According to medical statistics, approximately 40% of men of fertile age experience difficulties in achieving a full erection. The penis is either not hard enough for penetration, or spontaneous premature ejaculation occurs. Both pathologies relate to impotence or sexual dysfunction (erection). Often the problem lies in insufficient arterial-venous circulation in the pelvic area. Dopplerography of the vessels of the penis makes it possible to determine the state of blood flow and the causes of erectile dysfunction.
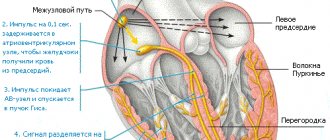
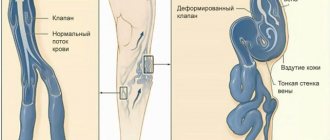
An erection is achieved by filling special anatomical structures of the penis with arterial blood—the corpora cavernosa. Thanks to the high speed of arterial blood flow and low speed of venous outflow, an erection is ensured. As a result of an impaired rate of blood return through the veins or insufficient blood circulation in the penis, sexual function decreases. Doppler ultrasound is designed to put an end to the issue of the origin of erectile dysfunction.
Indications for the study
Erectile dysfunction is one of the indications for Dopplerography of the vessels of the penis. Erectile dysfunction of any origin.
- congenital and acquired injuries and deformations of the penis. Curvature and the like;
- voluminous neoplasms of the penis. Tumors can directly affect the nature of vascularization of the “genital organ”. In addition, the degree of blood supply to the neoplastic structure itself is determined. This is important for identifying the type of tumor process.
During the study, the following changes can be detected in the penis and its structures:
- disturbances in the blood supply to the cavernous bodies with arterial blood;
- change in the speed of venous outflow;
- compression of the vascular structures of the penis;
- narrowing of the veins and arteries of the penis;
- decreased elasticity of veins and arteries;
- the presence of foreign bodies and cicatricial changes in the structure of the urethral canal;
- atherosclerosis of the penis, fibrosis of anatomical structures.
What is examined during ultrasound examination of the vessels of the penis
During an ultrasound scan, the doctor examines the cavernous arteries, blood vessels, as well as the speed of blood inflow and outflow. Indicators must be compared with standards.
Deviations from the norms of ultrasound indicators:
- Echogenicity – decreased may indicate the development of acute cavernitis; increased echogenicity is observed in patients with cavernous fibrosis.
- The structure of the cavernous bodies must be homogeneous. Heterogeneity is characteristic of focal cavernous fibrosis.
- The tunica albuginea of the organ - thickening of the tissue indicates the development of Peyronie's disease.
- echogenicity of the walls of the cavernous arteries is usually observed in patients with diabetic vascular disease.
The diameter of the cavernous arteries is normal 0.2-1.4 mm. Narrowing of the lumen is a sign of autoimmune or atherosclerotic pathology. Diameter expansion is inherent in vascular development anomalies.
Ultrasound diagnostics is carried out so that the doctor can accurately determine the type of vascular disorder of the penis and select effective therapy.
Preparing for the study
Immediately before performing the manipulation, it is recommended to carry out thorough hygiene of the penis and groin area.
- in addition, half an hour before the start of the procedure, it is necessary that the bladder is partially filled. If the organ is empty, the results may be blurry and inaccurate;
- A few days before Dopplerography, you should give up alcoholic beverages, especially beer, and smoking, so as not to cause a secondary change in the blood flow of the vessels of the penis. Otherwise, the survey results will be false.
Research in recent years has changed not only the view of the mechanism of erection development, but also the etiology of erectile disorders. If previously the dominant point of view was on erectile dysfunction (ED) as a psychogenic disease, now most experts place organic factors in first place among its causes, although mental influences often aggravate it. According to various authors, from 70 to 85% of all cases of ED are associated primarily with organic causes. O. L. Tiktinsky and V.V. Mikhailichenko believe that 70% of ED are of vasculogenic nature (30% of them are of arterial origin, 30% of venous origin, 40% of mixed origin) [1]. N.A. Lopatkin also does not agree with the consideration of psychogenic factors as the main cause of erectile disorders. In his opinion, 70-85% of cases of erectile disorders are primarily associated with organic causes, that is, caused by vasculogenic, endocrine, neuroendocrine factors [2].
The most common pathogenetic factor of ED is vascular damage, and this damage is always systemic in nature. Therefore, identifying the vascular origin of ED may be the reason for a comprehensive examination of the patient’s cardiovascular system. Conversely, a patient who complains of erectile dysfunction and has risk factors for cardiovascular diseases (abdominal obesity, diabetes mellitus, high blood pressure) has a greater risk of arteriogenic ED.
