A defibrillator is a device designed to resuscitate and provide emergency assistance to patients. Modern defibrillators can be used even at home, without special education. The principle of operation of a defibrillator is based on the generation of a powerful charge of electric current, which reaches the heart muscle and leads to its contraction. As a result of this effect, heart function is normalized. If you need a medical equipment supplier, give preference to trusted companies. Let's talk about what the rules are for working with a defibrillator.
What does the heart need to beat?
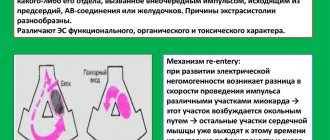
On average, the human heart contracts 60 to 100 times per minute. This occurs due to the work of special stimulating cells in the upper wall of the right atrium (the so-called sinoatrial node). Thanks to them, an electrical differential is created between the outer and inner sides of the cell membrane. At some point, they send an impulse through the entire heart muscle to its lower part, causing the muscle to contract. It would seem that since the heart works from the impulses sent, then what is wrong with electrical stimulation from the outside? To understand this, let's move on.
The electrical differential in the sinoatrial node is created for a reason, but thanks to the presence of electrolytes potassium, sodium and calcium. The electric charge from them passes through the cell walls through special channels (each has its own). An instant before the heart muscle contracts, potassium is contained inside the cells, and calcium and sodium are outside. When sodium enters the cell, it begins to squeeze potassium out, thereby creating an electrical potential. Then channels for calcium open and it also breaks through. This creates the charge necessary for the impulse. Then the impulse from the sinoatrial node goes to the atrium, and then a pulse originates in another node (atrioventricular). Thanks to this complex circuit, blood is pumped from the upper part of the heart to the lower part, and the impulse spreads to other parts of the heart muscle. And only the correct operation of this entire mechanism can create a heartbeat.
If the system fails, different consequences are possible. But we are now interested in the state of fibrillation. This happens if the sinoatrial node does not produce the impulse necessary for the heart. Then the cells of the heart muscle try to create the necessary impulse themselves for some time, but in this case, the contraction of different parts of the heart occurs at odds (fibrillation begins) and the muscle loses its ability to pump blood. It is clear that this cannot continue for long and cardiac arrest soon occurs. But while the muscle is still in a state of fibrillation, there is hope for a defibrillator.
Types of defibrillation
Electrostimulation of the heart is divided into:
- Defibrillation is when an activity is performed to normalize the ventricular rhythm.
- Cardioversion, in which the manipulation is associated with the restoration of atrial rhythm, and all actions are monitored by an ECG.
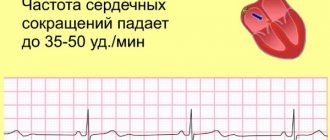
In the first case, the procedure is performed urgently if the ordered heart rhythm is disturbed. The patient is unconscious. Initially, the discharge is 200 joules, later - 360 joules.
Cardioversion can be elective or urgent. This procedure is usually prescribed for a specific period of time, but requires written consent from the patient. During the procedure, the patient is conscious under the influence of sedatives.
What is happening is shown on the monitor and everything is synchronized with the QRS rhythm. Cardioversion voltage is lower than defibrillation and delivers a shock of 50-200 J.
Both methods are performed externally on the chest, doctors use 2 defibrillator electrodes. A third alternative is also possible if the cardioverter-defibrillator is placed inside the chest. It is able to prevent arrhythmia by restoring the function of the generating medium.
When to use a defibrillator
A defibrillator is a device used in medicine to eliminate the condition of fibrillation, that is, uneven, rapid, arrhythmic and unproductive contraction of the heart muscle, atria or ventricles.
The state of fibrillation on the cardiogram will look like a curved line with many small jumps up and down (and not like the smooth straight line from the movies). This graph indicates that different parts of the heart contract at different rates and with their own rhythm. And just the electric discharge gives a chance to restore the correct rhythm of contractions. Exposure to an electric current that is more powerful than the contraction of the heart muscle allows you to even out this process and force different parts of the heart to work in unison again.
The “miracle” of the defibrillator is that the electric current activates the electrolytes and they again begin to flow through the channels in their “schedule”. But that same straight line on heart monitors is asystole. She says that the electrolytes necessary to create an impulse are absent in the cells. The task of doctors is to apply defibrillation before the patient experiences asystole. Later, all the defibrillator can do is burn the heart with heat from the shock.
