- Gallery
- Reviews
- Articles
- Licenses
- Vacancies
- Insurance partners
- Partners
- Controlling organizations
- Schedule for receiving citizens for personal requests
- Online consultation with a doctor
- Documentation
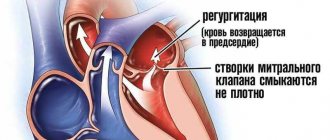
Minor anomalies of cardiac development (MACD) in children are minor changes in the structure of the heart and blood vessels, which, as a rule, do not lead to gross disturbances of blood flow and do not cause significant clinical manifestations.
The abbreviation MARS is consonant with the name of the planet, which makes it easier to remember the long, complex term.
In recent years, there has been an increase in the number of children with minor anomalies of cardiac development. This is primarily due to improved diagnostics due to the widespread introduction into practice of ultrasound examination of the heart (cardiac ultrasound or EchoCG - echocardiography).
A minor anomaly of cardiac development is manifested by symptoms of autonomic dysfunction:
- pain in the heart area;
- emotional lability;
- fatigue;
- signs of astheno-neurotic syndrome;
- a characteristic heart murmur is heard.
Their manifestations can become more pronounced as the child grows, leading to various complications, for example, heart rhythm disturbances and the formation of additional pathways in the heart. This leads to poor exercise tolerance and a tendency to faint. Such children are at risk for developing infective endocarditis - complications after acute respiratory infections and tonsillitis in the form of an inflammatory process of heart tissue.
Prevention of the development of complications is a timely visit to a doctor in cases of the appearance of the listed complaints and the implementation of prescribed diagnostic measures.
Children are prescribed an ECG (to determine possible arrhythmias) and echocardiography (ultrasound of the heart). This method allows you to visualize the heart and large vessels, clarify the presence of cardiac abnormalities and determine whether there are disturbances in its functioning.
Make an appointment with a pediatric cardiologist and examination by phone +7(495)150-60-03
Services and prices
Primary appointment (examination, consultation) with a pediatric cardiologist
2,200 rub.
Repeated appointment (examination, consultation) with a pediatric cardiologist
2,100 rub.
Electrocardiogram at rest
600 rub.
Electrocardiogram with functional tests
1,000 rub.
Echocardiography with Doppler analysis (in PW, CW mode) and color two-dimensional Doppler mapping for children under one year old
RUB 3,800
Echocardiography with Doppler analysis (in PW, CW mode) and color two-dimensional Doppler mapping for children from 1 year to 7 years
3,700 rub.
Echocardiography with Doppler analysis (in PW, CW mode) and color two-dimensional Doppler mapping for children over 7 years old
3,600 rub.
Publications in the media
Minor anomalies of cardiac development (MADC) are anatomical congenital changes in the heart and great vessels that do not lead to gross dysfunction of the cardiovascular system. A number of MARS are unstable and disappear with age. Frequency - 2.2-10% in the population, in children with various cardiac pathologies - 10-25%, increases with hereditary connective tissue diseases. The predominant age is children of the first 3 years of life. Etiology. Hereditary determined connective tissue dysplasia. A number of MARS are dysembryogenetic in nature. The influence of various environmental factors (chemical, physical effects) cannot be excluded.
Options. About 40 variants of MARS are described in the literature. Most often observed • Ectopic trabeculae • Mitral valve prolapse • Tricuspid valve prolapse • Patent foramen ovale • Long Eustachian valve (flap) - a non-rudimentary fold of the endocardium (an element of the embryonic circulation), located at the mouth of the inferior vena cava from the side of the right atrium cavity, with a length of 1 up to 2 cm. Usually accidentally found during echocardiography • Aneurysm of the interatrial septum - protrusion of the interatrial septum in the area of the fossa ovale, which does not cause hemodynamic disturbances. Clinically, upon auscultation - systolic clicks • Aneurysm of the interventricular septum - bulging of the interventricular septum towards the right ventricle. On auscultation - systolic murmur and clicks on the left at the base of the sternum • Dilatation of the aortic root and sinuses of Valsalva - expansion of the aortic orifice (in children, normally 1.2–2.4 cm) and sinuses (normal depth, 1.5–3 mm ). Auscultation - inconsistent systolic “clicks”, sometimes a “spinning top” sound on the vessels of the neck.
Concomitant pathology • Marfan syndrome • Ehlers–Danlos–Rusakov syndrome • Primary hypogonadism • Behcet's syndrome • Congenital heart defects (CHD) • Cardiac arrhythmias • Infective endocarditis • Valvular regurgitation.