One of the most authoritative experts on this problem is Professor P. Montorsi from the University of Milan. In 2005, he called ED “the tip of the iceberg” of systemic vascular diseases and pointed out that isolated ED is a reason for further examination of the patient, especially the state of his cardiovascular system [3].
Professor R. Montorsi et al. showed that in patients with angiographically proven obstructive ischemic heart disease, the onset of ED preceded the onset of symptoms of this disease. The time interval was 38.8 months (range 1–168 months), with ED determined by questionnaire only. One of the most important facts established during this study is that in 40% of patients, coronary heart disease debuted with acute myocardial infarction [4].
According to other data, the time from the onset of ED to the appearance of the first symptoms of coronary heart disease is 24 (12-36) months [5].
While the risk of cardiovascular disease mortality was higher in men with an established diagnosis of cardiovascular disease (CVD) before ED diagnosis, the average time interval between the onset of ED and cardiovascular death was 10 years in the 40-69 age group . Despite the statistically significant increase in the risk of death with an established diagnosis of CVD, the study showed that only 35% of all deaths in men with ED were etiologically related to these diseases, while 65% were not related to them (mortality from cancer amounted to 29%) [6].
A large cohort study of the incidence of adverse cardiovascular events in patients with ED showed that although ED increases the risk of future such vascular events, it is not an age-independent predictor of their development, unlike arterial hypertension and diabetes mellitus [ 7]. However, a limitation of this study is that ED was determined only using the International Index of Erectile Function (IIEF) questionnaire.
However, data on the relationship between ED and CVD are sometimes very contradictory. Thus, when comparing two groups of patients at high risk of cardiovascular diseases with and without ED for the presence of clinically significant damage to the coronary arteries, it turned out that in patients with erectile dysfunction, clinically significant damage to the coronary arteries occurred in 87% of cases, and in patients with normal erection in 82% (p=0.552). In addition, no statistically significant differences were found when analyzing individual coronary artery lesions or their number with the presence of ED (52.5% of cases of multivessel disease in the ED group compared with 34.2% in the control group, p = 0.076) [8].
According to the results of an autopsy study of patients, coronary atherosclerosis was found in 87.1% of patients, while atherosclerosis of the penile vessels was found in only 12.9%, and damage to the deep penile artery was found in 9.7%. In this study, diabetes mellitus was the only factor that was associated with atherosclerosis of the arteries supplying blood to the penis. This allows us to think about how strongly ED is ultimately associated with damage to the coronary arteries [9].
In addition, almost all published studies on this topic determined the presence of ED in patients only using questionnaires (most often IIEF-5). Although the sensitivity is sufficiently high, questionnaires have low specificity. For this reason, patients with psychogenic, endocrine, and neurogenic ED were included in the studies. Due to conflicting literature data, there was a need to study the state of penile hemodynamics in patients with CVD risk factors using instrumental methods for studying penile blood flow as a criterion for arteriogenic ED.
Today, the main method for determining vascular disorders in patients with ED is Dopplerography of the vessels of the penis. For the first time, a method for assessing arterial blood supply, including in the vessels of the penis, based on the use of the Doppler effect, began to be used in 1975. The method of artificial pharmacological erection proposed in 1982 by R. Virag significantly improved the quality of functional studies of penile blood flow [10]. Currently, pharmacological artificial erection using vasoactive agents such as papaverine, phentolamine, prostaglandins E1 and their various combinations is widely used in clinical practice as a screening test, allowing one to differentiate psychogenic and organic forms of erectile disorders with some certainty [11].
Pulse Dopplerography and spectral analysis in the study of erectile function were proposed in 1980 and were reflected in the works of A. Cliffird et al. and D. Velcek et al. [12, 13]. Since 1984, the technique of high-frequency sonography in combination with quantitative analysis of the Doppler spectrum, described in the works of TF Lue et al., has become widespread. [14].
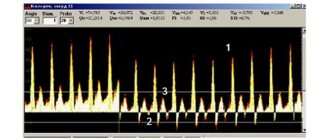
The main quantitative indicators of Doppler ultrasound are maximum (peak) systolic velocity (PSV or Vmax) and end-diastolic velocity (EDV or Vend). Based on absolute indicators, relative indicators are calculated using standard formulas - resistance index (RI) and pulsation index (PI). Usually, values equal to 25 cm/s are taken as the norm for maximum systolic velocity [18]. After pharmacological stimulation, the highest value for a given patient is usually achieved within 5-10 minutes.