Medical indications for defibrillation:
- ventricular fibrillation (chaotic contraction at a speed of 200-300 beats per minute);
- ventricular flutter (contraction is rhythmic, but at a speed of about 300 beats per minute);
- atrial flutter (rhythmic but rapid contraction up to 240 beats per minute);
- atrial fibrillation (chaotic contraction, 300 beats per minute).
In case of ventricular fibrillation, so-called emergency defibrillation is performed (what, in fact, is shown in films).
In case of atrial rhythm disturbances, the procedure can be done as planned. In such cases we talk about cardioversion.
A defibrillator does not restart a stopped heart. Defibrillator starting a stopped heart
If the heart has stopped, it can be started again using a defibrillator. Such scenes in Hollywood movies always end well. The hero lies on a hospital bed without moving and only rhythmic sound signals notify that all is not lost. And then, suddenly, the signal gets stuck on one note, and an ominous straight line appears on the monitor. Doctors burst in. One of them constantly shouts: “Defibrillator! We are losing him! And here are a few discharges, dramatic music, certainly someone’s cry “LIVE, DAMMIT YOU!”, and miraculously the heart begins to beat. The hero is saved!
And everything would be fine, but... the problem is that a defibrillator cannot be used to restart a stopped heart. Alas.
In medicine, a straight line on the monitor is called asystole and means the absence of heart contractions. The idea that these contractions can be restored by electric shock seems absolutely sound.
In order to understand why this is not so, we must first understand how the heartbeat occurs.
The heart typically receives 60-100 beats per minute from stimulating cells in the upper wall of the right atrium (sinoatrial node). These specialized cells create an electrical differential between the inside and outside of the cell membrane. At a certain moment, an impulse is sent down the heart muscle, causing it to contract. This electrical signal travels throughout the heart.
If someone goes into cardiac arrest and has no pulse, an electric shock may be needed, depending on how the conduction system works. During cardiac arrest, there may be several types of electrical rhythms.
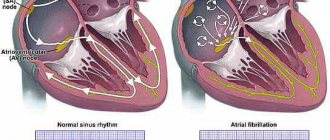
The most common heart rhythm during cardiac arrest is called ventricular fibrillation (arrhythmic contraction of the muscle fibers of the atrium). When the sinoatrial node fails to fire, many other heart cells try to do so. As a result, multiple areas of the heart are shaken simultaneously from different directions. Instead of measured beats, we see a heart attack.
Fibrillation
With this rhythm, the heart cannot pump blood through itself. The only way to get all these different areas of the heart to work in unison again is to deliver an electrical shock more powerful than the ones they create.
When you run that kind of electricity through those cells, it activates all the electrolytes from the cells at the same time. The only hope (and this is really just a hope) is that the normal functioning of cardiac electrolytes, flowing through cell membranes in an orderly manner, will resume.
In a state of asystole, a person does not have such an electrical differential that can be shown by a heart monitor. In reality, there are simply no electrolytes inside the cell that can create an impulse. In such a situation, the discharge will not help. Thus, if asystole (the complete absence of ventricular contractions) occurs before you can use a defibrillator, all you can do is burn the heart with a high temperature from the discharge.
When the procedure is not done
The only contraindication to using a defibrillator is cardiac arrest. In such cases, a procedure using electric current will simply be useless. It would be better to spend this time on other, more effective methods of resuscitation in such a situation.
In case of cardiac arrest, doctors usually try to save the patient with chest compressions and artificial ventilation; the patient is administered epinephrine, adrenaline, atropine, and sodium bicarbonate.
Contraindications to elective defibrillation:
- the presence of blood clots in the atria;
- sinus or polytopic atrial tachycardia;
- electrolyte disturbances;
- contraindications to anesthesia;
- glycoside poisoning.
Will a defibrillator be included in the list of first aid measures in Russia?
AEDs are very easy to use and were specifically designed to be used by people without medical training. In many countries, AEDs are placed in crowded areas such as stadiums, train stations, airports, universities and schools.
In our country, the use of AEDs is not yet included in the list of first aid measures, but positive changes in this direction are expected in the near future.
On October 8, 2021, the 2nd All-Russian scientific and practical conference with international participation “First Aid 2020” started in a remote format.
In this regard, Deputy of the State Duma of the Federal Assembly of the Russian Federation, member of the Committee on Health Protection Nikolai Gerasimenko focused on the need to regulate the legislative provision of first medical aid in our country. In particular, the speaker spoke about the work on the draft law on providing first aid with the use of defibrillators.
