Dextrocardia is a fairly rare congenital defect in which the heart and large vessels are deviated to the right. In this case, symmetry is maintained in relation to the midline of the body. The first descriptions of the unusual location of the heart appeared in the 17th century.
As a rule, this defect is combined with displacement of all unpaired organs to the right side. According to statistical observations, 0.01% of the total population has dextrocardia.
Clinically it may not manifest itself at all. In modern conditions, it is detected during examination of a child in the maternity ward, and in an adult - during fluorography (fluoroscopy), ECG or other studies of the chest organs.
Kinds
Abnormal location of the heart can be caused by painful processes in neighboring organs. Such mechanical displacement is defined as secondary, and dextrocardia is considered pathological. It is possible with:
- pulmonary atelectasis (blockage of air outlet);
- pneumopleurothorax (collapse of airiness) of part or all of the lung due to rupture, injury, cavernous tuberculosis with the release of air into the pleural cavity;
- hydrothorax (fluid accumulation in the pericardial sac);
- the growth of a large tumor.
A true anomaly is of congenital origin.
Depending on the combination with other disturbed positions of internal organs, it is customary to distinguish:
- simple dextrocardia - the location of only the heart and blood vessels is mirrored;
- simultaneous dextroposition of the heart, parts of the digestive and respiratory organs;
- complete dextroposition of internal organs.
Causes and risk factors
Non-dominant (also called autosomal recessive) genes cause dextrocardia.
These abnormal genes cause the primordial tube, or heart tube, to change direction as the fetus develops in the womb.
Depending on the degree and timing of the reversal, the heart and abdominal organs may also develop in a reverse fashion.
Because recessive genes cause dextrocardia, a person must inherit a copy of the abnormal gene from both parents to develop the disease.
Dextrocardia is estimated to affect 1 in every 12,000 people. Dextrocardia situs inversus totalis affects approximately one in every 10,000 children. Gender, race and ethnicity do not appear to influence whether a person develops this disease or not.
How does the anomaly form?
It is believed that the fetal heart tube is formed already in the early stages of pregnancy (in the first 10 weeks). Its curvature to the right side leads to displacement, formation of the heart and great vessels on the right.
The fetus may simultaneously have other abnormalities of organs and systems associated with genetic mutations. The most studied mutations are the ZIC3Shh, Pitxz, HAND, and ACVR2 genes. Hereditary transmission of the anomaly is assumed.
The exact mechanism of dextrocardia has not been proven. In most cases, the heart functions normally. The child grows and develops without noticing the defect. Pediatricians observe such children at risk for the possibility of developing cardiac pathology.
Disease or not?
Modern medicine classifies this phenomenon as an anomaly of intrauterine development.
Dextrocardia is the name scientists gave it, because the word dexter is translated from Latin as “right”, and cardio is Greek for “heart”. Some people have a “mirror” arrangement of not only the heart, but also the liver, spleen, and appendix, then we are talking about such a diagnosis as “transposition of organs.” The famous Italian medical scientist Hieronymus Fabricius in 1606, during his anatomical studies, discovered the very first case of dextrocardia known to science. And in 1643, his colleague Marco Aurelio Severino described the transposition of organs, when they were all located “mirror” in a person.
The heart of the unborn child begins to form already in the third week of pregnancy, it is then that it is determined where it will be located: in the left or right side of the chest.
There is debate in the scientific community about the causes of dextrocardia. Over the years, everything was blamed on: infectious diseases; incorrect lifestyle of the expectant mother; fetal trauma during intrauterine development. Now most scientists are inclined to think that people are born right-hearted as a result of mutations in the genes HAND, ZIC3Shh, ACVR2, Pitxz. Moreover, such a rare feature can be inherited.
Doctors reassure patients with dextrocardia and their relatives: if a person does not have other congenital heart defects or intrauterine developmental anomalies, then he can live, study and work peacefully like everyone else. Many right-hearted people live to an old age, and some of them do not even realize that their internal organs are “mirror-like” until they consult a doctor.
Is it a danger to human health?