Diagnostic criteria • Anamnestic data (occupational hazards, maternal alcoholism during pregnancy, connective tissue diseases in the family, etc.) • Signs of dysplastic development (external minor developmental anomalies - short neck, high palate, etc.) • Characteristic auscultatory pattern depending on the variant of MARS • Changes on the ECG • EchoCG criteria • X-ray criteria.
Differential diagnosis • Congenital heart disease • Major anomalies of cardiac development.
Functional significance • Depends on the patient’s age, variant of MARS, presence of concomitant diseases • Marker of dysembryogenetic development of the heart • Predisposes to the development of arrhythmias, valvular regurgitation, left ventricular dysfunction.
Treatment is determined by the type of MARS and concomitant pathology.
Reduction. MARS - minor anomalies of cardiac development
ICD-10. Q20.9 Congenital anomaly of cardiac chambers and connections, unspecified
Note. Major anomalies of cardiac development are anatomical changes in the heart and great vessels, accompanied by gross dysfunction of the cardiovascular system (for example, mitral valve prolapse with grade III regurgitation).
Minor anomalies of the aorta
A borderline narrow aortic root is the presence of low values of aortic diameter (from the 3rd percentile and below the distribution curve), with the absolute absence of both signs of stenosis (including Dopplerography) and ECG signs of left ventricular hypertrophy or left-sided overload. The incidence among minor cardiac anomalies is 7-10%
Primary EchoCG criteria:
- aortic diameter less than 20 mm
- absence of a significant pressure gradient between the aorta and left ventricle
Borderline wide aortic root - the presence of increased values of aortic diameter (from 90 percentile or more of the distribution curve). The incidence among minor cardiac anomalies is 5.8-9%.
Dilatation of the sinuses of Valsalva - the presence of dilatation of the sinuses from 3 to 7 mm (usually non-coronary, less often right and left). Occurrence in the population is 0.26%, among minor cardiac anomalies - 27.5%
Asymmetry of the aortic valve leaflets - the presence of unevenly developed and located leaflets (detected in the parasternal position along the short axis). Occurrence among MAS - 8.2%
Aortic valve prolapse is a diastolic protrusion towards the left ventricular outflow tract (more than 1 mm from the line of the annulus fibrosus). Occurrence among MAS - 6.6%
Mitral valve prolapse
Among ultrasound methods for diagnosing primary mitral valve prolapse, preference is given to two-dimensional echocardiography, since one-dimensional echocardiography results in a large number of false-positive and false-negative results. With two-dimensional echocardiography, it is necessary to measure the area of the atrioventricular valve and the circumference of the atrioventricular ring, which are significantly larger in children with mitral valve prolapse than in healthy ones. Sometimes it is possible to identify a violation of the architectonics of the valves, elongation, atypical attachment and incorrect distribution of the chords. The end-diastolic diameter of the left ventricle in children with primary mitral valve prolapse is reduced: in one third it corresponds to the 5th and in half to the 25th percentile. The combination of a reduced left ventricular cavity with an increase in the area of the mitral valve contributes to the occurrence of valvular-ventricular disproportion, which is one of the pathogenetic aspects of leaflet prolapse.
Idiopathic dilatation of the pulmonary artery
It is characterized by an expansion of the trunk in the absence of heart disease and pulmonary pathology. Dilatation of the pulmonary artery trunk occurs against the background of hereditarily determined connective tissue pathology, which is confirmed by the simultaneous detection of other markers of connective tissue dysplasia of the heart and the frequent detection of dilation in hereditarily determined syndromes, for example, Marfan syndrome. Auscultation can detect a systolic murmur of moderate intensity at the base of the heart, which decreases with an upright position. With idiopathic dilatation of the pulmonary artery, dynamic observation and examination is necessary.
Microanomalies of the papillary muscles
This anomaly includes changes:
- forms
- quantities
- location
According to the autopsy:
- Two papillary muscles - 65.2%
- Three papillary muscles - 13%
- Four papillary muscles - 4%
- Five papillary muscles - 4.4%
- Six papillary muscles - 4.4%
Tags: abnormal trabecula, Abnormally located trabeculae, heart disease, true chord, false chords, macroanomalies of the heart, minor cardiac anomalies, MAS, Microanomalies of the papillary muscles, LLC, Patent foramen ovale, right atrium, mitral valve prolapse, pulmonary artery dilatation, heart, Chiari network, Chiari network, trabecula, Elongated Eustachian valve
Microanomalies of the right atrium
The Chiari network is a fibrous structure extending from the crest border or tubercle inferiori to the eustachian or basal valve. The frequency among congenital anomalies is 4%.
