomes unable to properly pump blood throughout the body, cardiac output decreases;
- frequent extrasystoles further aggravate the current disease of the cardiovascular system;
- ventricular fibrillation may occur, which in turn often leads to death;
- the risk of sudden cardiac arrest increases.
Causes
To understand the etiology of the appearance of such arrhythmia, it is most convenient to present all the factors in the form of a table:
| Kinds | Cause | How to suspect |
| Organic |
| The symptoms of the underlying pathology come first; extrasystole acts as a complication. |
| Extracardiac |
| Studying anamnesis, checking the functioning of internal organs, studying the ionic composition of the blood, ultrasound and x-ray diagnostics. |
| Functional |
| There is a clear connection between the development of arrhythmia after exposure to a provoking factor, and the absence of organic changes. |
| Idiopathic | No connection with disease or other factors | Only with the help of ECG and Holter monitoring. |
For any disease, the only examination that will clearly show the presence of additional ventricular contractions is electrocardiography. If it is not possible to register a deviation during an ECG, then a special device is used that records heart activity over a given time.
Symptoms and manifestations
Most often, single extrasystoles appear without clinical symptoms. According to statistics, interruptions in this case develop in 30% of patients, and approximately 7% believe that this phenomenon significantly worsens their well-being. The patient’s complaints at the time of the onset of arrhythmia are as follows:
- heart sinking, tremors and interruptions;
- dizziness and general weakness;
- shortness of breath, lack of air;
- volley and frequent ventricular extrasystoles can cause pain against the background of an ischemic attack and impaired consciousness.
I have often noticed that additional myocardial contractions of functional origin often cause significant symptoms. But disturbances against the background of organic changes of a chronic nature are not perceived, as if a person is getting used to them.
Classification and types
There are several types of classifications to determine the type of a given arrhythmia. They are important for establishing the cause of the pathology, accurate diagnosis, treatment approach and further prognosis.
According to the frequency of occurrence, the following ventricular extrasystoles are distinguished:
- rare (less than 5 per minute);
- medium frequency (up to 16/min);
- frequent (16 or more).
By density:
- single;
- pairs;
- group.
By localization:
- right ventricular;
- left ventricular.
By localization of excitation:
- monomorphic (arise from one focus, have the same appearance on the ECG);
- polymorphic (different places of origin, complexes differ markedly when registered).
According to the rhythm of appearance:
- bigeminy (every second contraction is an extrasystole);
- trigeminy (every third);
- quadrigeminy (fourth);
- sporadic (excitations without a clear sequence).
According to the degree of danger, there are the following classes:
- Benign ventricular extrasystoles. They occur in the absence of myocardial damage or hypertrophy, their frequency does not exceed 10 per hour, and are not accompanied by impaired consciousness.
- Potentially malignant. Against the background of left ventricular dysfunction, with a frequency of 10 or more per minute. No fainting or cardiac arrest.
- Malignant. Frequent, polymorphic and polytopic, against the background of significant deviations (ejection fraction of 40% or less), turn into stable ventricular tachycardia. The medical history contains a description of impaired consciousness and (or) cardiac arrest.
Ryan gradation
My colleagues and I still use the classification of ventricular extrasystole (VC), proposed by M. Ryan in 1975; it is intended for patients who have a history of myocardial infarction. According to this gradation, the following degrees of arrhythmia development are distinguished:
| Stage | Description of extrasystoles |
| 0 | There are no episodes of sudden contractions |
| 1 | Number does not exceed 30 per hour, monotopic |
| 2 | More than 30 extrasystoles in 60 minutes, monotopic |
| 3 | Multifocal, frequent |
| 4a | Paired monotropic |
| 4b | Polymorphic, paired and grouped with flickering and fluttering |
| 5 | Early, salvo, polymorphic, turning into paroxysm of ventricular tachycardia |
Early ventricular extrasystoles have especially severe consequences for the patient’s life. They occur while the active phase of depolarization occurs, preventing the heart from relaxing for the next contraction.
Forecast
Having understood the classification of ventricular extrasystole, having understood what it is and against the background of what diseases it occurs, we should say a few words about the prognosis.
A functional VES does not pose a threat to life. It occurs in almost all people, and is often asymptomatic. Pathological extrasystoles require attention, correct diagnosis and treatment, since they can greatly worsen the quality of life, aggravate the underlying disease and increase the risk of sudden death.
Diagnostics
Diagnostics that determine rhythm disturbances are based on standard methods. First, a cardiologist or therapist conducts a survey, identifying the patient’s main complaints. Examination and auscultation help to detect signs of heart failure and suspect a valve problem.
ECG and Holter monitoring
The most effective method for accurately determining heart rhythm disturbances such as ventricular extrasystole is an electrocardiographic study. But it cannot 100% identify the problem, since additional stimulation does not always occur at the time of taking an ECG.
If it is necessary to establish a diagnosis, 24-hour monitoring is used, which is called Holter monitoring. It helps in determining any type of arrhythmia, especially if the deviation is transient. After recording the electrical activity of the heart, it becomes possible to:
- clarify the number and morphology of ventricular complexes;
- dependence of their appearance on physical activity or other factors;
- record changes depending on sleep or wakefulness;
- draw a conclusion about the effectiveness of drug therapy.
Electrocardiographic signs
On an ECG, ventricular extrasystole manifests itself as follows:
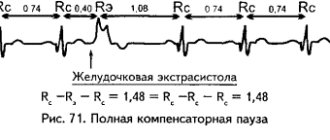
- The occurrence of an extraordinary QRS complex. It is characterized by the absence of an atrial wave, expansion and deformation. In this case, T has the opposite (discordant) direction. Most often, it is followed by a complete compensatory pause (isoline).