In the absence of concomitant pathology, dextroposition itself does not pose a health hazard and does not shorten a person’s life span. However, during diagnostic studies and surgical intervention, the likelihood of medical errors increases significantly.
Acute pathology may be missed due to the unusual location of neighboring organs. In transplantology we have to take this into account and adapt to the abnormal course of arteries, veins, and nerve plexuses.
Practice shows that people with dextrocardia are more prone to contracting infectious diseases, especially those complicated by pathology of the lungs and bronchi.
What other defects is it most often combined with?
Rarely does an isolated “simple” anomaly occur. Dystopia (disorder of arrangement) also affects other organs. The most common combinations are found in childhood in the form of:
- tetralogy of Fallot - dextroposition of the aorta, pulmonary stenosis or complete occlusion, ventricular septal defect, significant hypertrophy of the right ventricle;
- reverse position of the main arteries;
- ventricular and atrial septal defect;
- pulmonary stenosis;
- valvular endocardial defects;
- double ventricular outlet;
- two- or three-chamber heart.
During transposition, the aorta emerges from the right ventricle, and the pulmonary artery emerges from the left.
A great danger to the life of a newborn is represented by “blue” defects, which appear in the first hours after birth. The vital activity of internal organs depends on the speed of surgical intervention to eliminate the defect.
With “white” defects, oxygen deficiency manifests itself in preschool age. Therefore, there is time for examination and preparation for surgery. The combination with pathology of the digestive and respiratory organs is expressed in:
- heterotaxic syndrome - there is no spleen or there are several underdeveloped spleens, practically non-functional;
- primary ciliary dyskinesia - the pathology consists of underdevelopment of the ciliated epithelium of internal organs, occurs in ¼ of patients with dextrocardia, is accompanied by multiple bronchiectasis, impaired anatomical structure of the bronchi, trachea, larynx, infertility in men due to low sperm motility;
- genetic mutations on the thirteenth pair of chromosomes (trisomy) - manifested by multiple malformations (Patau syndrome), defects of the nervous system (brain), eyes (microophthalmia, congenital cataracts), extra fingers, cleft palate and lip, changes in the urinary and genital organs, causes intrauterine fetal death, born children rarely live more than five years.
Diagnosis of a pathological disease
Most cases of dextrocardia are diagnosed using an electrocardiogram (ECG) and chest x-ray.
An ECG with inverted or reversed electrical waves usually indicates dextrocardia.
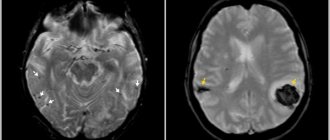
Once a doctor suspects dextrocardia, they may use computed tomography (CT) or magnetic resonance imaging (MRI) to confirm the condition.
Cartagena syndrome
Cartagena syndrome is when dextrocardia situs inversion is accompanied by primary ciliary dyskinesia, an inherited condition in which the cilia that help move mucus become immobile.
Approximately 20% of patients with dextrocardia also suffer from Cartagenere syndrome.
Dextroversion
Dextroversion occurs when the heart is incorrectly positioned further to the right and rotates to the right. The right ventricle usually follows the left, while the left remains left. This complication is diagnosed using an electrocardiograph (ECG).
Dextroposition
Dextroposition occurs when the heart becomes dislocated or moved to the right. Unlike dextrocardia, other organs are not mirrored.
This disease is usually associated with acquired diseases of the lungs, diaphragm, or pleura (the membranes surrounding the lungs).
Surgery and muscle damage or strain can also contribute to the development of dextroposition.
Doctors often use an ECG test to distinguish dextroposition from dextrocardia [KG3].
Large Vessel Rearrangement (TGA)
TGA occurs when the main vessels of the heart flow backward due to reversal of the heart chambers. This is a fairly rare disease.
Congenital corrected transposition of the great arteries (CCTGA).
This condition occurs when the lower half of the heart unfolds, especially the lower ventricles and connected valves.
The condition is even rarer than TGA, and the cause is still unknown. About 0.5 to 1 percent of all children born with heart disease have CCTGA, according to the Adult Congenital Heart Association.