Analysis of the nature, severity and duration of pharmacological erection and parameters recorded by ultrasound Doppler scanning, often when performing a study, allows not only to record the fact of vascular disorders, thereby differentiating psychogenic and organic ED, but also to distinguish arterial insufficiency of the penis from venogenic [19 ].
MATERIALS AND METHODS
The study included adult men with complaints of erectile dysfunction. A total of 481 men aged 18 to 75 years were included in the study. The mean age was 40.2±12.8 years (95% CI: 39.1-41.4 years).
All patients underwent a comprehensive study of erectile function, which included: examination by a urologist, a standardized survey using questionnaires IIEF, Ageing male scale - (AMS), biochemical blood test, blood test for testosterone, Dopplerography of penile vessels with a pharmacological test , Rigi-scan real-time monitoring of penile tumescences, as well as assessment of systemic endothelial function by post-occlusion measurement of peripheral arterial tone.
Statistical analysis of the obtained data was carried out after retrospectively dividing the study population into groups of high and low CVD risk. The presence of at least one of the following conditions was taken as a high-risk criterion:
- Abdominal obesity;
- Arterial hypertension;
- History of diabetes mellitus type 1 or 2;
- Age over 40 years.
Also, studies were conducted on the correlation between hemodynamic parameters of the penis and anthropometric indicators in the general group.
DESCRIPTION OF THE METHOD OF PHARMACODOPPLEROGRAPHY OF THE VESSELS OF THE PENIS
Duplex and triplex Doppler scanning of penile vessels was performed on an Accuson-128, Siemens 270 A device. 7.5 MHz, 8 MHz, 10 MHz sensors were used.
As the drugs of choice for creating a pharmacological erection, optimally suitable for intracavernous administration for diagnostic purposes, we used drugs from the E1 prostaglandin group (Caverject, Edex). The dose of the drug was 10 mcg. Doppler ultrasound, first of all, assessed the speed and nature of blood flow in the penile arteries, as well as the nature of changes in blood flow after the introduction of pharmacological erection stimulants.
With the patient in a horizontal position, sequential bilateral locating of the dorsal and deep penile arteries was performed. The scanning angle ranged from 45 to 60º. To locate the dorsal arteries, the sensor was installed on the dorsal surface of the penis lateral to the midline at the base of the penis and in the area of the coronary sulcus. When locating the cavernous arteries, the sensor was installed lateral to the spongy body of the urethra.
Dopplerographic parameters were recorded bilaterally throughout the entire vessel segment by segment. The study of the arterial phase began with the tumescence phase (ER1 - ER2-3) - the phase of increased arterial inflow to the penis and continued throughout the entire cycle of erection development until the rigid phase (ER4, ER5).
The quality of the pharmacological response was assessed using a six-point Junemann scale using graphical analysis. The use of this scale is pathogenetically justified, since it reflects in more detail the phases of erection development.
Junemann scale
- ER0 – no response;
- ER1 – slight tumescence (increase in the length of the penis);
- ER2 – incomplete tumescence (increase in the diameter of the penis);
- ER3 – complete tumescence (increase in diameter at the maximum possible length is not sufficient for full coitus);
- ER4 – semi-rigid state of the penis;
- ER5 – full erection.
Starting from degree ER4, intromission and coitus are possible.
Doppler ultrasound can show the following:
- hemodynamics in the penis at rest;
- the presence of a deficiency of arterial blood flow to the corpora cavernosa during the occurrence of an erection;
- the presence of pathological venous drainage.
Throughout the study, qualitative and quantitative (absolute and relative) parameters were assessed. Of the absolute quantitative values, peak systolic velocity, end-diastolic velocity, and average blood flow velocity were used. Among the relative ones, there are the resistance index (RI) and the pulsatility index (PI), calculated according to generally accepted formulas: RI = (Vmax – Vend)/Vmax, where Vmax is the maximum systolic blood flow velocity, Vend is the final diastolic blood flow velocity. РI = (Vmax – Vmin)/Vmean, where Vmax is the maximum blood flow speed, Vmin is the minimum blood flow speed, Vmean is the average blood flow speed (time-averaged maximum speed).
The Doppler spectrum of the penile artery is normally characterized by:
- Gradient of increase in maximum systolic blood flow velocity by two or more times for dorsal arteries;
- The gradient of the increase in maximum systolic blood flow velocity is three or more times for the deep penile arteries;
- Lack of diastolic blood flow in the relaxed phase;
- High-frequency diastolic blood flow in the tumescence phase with regression during the development of a semi-rigid state;
- Phase changes in Doppler parameters during the transition of the penis from a relaxed state to an erect state;
- Dynamic change in the resistance index with maximum values equal to one in the relaxation phase and in the phase of full erection.