Prolapse of the pectineal muscles in the cavity of the right atrium - in the form of thin thread-like and mobile structures in the area of the wall of the right atrium or appendage. Frequency among congenital anomalies - 9.7%
Abnormally located trabeculae, false chords
From the history
The first description is by W. Turner (1893) based on autopsy data
The first term is “moderator band” (1893)
The first classification is MCLam et al. (1970), the term “false chordae tendineae”, i.e. false chord
The first description according to echocardiography data in 1981.
Prevalence of abnormally located trabeculae, false chordae
- according to population studies up to 17%
- autopsy data up to 16%
- according to echocardiography 2.3-68%
- in children with manifestations of CTD in 94%
Video 2. Open oval window. A blood flow discharge from left to right is visualized. Jet diameter 4 mm. Epigastric section.
What is a false chord and anomalous trabecula?
The true notochord is a fibrous cord connecting the papillary muscle to the valve.
False chord is a fibromuscular or fibrous cord connecting the papillary muscles to the wall of the left ventricle or to each other.
Normal trabecula is a muscle cord tightly adjacent to the ventricular endocardium.
Abnormal trabecula is a muscular or fibromuscular cord loosely adjacent to the ventricular endocardium.
Violation of the distribution of chords - their predominant attachment to the base of the valve and, to a lesser extent, in the area of the body or free edge (in systole additional echo signals are located in the outflow tract of the left ventricle)
Lengthening of the chords - additional thin, linear echo structures, performing large-amplitude diastolic movements
Ectopic attachment of chords - attachment of the chord from the wall of the left ventricle to the mitral valve leaflet.
False chords
Quantity:
- single
- multiple
Direction:
- transverse
- diagonal
- longitudinal
Level:
- apical
- median
- basal
Eustachian valve
The Eustachian valve (valvula venae cavae inferioris) is located at the level of the anterior arch of the inferior vena cava and, usually after the neonatal period, does not exceed one centimeter in length or is completely rudimentary. The valve is a fold of the endocardium with an average width of 1 cm. In the embryo, the valve directs a stream of blood from the vein to the foramen ovale. After birth, in the absence of communication between the atria, this valve function loses its significance. According to sectional data, the Eustachian valve is found in 86% of children.
In population studies using echocardiography, an unusually long Eustachian valve (more than 1 cm) is detected in 0.20% of the population and is considered a stigma (Fig. 161). According to our data, this small anomaly predisposes to supraventricular arrhythmias, probably reflexively due to irritation of the pacemaker formations of the atrium.
Fig. 161
Enlarged Eustachian valve of the inferior vena cava.
EchoCG criteria.
Two-dimensional echocardiography:
Visualization of a valve-like structure in the right atrium at the junction of the inferior vena cava.
Subvalvular apparatus of atrioventricular valves
The significance of these microanomalies is not fully understood. Typically, these abnormalities in childhood do not cause valvular regurgitation and/or obstruction of blood flow and are manifested only by a functional systolic murmur, sometimes simulating congenital heart disease. Whether microabnormalities of the chordae and papillary muscles predispose to the onset of valve insufficiency in adulthood is not fully understood. These anomalies are likely to predispose to rheumatic and infective endocarditis, as well as mitral valve prolapse in children and, as a consequence, atrioventricular valve insufficiency in adults. The subvalvular apparatus of the left atrioventricular valve has a wide variety of structure (Fig. 158).
Fig. 158
Anomaly in the structure of the papillary muscles: one papillary muscle located in the apical region, the obturator function of the valve is not impaired.
Most often in childhood, impaired distribution of the chords to the anterior or posterior leaflet of the mitral valve occurs.
Disturbed distribution of chords to the anterior (posterior) leaflet of the mitral valve
EchoCG criteria
One-dimensional echocardiography:
- Increased diastolic excursion of the anterior mitral leaflet.
- Additional echoes from tendon formations in the left ventricular outflow tract during systole.
Two-dimensional echocardiography
- On an echocardiogram, tendon echoes from the anterior (posterior) leaflet are predominantly oriented in the center or at the base.
- There are no manifestations of mitral regurgitation (dilatation of the left atrium and ventricle).
Doppler EchoCG
There is no significant pressure gradient between the left atrium and the left ventricle, as well as the left ventricle and the aorta.
Patent foramen ovale (PFO)
Frequency in the population - 15%
The morphological anomaly is an oval window closed by a fold that is not adherent to the septum
EchoCG criteria
Gradual wedge-shaped thinning of the interatrial septum with interruption of the echo signal (as a rule, there is no sharp break as with an atrial septal defect).
A slight left-to-right shunt can be determined by the color circulation (there is a dependence of the discharge on the respiratory phase)
Pressure in the right side of the heart is within normal limits
Open oval window. A discharge of blood flow from left to right is visualized, the diameter of the jet is 4 mm. Epigastric section.