Tricuspid atresia
This is a congenital defect in which the tricuspid valve does not develop. The tricuspid valve prevents blood from the right ventricle from flowing back into the right atrium.
Single-, double- and bicuspid ventricles or bicuspid ventricles
These cases occur when the aorta, which normally transports oxygenated blood from the left ventricle to the rest of the body, and the pulmonary artery, which carries deoxygenated blood from the right ventricle to the lungs, join in the same (left or right) ventricle.
pulmonary stenosis or atresia
It occurs when the heart's pulmonary (pulmonary) valve, which allows blood to leave the heart, becomes narrowed (stenosis) or fails to develop (atresia).
Heterotaxis
Heterotactic syndrome occurs when mirrored internal organs do not develop or function properly. Depending on the organs involved and the severity of the disease, heterotaxy can be life-threatening.
Endocardial cushion defect
This is a congenital heart defect in which the tissues separating the chambers of the heart do not develop, interfering with blood flow. This condition is also known as atrioventricular canal defect.
When the first signs of abnormal heart development appear, the doctor must prescribe a series of diagnostic procedures. The most common methods for diagnosing this disease include:
- general examination of the patient, auscultation and percussion. These methods make it possible to listen to the beats of the upper part of the heart on the right side. When palpating internal organs, it is necessary to remember that organs can also be located symmetrically;
- chest x-ray, which can be used to observe the abnormal position of the heart;
- ECG of the heart. An ECG with dextrocardia gives a picture as if the diagnostician made a mistake and installed the electrodes incorrectly. That is, the first lead will give a mirror image of the first, and the second and third will seem to be swapped. That is, the second lead will correspond to the third and vice versa;
- Ultrasound, CT, MRI;
- if necessary, the doctor may also prescribe an angiocardiogram or cardiac catheterization.
Are there typical symptoms of dextrocardia?
Dextrocardia does not manifest itself with any characteristic symptoms. A person with such an anomaly can live a normal life and suffer from various diseases. Indirect signs can be the phenomena of other combined defects leading to acute heart failure in early childhood.
These include:
- bluish or pale skin, especially when screaming;
- severe weakness;
- dyspnea;
- prolonged jaundice of the sclera and skin in a newborn;
- detection of arrhythmias.
Such symptoms in childhood require careful examination, searching for causes and deciding on treatment. During the neonatal period, the risk of sudden death increases sharply.
Parents and doctors have to nurse the baby for a long time in a specialized department
Older children are registered with a cardiologist and are checked at least twice a year.
How is diagnosis carried out?
The initial diagnostic procedure for a newborn is an examination by a neonatologist on the first day of life. Listening at typical points may indicate dextroposition of the heart. It is important to determine the type of defect, combination with additional anomalies.
An ultrasound examination can be performed in the maternity ward. The technique allows you to accurately determine the location of the heart and blood vessels and other organs. It is important that it is not dangerous for early childhood and helps to establish the degree of dysfunction.
Magnetic resonance imaging is considered a more accurate method. Provides maximum information about the work and anatomical structure of organs.
An electrocardiogram (ECG) can be performed on a small child only after first using sedatives. Since any movements disrupt the recording of potentials, making it unsuitable for decoding.
The image of the cardiac shadow on the radiograph appears to be a mirror image of the norm
The X-ray technician's first impression is that the person is standing with his back to the screen. First, he is asked to stand in front without looking, and then the thought of dextroposition arises. For older children and adults, X-rays are taken in frontal and lateral projections, and a full ECG examination is performed.
Features of ECG
If the heart is reversed and the electrodes are placed normally, the recording will show waves in the opposite direction. The picture is not similar to any other disease; it extends to the enhanced and chest leads. Accompanied by a sharp decrease in voltage.
The ratio of the height and depth of the teeth in conclusion indicates the likelihood of dextroposition. To diagnose heart disease in a patient with such an abnormality, an ECG is taken by moving the red electrode to the left hand and the yellow electrode to the right.