Determination of Dopplerographic indicators of blood flow in the penis was also carried out after intracavernous administration of a vasoactive drug. The main symptom of arteriogenic ED was a decrease in peak systolic velocity of less than 25 cm/s. The maximum value of peak systolic velocity was assessed, which is not always recorded in the first 5-10 minutes of the study. Venogenic disorders are characterized by an end-diastolic velocity of more than 5 cm/s with adequate arterial inflow, a resistance index of less than 0.85; pulsation index less than 3.
RESULTS AND DISCUSSION
In domestic and foreign literature, the IIEF-5 scale is most often used to determine the presence and severity of ED, so it was extremely important for us to find out whether the IIEF-5 scale allows us to judge the nature of blood flow in the vessels of the penis. When analyzing the entire study population, it turned out that the maximum systolic blood flow velocity in the cavernous arteries does not correlate with the severity of ED, determined by the IIEF-5 scale (Fig. 1). Thus, the widely used IIEF-5 questionnaire does not allow determining the nature of erectile dysfunction and the severity of vascular damage.
Rice. 1. Correlation between the IIEF-5 score and Vmax in the cavernous arteries according to Doppler ultrasound.
As one of the diagnostic criteria that allows us to assume the organic nature of ED already at the stage of collecting complaints, the duration of the history of erectile disorders is used. When comparing hemodynamic characteristics with the duration of ED, we identified a tendency towards a decrease in peak systolic blood flow velocity in the penile arteries with increasing duration of ED (r = -0.068) (Fig. 2). Our study revealed that as the duration of ED increases, the number of scores on the IIEF-5 scale actually decreases, but this does not increase the likelihood of vascular origin of ED.
When analyzing the dependence of penile hemodynamics on the severity of individual risk factors for cardiovascular diseases, a statistically significant correlation was revealed between abdominal circumference and peak systolic blood flow velocity (r=-0.22, p
Rice. 2. Correlation between the duration of ED (in months) and Vmax in the cavernous arteries according to Doppler ultrasound data
Rice. 3. Correlation between abdominal circumference (in cm) and Vmax in the cavernous arteries in the study population according to Doppler ultrasound data
269 people were included in the group of patients at high risk of cardiovascular diseases. When comparing the severity of ED on the IIEF-5 scale and Doppler characteristics of penile blood flow, a statistically significant difference was revealed only in Vmax values (Fig. 4–6).
It turned out that in the group of patients with a high risk of cardiovascular diseases, the severity of ED, assessed using the IIEF questionnaire, practically does not allow predicting the severity of blood flow disorders in the vessels of the penis (Fig. 7).
Rice. 4. Comparison of IIEF-5 scores in patients at low and high risk of cardiovascular disease
Rice. 5. Comparison of Vmax in the penile arteries in patients with low and high risk of cardiovascular disease
Rice. 6. Comparison of Vend in penile arteries in patients at low and high risk of cardiovascular disease
Rice. 7. Correlation between IIEF-5 scores and Vmax in the cavernous arteries in a group of patients at high risk of cardiovascular disease
The history of cardiovascular diseases in a number of observations also did not allow us to confidently assume the arteriogenic nature of erectile dysfunction. Thus, in patients with a previously established diagnosis of arterial hypertension, there are no significant differences in the nature of blood flow in the cavernous arteries compared to patients with normal blood pressure (Fig. 8).
Rice. 8. Comparison of Vmax in the cavernous arteries with the risk of cardiovascular diseases in patients with normal blood pressure and with a history of arterial hypertension.
A history of diabetes mellitus, on the contrary, is an independent risk factor for deterioration of inflow through the arteries supplying blood to the corpora cavernosa of the penis (Fig. 9).
Rice. 9. Comparison of Vmax in the penile arteries in patients with and without diabetes mellitus (p=0.022)
There is also a tendency for Vend to decrease in the penile arteries in men with diabetes mellitus compared to men with normal carbohydrate metabolism (Fig. 10) (p = 0.067).
Peak systolic blood flow velocity was not statistically different between men with normal testosterone levels and men with low testosterone levels (Fig. 11).