Draft federal law No. 4669777 “On amendments to Article 31 of the Federal Law “On the fundamentals of protecting the health of citizens in the Russian Federation” (regarding the provision of first aid using automatic external defibrillators) was adopted by the State Duma in the first reading on March 14, 2021.
What is a defibrillator
A defibrillator is a medical device designed to apply electric current to the heart muscle in order to restore and synchronize its rhythm. The procedure uses high voltage (about 1000 volts). During “shock therapy,” the patient’s heart receives approximately 300 J of electricity (approximately the same amount is used by a 100-watt lamp in 3 seconds).
The defibrillation method was first used in 1899. This was a scientific study on animals. Two physiologists from the University of Geneva discovered that applying a small electrical discharge to the heart can cause ventricular fibrillation, while a more powerful current, on the contrary, eliminates this process.
The first person to experience the effect of the electric discharge procedure was a 14-year-old boy. In 1947, professor of surgical sciences Claude Bec used electric current to restore normal heart rhythm in a child. In the Soviet Union, electric current treatment was initiated by V. Eskin and A. Klimov. In 1959, Bernard Lown and Baruch Berkowitz determined the optimal procedure time for various cases of arrhythmias.
The first portable defibrillator was created in 1965. The device was invented by a professor from Northern Ireland, Frank Pantridge.
The doctor was prompted to create the device by the fact that in the 1960s, defibrillators could only be used in medical institutions, but many patients with heart disease died on the way to the hospital. Pantridge's invention was very different from modern portable devices. The device weighed about 70 kilograms, and the “irons” in it were huge lead plates. But even such a device could already be transported in ambulances, and this was its huge advantage.
Treatment of cardiac pathologies with a defibrillator
Cardioversion may be performed as an emergency treatment for sudden tachycardia or as routine treatment for tachyarrhythmia when it cannot be controlled with medication. Urgent treatment is necessary when arrhythmia can turn into fibrillation, when the patient is in a pre-infarction state, heart failure is diagnosed, or a drop in blood pressure.
In planned treatment, you can combine electrical stimulation techniques and medications.
In atrial fibrillation, cardioversion is used for:
- There is no adequate effect from pharmacological treatment.
- In the presence of paroxysmal arrhythmias in Wolff-Parkinson-White syndrome.
- Medicines for hypertensive arrhythmia.
- Recurrence rate of paroxysmal arrhythmias.
- Pharmacological treatment of persistent atrial fibrillation is ineffective.
Complications after the procedure
During defibrillation, the main complications are burns, and less commonly, thromboembolic disorders of arterial blood. Burns are caused by strong discharge and are treated with corticosteroid ointments. Thromboembolism is much more difficult to treat; thrombolytic and anticoagulant drugs are used, sometimes requiring urgent surgery.
But these complications justify the goal - saving the patient's life in emergency cases. When deciding on elective cardioversion, possible negative consequences should be carefully assessed.
And here the same consequences are possible:
- Ventricular fibrillation. Occurs rarely, usually due to non-compliance with the technique. Treated with multiple blows.
- A sharp drop in blood pressure. This resolved spontaneously or with vasopressors.
- Atrial and ventricular extrasystoles.
- Pulmonary edema. It does not appear immediately, but after a few hours. Treated with diuretics, antispasmodics, oxygen inhalations.
It is impossible to restart the heart if it has been stopped completely by a defibrillator. Manipulation can only normalize the rhythm. If there is no contraction, cardiopulmonary resuscitation followed by defibrillation is used.
Conversely, cardioversion is useful for supraventricular arrhythmias and some forms of atrial fibrillation when ventricular synchronization is necessary.
Types of defibrillators and principles of their operation
A defibrillator is a device that delivers electrical impulses. It can be stationary or portable.
The device consists of three blocks:
The following types are also distinguished:
- A two-phase device that conducts current in one direction.
- Single-phase device. The operating principle of the defibrillator is based on alternating current energy, which is transmitted from one electrode to another and back.
Manual defibrillators are difficult to use but inexpensive. They are difficult to use as transport is not possible due to their size, so these devices are more common in clinics.
The advantage of automatic defibrillators is the ability to detect arrhythmias and the ability to adjust the power of the defibrillator depending on the specific situation.
This type of defibrillator is not complicated and can be used even by a beginner. However, the cost is quite high, and the choice of additional settings leaves much to be desired. There are also universal devices that combine both types.
Depending on the type of defibrillator, its maximum power also varies. Usually it is 5000-7000V.