Chest leads are removed on the left and right
It is taken into account that even when the heart is displaced, its parts (atria and ventricles) are located normally in relation to the median axis (the right sections are on the right, the left atrium and ventricle are on the left). The impulse travels through the atria from right to left, then goes down the interventricular septum into the ventricles.
The norm for dextrocardia will be high ventricular complexes in chest leads V1–V3 and low ones in V4–V6.
Development mechanism
The question of whether dextrocardia is considered a disease has not yet been resolved. More and more doctors are inclined to believe that an uncomplicated process is not considered pathological. How is an anatomical disorder formed?
Conventionally, there are two types of this condition. True, when the anomaly is the result of the influence of perinatal factors, and false, it can be acquired and is always pathological.
In the first case, the main role is given to the genetic factor and random errors. The heart is formed in the second week of gestation and represents the rudiments of a full-fledged organ.
Under the influence of one factor or another, the tube shifts to the right and begins to develop from the opposite side.
The formation of other organs occurs in accordance with the new “configuration”.
There are three options:
- Isolated dextrocardia is an altered location of the heart and normal location of other internal organs.
- Partially combined - reverse arrangement of the heart and lungs (the left lung has three lobes, and the right lung has two).
- Complete - a mirror arrangement of the heart and the same transposition of the internal organs.
If a genetic defect is to blame, other defects also develop. Including those not related to cardiac structures.
A false form is the result of gross violations. Their influence occurs already in the second or third trimester.
There are known cases of organ displacement in older age. The classic variant is a lung tumor, usually malignant.
As it grows, it provokes a shift of the muscular heart to the other side, pushes it aside, and causes tissue compression.
In such a situation, doctors talk about dextroposition or false vice. We are talking about a disease, not a developmental feature.
Large neoplasias can cause significant displacement. Therefore, during auscultation (listening to tones), the heart will be detected on the other side.
The same effect is produced by a previous inflammatory disease (rarely), lung pathologies, or accumulation of fluid in the chest.
Are there preventive measures?
There is no special prevention for dextrocardia. To prevent any defects in the child, the mother must be prepared before pregnancy begins. Therefore, obstetricians-gynecologists advise a woman to plan a pregnancy, get examined and treat chronic diseases. It can be difficult to leave work in hazardous working conditions, but this significantly reduces the risk of pathology in the fetus.
Care should be taken when referring future parents who have relatives with developmental anomalies to genetic counseling.
Cardiac dextroposition is not a disease, but an anatomical feature. If it is detected, you must follow the doctor's recommendations. In adulthood, the patient must be warned about the developmental defect if an examination or operation is prescribed. Life activities may be limited only by concomitant anomalies or diseases.
Treatment
In most cases, dextrocardia has a favorable prognosis and does not require special treatment. Most often, the anomaly is discovered completely by accident during a medical examination or routine medical examination. Persons with this pathology lead a normal life, without any complications associated with their medical condition.
If dextrocardia is combined with a congenital heart defect, surgical treatment is performed. In advanced cases, surgical intervention is the only option to save the patient's life.
Conservative therapy is aimed at eliminating concomitant pathology. It alleviates the condition of patients and helps prepare the body for surgery.
Patients are prescribed:
- Drugs that support and strengthen the heart muscle - Trimetazidine, Panangin, Asparkam, Riboxin;
- Cardiac glycosides – “Strofanthin”, “Korglikon”;
- Diuretics – “Furasemide”, “Hypothiazide”, “Veroshpiron”;
- Hypotonics – “Enalapril”, “Captopril”, “Lisinopril”;
- Vitamin and mineral complexes;
- Plant adaptogens – Rhodiola rosea, Leuzea safflower, hawthorn;
- Nutritional supplements – omega-3, L-carnitine.
In order to prevent postoperative complications, antibacterial and immunostimulating therapy is carried out. Patients are usually prescribed broad-spectrum antibiotics from the group of cephalosporins, macrolides, and fluoroquinolones. To stimulate the immune system and maintain it at an optimal level, patients are prescribed drugs from the interferon group, Imunorix, Polyoxidonium, Bronchomunal.
Timely and correct treatment of patients avoids disability and death.