Rice. 10. Comparison of Vend in penile arteries in patients with and without diabetes mellitus (p=0.067)
Rice. 11. Comparison of Vmax in the penile arteries in patients with normal and low testosterone levels (p = 0.25)
Some sources [21 – 23] claim that veno-occlusive ED may be associated with a decrease in testosterone levels. The results of our study showed that Vmax in the deep dorsal veins in patients with normal and low testosterone levels does not differ (Fig. 12)
Rice. 12. Comparison of Vmax in the deep dorsal veins in patients with normal and low testosterone levels (p = 0.82)
Despite the fact that today, unfortunately, there are difficulties in standardization in the interpretation of Dopplerographic indicators, which are associated with different resolutions of ultrasound devices, methodological features, the choice of parameters being studied, as well as with psychogenic depression in patients with a labile nervous system, Doppler ultrasound of blood vessels penis is the main method for determining blood flow in the arteries of the penis, which ensures the occurrence and maintenance of an erection. The uniqueness of the Doppler ultrasound technique is that often in the course of one study it is possible to carry out not only topical diagnostics, but also differential diagnostics of the condition of the vascular system of the penis.
CONCLUSION
In most cases, vascular lesions in the human body are systemic in nature, so it seems logical that in patients with a history of cardiovascular disease or relevant risk factors, disturbances in penile hemodynamics (in particular, arterial inflow) will be very pronounced. However, the results of our research show that this is not always the case.
Some CVD risk factors, such as obesity, do correlate with impaired penile hemodynamics. Abdominal obesity is an independent risk factor for cardiovascular and endocrine diseases, as well as arteriogenic ED. Excessive fat deposits on the anterior abdominal wall leads to a decrease in testosterone levels, and as a result, problems with erection.
Among the studied diseases characterized by vascular damage, only diabetes mellitus turned out to be a statistically significant predictor of decreased arterial inflow through the cavernous arteries.
LITERATURE
1. Tiktinsky O.L., Mikhailichenko V.V. Andrology. 1999. pp. 109–223.
2. Impotence // Guide to urology. [Ed. Lopatkina N.A.] M.: Medicine, 1998. T. 3. P. 602-621.
3. Montorsi P, Montorsi F, Schulman CC. Is erectile dysfunction the “type of the iceberg” of a systemic vascular disorder? // Eur Urol, 2003. Vol 44, N 3. P. 352-354.
4. Montorsi F, Briganti A, Salonia A, Rigatti P, Margonato A, Macchi A, Galli S, Ravagnani PM, Montorsi P. Erectile dysfunction prevalence, time of onset and association with risk factors in 300 consecutive patients with acute chest pain and angiographically documented coronary artery disease. // Eur Urol. 2003. Vol. 44, N 3. P. 360–365
5. Montorsi P, Ravagnani PM, Galli S, Rotatori F, Veglia F, Briganti A, Salonia A, Dehò F, Rigatti P, Montorsi F, Fiorentini C. Association between erectile dysfunction and coronary artery disease. Role of coronary clinical presentation and extent of coronary vessels involvement: the COBRA trial. // Eur Heart J. 2006. Vol. 27, N 22. P. 2632-2639.
6. Chew KK, Gibson N, Sanfilippo F, Stuckey B, Bremner A. Cardiovascular mortality in men with erectile dysfunction: increased risk but not inevitable. // J Sex Med. 2011. Vol. 8, N 6. P. 1761-1771.
7. Ponholzer A, Gutjahr G, Temml C, Madersbacher S. Is erectile dysfunction a predictor of cardiovascular events or stroke? A prospective study using a validated questionnaire. // Int J ImpotRes. 2010. Vol.22, N 1. P. 25-29, 2010.
8. Garcia-Cruz E, Bonet A, Asiain I, Luque P, Freixa R, Alcaraz A. Relationship between erectile dysfunction and coronary anatomy in patients with ischemic heart disease debut. // Eur Urol Suppl. 2013. Vol. 12, N 1. P. 208.
9. Ponholzer A, Stopfer J, Bayer G, Susani M, Steinbacher F, Herbst F, Schramek P, Madersbacher S, Maresch J. Is Penile Atherosclerosis the Link Between Erectile Dysfunction and Cardiovascular Risk? An Autopsy Study. // Int J Impot Res. 2012. Vol. 24, N 4. P. 137-140.
10. Virag R.. Intracavernous injections for erectile failure. // Lancet, 1982. Vol. 320, N 8304. P. 938.
11. Kovalev V.A. Diagnosis and treatment of erectile dysfunction: abstract. diss. ... dr. honey. Sci. M. 2001. 37 p.
12. Clifford A, Toppo JN. Role of penile color doppler in the evaluation of erectile dysfunction. // Indian J Radiol Image. 2006. Vol.16. P..891-896
13. Velcek D, Sniderman KW, Vaughan ED Jr, Sos TA, Muecke EC. Penile flow index utilizing a Doppler pulse wave analysis to identify penile vascular insufficiency // J Urol. 1980. Vol. 123, N 5. P. 669-673.