- Extrasystoles from the left ventricle are characterized by a tall and wide R wave, as well as a subsequent deep negative T wave in leads III, aVF, V1 and V2, as shown in the photo. At the same time, there is a deep and wide S, high T in I, II, aVL, V5 and V
- Complexes from the right ventricle present the opposite picture, +R and –T will be in I, II and left precordial leads. Negative R and positive T are in the right leads and aVF, the changes are clearly visible in the photo.
- There are interpolated (inserted) extrasystoles. On the cardiogram they appear as a deformed QRS complex, which is inserted between two normal contractions and does not have a compensatory pause. Often this phenomenon accompanies bradycardia, as can be seen in the photo.
More details on the electrocardiographic signs of extrasystoles can be found here.
Treatment
Treatment tactics after detection of ventricular extrasystoles depend on the presence of other diseases, symptoms, and threatening types of rhythm disturbances. If there are no complaints and rare emerging complexes are identified, no special therapy is required. A person is advised to give up caffeinated drinks, avoid alcohol and smoking.
If attacks are accompanied by clinical symptoms, but are benign and do not interfere with hemodynamics, beta blockers become the drugs of choice. Sometimes Valocordin or Corvalol helps stop an attack. In some cases, the problem can be eliminated with the help of Phenazepam.
Some specialists use class I antiarrhythmics in this case. But recent research confirms the inconsistency of this choice. It is especially dangerous to give these drugs in the presence of cardiac ischemia or during active myocarditis. The mortality rate of patients with the use of these drugs increases by 2.5 times.
In case of malignant extrasystole, the patient is placed in a hospital, where the following means are used:
- Amiodarone – used alone or in combination with beta blockers (Concor). This can significantly reduce the likelihood of death in patients with impaired cardiac blood flow. Treatment is carried out under the control of the QT interval.
- If Amiodarone is ineffective, Sotalol is used.
- If the problem is caused by an electrolyte imbalance, the patient receives potassium chloride or magnesium sulfate.
Treatment for a benign course continues for several months under ECG monitoring, then gradual withdrawal of antiarrhythmic drugs is recommended. Malignant pathology requires longer therapy.
How to relieve an attack
Frequent ventricular extrasystole is often observed in the first hours and days of acute myocardial infarction. It is dangerous due to the development of fibrillation and requires immediate relief. To do this, the following algorithm of actions is used:
- Intravenous administration of Lidocaine in a stream followed by a transition to a drip.
- If there is no result, switch to Novocainamide or Etatsizin.
- If palpitations are noted, beta blockers and Cordarone are used.
- For extrasystoles against the background of bradycardia, it is better to use Ethmozin or Ritmilen.
- Combining antiarrhythmic drugs is undesirable. This should only be done if absolutely necessary.
A detailed description of the use of drugs to relieve extrasystole is here.
When is surgery necessary?
The indication for surgery for this arrhythmia is the detection during daily monitoring of at least 8,000 extraordinary contractions throughout the year. In this case, the patient is recommended to undergo radiofrequency ablation (RFA).
The essence of this technique is that a catheter is inserted into the patient into a large-caliber vessel (this can be a vein under the collarbone or in the thigh area), which is guided under the control of equipment to the very heart. Then a radiofrequency pulse is applied to the site of pathological excitation (burning). I would like to note that such manipulation is usually successful, its effectiveness is 90%.
Prevention
The consequences of ventricular extrasystoles can be extremely dangerous, even fatal, so their prevention is important. It includes:
- Maintaining a healthy lifestyle. It is necessary to maintain a daily routine, allocate enough time for sleep and rest, and avoid excessive physical and emotional stress;
- Balanced diet. You should not eat a lot of fried, salty, spicy foods. It is useful to include foods containing large amounts of fiber in your diet;
- Rejection of bad habits. Alcohol and smoking aggravate many diseases of the cardiovascular system;
- Periodic examination of the body. It is necessary to consult a doctor in a timely manner if any complaints arise, and also periodically undergo age-related medical examinations;
- Treatment of diseases, compliance with all doctor’s prescriptions. You should not treat diseases yourself, using folk remedies, or voluntarily cancel or change the dosage of medications prescribed by a cardiologist.
Case from practice
A patient came to see me with a feeling of interruptions in the heart; during the attack, the extremities became cold, the pressure increased to 150/95 mm Hg. Art. There is no history of cardiac pathology. Indicates a worsening of arrhythmia with physical activity and alcohol intake. The ECG showed no deviation; after Holter monitoring, episodes of volley extrasystoles from the right ventricle were detected. After prescribing sedatives and a beta blocker (Bisoprolol), the patient was discharged after two weeks with improvement.
Expert advice
Detection of ventricular extrasystoles on an ECG is not yet a sign of a serious problem and does not require special treatment.
Functional rhythm disturbances are often accompanied by symptoms that do not correspond to the severity of the condition. To eliminate them, it is enough to remove alcohol from your diet, quit smoking and drink caffeinated drinks. Among the drugs you can drink valerian tincture, Corvalol. When extrasystole is accompanied by coronary disease or other disorders, you must immediately contact a cardiologist and undergo a full examination. All medications should be taken as scheduled and should never be discontinued on your own.
How to treat ventricular extrasystole
When treating ventricular extrasystole, classical drug therapy or surgery is used. The treatment regimen is always determined by a cardiologist.
In our center of the Federal Scientific and Clinical Center of the Federal Medical and Biological Agency there is a therapeutic department in which the patient can undergo all the necessary heart examinations and tests under the supervision of specialists.
The surgical department employs doctors with many years of experience who perform heart surgeries of any complexity. In the case of ventricular extrasystole, radiofrequency catheter ablation may be proposed - a targeted effect of the electrode on areas with impaired conductivity.