14. Lue TF, Hricak H, Marich KW, Tanagho EA Vasculogenic impotence evaluated by high-resolution ultrasonography and pulsed Doppler spectrum analysis. // Radiology. 1985. Vol. 155, N 3. P. 777-781.
15. Koroleva S.V. Dopplerography of the penis in the diagnosis of erectile dysfunction: Abstract. diss. ...cand. medical sciences M., 1997. 29 p.;
16. Kogan M.I., Krupin V.N., Shakhov B.E. Arterial factors in the mechanism of penile erection. // Urology and nephrology. 1995. N 2. P. 37–41.;
17. Montorsi F, Guazzoni G, Barbieri L, Galli L, Rigatti P, Pizzini G, Miani A. The effect of intracorporeal injection plus genital and audiovisual sexual stimulation versus second injection on penile color Doppler sonography parameters. // J Urol. 1996. Vol. 155, N 2. P. 536-540.
18. Wilkins CJ, Sriprasad S, Sidhu PS. Color Doppler ultrasound of the penis. // Clin Radiol. 2003. Vol. 58, N 7. P. 514-523
19. McMahon CG. Correlation of penile duplex ultrasonography, PBI, DICC and angiography in the diagnosis of impotence. // Int J Impot Res. 1998. Vol. 10, N 3. P. 153-158.
20. Porst H. Manual der Impotenz. UNI-MED Verlag AG, 2000. 544 p.
21. Traish AM, Guay AT. Are androgens critical for penile erections in humans? Examining the clinical and preclinical evidence. // J Sex Med. 2006. Vol. 3, N 3. P. 382–404.
22. Traish AM, Goldstein I, Kim NN. Testosterone and erectile function: from basic research to a new clinical paradigm for managing men with androgen insufficiency and erectile dysfunction. // Eur Urol. 2007. Vol. 52, N 1. P. 54–70.
23. Rogers RS, Graziottin TM, Lin CM, Kan YW, Lue T. Intracavernosal vascular endothelial growth factor (VEGF) injection and adeno-associated virus-mediated VEGF gene therapy prevent and reverse venogenic erectile dysfunction in rats. // Int J Impot Res. 2003. Vol. 15, N 1. P. 26–37.
| Attached file | Size |
| 538.28 kb |
‹ Bacterial urinary tract infections in patients after kidney transplantation Up Deferentitis and funiculitis: classification, clinical picture and diagnosis (literature review) ›
Description of the study
The patient undresses, takes off his underwear and lies down on the couch. The doctor lubricates the penis area with a special gel and applies an ultrasound sensor. By its nature, Doppler ultrasound is a variation of vascular ultrasound. After a thorough examination of the non-erect penis, a special drug is injected into the corpora cavernosa to cause a spontaneous erection. Unlike a normal erection, an induced erection does not begin as quickly and develops over a longer time, thanks to which the diagnostic specialist can track the nature and intensity of blood flow in each phase. The duration of the study is 30-40 minutes. Measurements are taken every 3-5 minutes, after which the doctor records the results in a protocol.
Instead of injecting the drug into the organ area, it is possible to take Viagra and its analogues. The use of sedative pharmaceuticals is not recommended, since there is a high risk of stopping potency. Depending on the clinic, other methods of stimulation are also possible, for example manual stimulation, viewing pornographic materials. However, these methods do not give a reliable result: natural erection is unstable and develops rapidly, so there is no way to study each of its phases. In addition, the procedure lasts 30-60 minutes, it is impossible to maintain potency for such a long time naturally. The results are given to the patient 20-30 minutes later, upon completion of the examination. As a result of the manipulation, the following diseases and pathological conditions can be identified:
- injuries of vascular structures (venous and arterial);
- thrombosis of the great vessels of the penis;
- cavernous fibrosis;
- neoplastic processes in the penis;
- atherosclerosis of the vessels of the penis (as a result of occlusion or stenosis);
- Peyronie's disease (curvature of the penis).
Treatment methods
The disease is treated conservatively or surgically.
If pathology is identified at the initial stage, it is quite possible to get by only with medication and auxiliary procedures. The use of vitamins and a mixture of fatty acids is prescribed. Diet and wearing loose underwear are recommended. If the condition is complicated by prostatitis, anti-inflammatory medications are prescribed.
The operation is a necessary measure aimed at restoring blood supply to the penis to prevent its atrophy. Bypass surgery has the main indication – blocking the lumen of a blood vessel by more than 70%.
High-quality treatment in our clinic will prevent the development of atherosclerosis of the penis and the consequences of pathology. Doctors have informative diagnostic equipment at their disposal. Thanks to him, it is possible to identify a violation even at the initial stage of its development. The operating rooms are equipped with high-quality equipment, which allows the intervention to be performed without subsequent complications.
Criteria for assessing survey results
- echogenic indicators of penile tissue and vascular structures of the organ;
- features of blood flow in the deep-lying and external areas of the penis;
- blood circulation speed, features of venous valves.
- systolic velocity of arterial blood supply is within 30-50 centimeters per second. A lower figure indicates insufficient filling of the corpora cavernosa with blood and, therefore, an erection either does not occur at all or is excessively weak;
- diastolic velocity of arterial blood flow, which is approximately 5 centimeters per second. Ideally, it is desirable that the indicated indicator be in the region of zero;
- pulsation index within approximately 4 and no more;
- resistance index. Indicators below 0.85 indicate erectile dysfunction.
Additionally, the speed of venous outflow is determined. If the levels are excessive, the erection is unstable. In general, the doctor deciphers the results. It's almost impossible to figure it out on your own. Dopplerography of the vessels of the penis is an indispensable study, for which there are no alternatives. It makes it possible to assess the nature and speed of blood flow and identify the causes of erectile dysfunction. After the manipulation, you should consult a doctor for decoding. All questions should be directed to your healthcare professional. Trying to understand the nature of the process on your own is a waste of time and effort.
How is ultrasound examination of the vessels of the penis performed?
During the diagnosis, the patient should lie on his back. A conductor gel is applied to the penis; it improves contact of the sensor with the skin. Moving across the skin, the equipment reads data about the structure of the penis and the condition of its arteries. The research results are visualized on the screen.
During the procedure, the doctor can introduce a pharmacological drug (like Vasoprostan or Caverject) through a special tourniquet, which will help cause an erection. If the patient is able to achieve an aroused state of the genital organ in a natural way (viewing magazines or videos of an erotic nature, manual stimulation), then the injection is not given.
In the erect state, signs of deformation of the penis, the level of filling of the cavernous bodies and the strength of blood flow are checked. After the doctor conducts Doppler mapping, the patient can use self-stimulation to get rid of the pharmacological effect; for this, he is left alone in the office. The results of scanning the blood vessels of the penis are given to the patient immediately, and he must go with them to his attending physician.
Service cost*
| NAME | PRICE (Kolomenskaya) | PRICE (Vidnoe) |
| Duplex scanning of the vessels of the scrotum and penis (on the device Voluson, Mindray, Logiq) | 2900 rubles | 2900 rubles |
We accept payment:
*Attention! The indicated prices are provided as reference information and do not constitute a public offer. Check current prices by phone and directly in clinics.
Prevention
To prevent erection problems, it is useful for men to heed the following advice:
- Learn to eat healthy, eliminating unhealthy foods (smoked, canned, salted, alcohol) from your diet. Fruits, vegetables, dairy products, herbs, nuts, and honey should take priority place on the table.
- Say goodbye to unhealthy habits (smoking, alcohol abuse, drugs, sedentary lifestyle).
- Have a regular sex life. Full, uninterrupted intercourse with a regular partner will eliminate many of the problems leading to ED.
- Do not neglect regular visits to the urologist's office. High-level specialists work at the Global Clinic Center; timely consultation will relieve men from problems with erection.
- Monitor your general health.
Symptoms
The presence of erectile dysfunction is indicated by a weakening of the ability to perform full sexual intercourse. This happens in cases where:
- the penis is not hard enough for coitus;
- erection weakens during sexual intercourse;
- it takes a long time for an erection to occur;
- change in sensations during orgasm.
The man does not immediately understand that these changes are associated with the appearance of erectile dysfunction, attributing this phenomenon to fatigue, stress, and general malaise. The roots of the problem may be much deeper. Only qualified doctors, such as those at the Global Clinic Center, can prescribe the correct course of treatment to eliminate this pathology.
DESCRIPTION OF THE INFORMATION WE COLLECT AND HOW WE USE IT
1. General information
Like many commercial organizations, we monitor use of this site by collecting aggregate information through cookies (see below). As a rule, we keep statistics on the number of visits to the site, each web page and register the name of the original domain of the Internet service provider whose services the visitor uses. The information obtained allows us to make conclusions about the use of the site by the visitor, and may also be transferred to other companies of the Group and other third parties.
2. Personal information
When you register as a user on our website or fill out an online form (for example, to receive email updates), we collect personal information about you, such as your first and last name, email address, country of residence, and other information you provide voluntarily.
We are committed to improving the content and functionality of our site. Therefore, through cookies (and other similar technologies) we collect information about your use of this site (see below). We may also monitor navigation and use of the site in order to improve its design and structure, taking into account user preferences by tailoring content. By doing this, we strive to make the site more user-friendly. We may also conduct statistical analyzes of our user accounts to determine the proportion of active users, the frequency of their visits, and the number of other sites they are registered with.
In some cases, we may receive information about your opinions, for example when you send us feedback or ask questions, as well as information about you from other publicly available sources, which we will supplement with information we already have in order to improve the service to suit your specific requirements. user.
If you provide information about another person, such as your colleague, you confirm that you are acting on the instructions of such person and provide his consent to the processing of his personal information, including important personal information, and also confirm that you have provided such person with information about us and about the purposes (in accordance with this Privacy Policy) for which personal information will be used.
We may provide personal information upon request to comply with legal requirements.
You consent to our transfer of information to countries or jurisdictions that do not provide legal protection for data protection to the same extent as your country. When we make such a transfer, we are committed to ensuring that your information is adequately protected.
All personal data provided to AstraZeneca Pharmaceuticals LLC, as well as companies included in the group (including those entered on the website), can be used and processed, in addition to the above, also for the purposes of:
• providing scientific medical and any other information about AstraZeneca products, as well as materials in written, printed, electronic, audio, video, oral and any other appropriate form, via email, regular and courier mail, telephone calls, SMS messages , messages on social networks on the Internet, in person and/or in any other appropriate way;
• invitations to scientific, educational and other events aimed at improving the professional level of relevant specialists, in all the above ways and in all the above forms;
• creating a database of persons who provided their personal data.
The person who voluntarily provided his personal data and information is notified and consents to the processing by AstraZeneca Pharmaceuticals Limited Liability Company, all other companies included in the group, as well as any third parties to whom AstraZeneca Pharmaceuticals LLC transfers the relevant personal data for the purposes specified above, and subject to the obligatory condition that these persons ensure the security of the personal data provided above, including collection, recording, systematization, accumulation, storage, clarification (updating, changing), extraction, use, transfer (distribution, provision, access, including cross-border transfer), depersonalization, blocking, deletion, destruction with or without the use of automation tools. Also, the Person who voluntarily provided his personal data and information is notified and agrees that during the cross-border transfer of his personal data, recipients of such data may be located in foreign countries that do not provide adequate protection of the rights of personal data subjects. Operators, at the same time, undertake to take all reasonable and appropriate actions to ensure the confidentiality and security of any Personal Data transferred to the territory of any foreign countries.
This consent to the processing of personal data is given for an indefinite period and can be withdrawn by sending a written application to the site administration. I hereby acknowledge and confirm that I have read and agree with the rights and obligations in accordance with the Federal Law of the Russian Federation of July 27, 2006 No. 152-FZ “On Personal Data,” including the procedure for revoking consent to the processing of personal data.
Filling out the form for providing Personal Information implies agreement that any personal data provided by filling out this form can be used, taking into account the consent provided, in accordance with the requirements of the Federal Law of the Russian Federation of July 27, 2006. No. 152-FZ “On Personal Data” and stored for ten years at (125284, Moscow, Begovaya St., 3, building 1) for registration and response to this request for scientific medical information.
What is erectile dysfunction
Harmony in sexual relationships among men of any age is an important part of a fulfilling life. Erectile dysfunction is an unpleasant moment that will plunge representatives of the stronger sex into despondency and deprive them of sleep. The statistics are relentless and indicate that the problem of erectile dysfunction has become much younger. Previously, it was mainly men of forty years of age and older who faced the lack of penile erection, but in the modern world, the presence of similar problems is diagnosed in young people. The causes and treatment of “male” dysfunction concern men of different ages. When blood circulation in the penis is impaired, a pathology called erectile dysfunction (ED) occurs. In this case, not only does sexual intercourse become difficult, but the possibility of conceiving a child is often excluded. Lack of erection is often confused with impotence. The presence of erectile dysfunction covers smaller problems than impotence, characterized by decreased libido and the inability to fertilize a woman's egg.