Potassium is the main intracellular macronutrient. About 90% of all potassium ions in the body are located inside cells. Such a large difference between intra- and extracellular concentrations is necessary to maintain the membrane potential of cells, their ability to excite and transmit nerve impulses. Accurate data on the overall prevalence of hypokalemia are not available. It is only known that it is detected in 3-20% of patients undergoing hospital treatment. This disorder is somewhat more often observed in patients of cardiology and gastroenterology departments.
General information
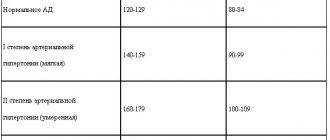
Hypokalemia means a decrease in serum potassium content to below 3.5 mmol/l, the deficiency of which can be caused by both a decrease in its reserves in the body and pathological movement into cells.
Most of the potassium (120–160 mmol/L) is normally found in the intracellular space (about 90%), and the remainder is found in the blood/bone tissue. The normal level of potassium in the body is its serum concentration from 3.5 to 5.5 mmol/l. The concentration of potassium in the blood is relatively constant, which is regulated by the processes of its entry into cells/excretion by the kidneys. The process of moving potassium from the blood through cell membranes is determined by the concentration of potassium outside the cell, the state of the membranes and cellular metabolism. The binding of potassium inside the cell occurs during the formation of protein and glycogen: it has been established that for 1 g of glycogen, 1 g of protein nitrogen and 0.3 mmol of potassium ions enter the cells. Potassium enters the body with food in an average amount of 2-3 g/day and is absorbed in the gastrointestinal tract (small intestine); excreted in urine (2-5 g), to a lesser extent in feces (less than 10 mmol). The volume/rate of potassium excretion is determined by many factors: potassium concentration in the blood, osmolarity, acid-base balance, the influence of vasopressin / aldosterone , and the rate of cell turnover.
The daily potassium requirement of an adult varies between 40–100 mmol/l. Vitamin B6 increases the efficiency of potassium absorption , while alcohol negatively affects its balance in the body. It should be taken into account that potassium from food is poorly absorbed in case of magnesium deficiency. Therefore, the lack of potassium and magnesium in the body is often interrelated. Normally, potassium balance is constantly maintained by the process of its excretion and intake with food. At the same time, the potassium content in the body is inversely proportional to the sodium content, that is, the more potassium, the less sodium, and vice versa.
Potassium takes an active part in the transmission of nerve impulses, the formation of cellular potentials, the contraction of smooth/skeletal muscle fibers, and cardiomyocytes. The macroelement increases stress resistance/physical endurance, coordinates heart rate, is responsible for normalizing blood pressure, and helps eliminate allergens/toxins from the body. Lack of potassium in the body in women and lack of potassium in men is a dangerous condition, since its functions in the body are extremely wide: potassium maintains the bioelectrical activity of cells, acid-base balance/water-salt balance; Helps stabilize heart rate, blood pressure, and maintain pH levels.
There are no reliable statistics on the prevalence of hypokalemia in the general population. It is important to understand that both manifest and especially subclinical hypokalemia are very common in clinical practice, but often remain unrecognized. However, potassium deficiency is detected in 3-20% of patients in gastroenterology/cardiology departments. The reason for the difficulty in recognizing hypokalemia is the variability/dynamism and variety of its clinical manifestations, and therefore hypokalemia imitates various organ/systemic pathologies.
Classification
Most often in clinical practice, hypokalemia is divided into:
- light
- K+ content 3-3.5 meq/l. - severe
- K+ level below 3 mmol/l.
Separately, pseudohypokalemia is distinguished, which has no symptoms and does not require treatment. A false test result can be obtained if the patient has a very high level of leukocytes (leukocytes actively absorb K+). This happens, for example, with leukemia or severe infection. Falsely elevated readings are also possible if the K+ concentration is determined in blood stored for a long time at room temperature.
Pathogenesis
The pathogenesis of hypokalemia is diverse and determined by its form. The kidneys play a major role in maintaining potassium homeostasis. The level of potassium is determined by a combination of several processes, namely: potassium filtration, secretion and reabsorption. Since potassium in the blood plasma is in a free state, it is completely filtered in the renal glomeruli; potassium ions passing through the filter are almost completely reabsorbed in the distal/proximal tubules.
The process of potassium excretion by the kidneys is under humoral control, the main role in which belongs to mineralocorticoids ( aldosterone ), which both increases the penetration of potassium ions into the cells of the distal tubule and increases the permeability of the cell membrane to potassium, promoting potassium secretion. insulin also takes part in the processes of regulation of potassium excretion by the kidneys , which reduces the excretion of potassium by the kidneys. The state of acid-base balance has a significant influence on kaliuria. Thus, with alkalosis , hypokalemia develops as a result of the transition of potassium found in the blood plasma into cells. Potassium deficiency is observed with increased/accelerated breakdown of proteins in the body, which helps to force the release of potassium.
Breast pain caused by bra
Diseases can have very mundane causes, for example, injuries caused by strong seat belt tension in a car when braking. Breast pain also affects women who wear ill-fitting bras (for example, with cups that are too small). When shopping for a bra, be sure to measure the circumference under your bust and around your chest at nipple level. There should be 1-2cm of sag in the cups because breasts swell and change shape over the course of a month, and under the bust the bra should fit snugly but not cut into the body. Be careful with underwire bras as they can put too much pressure on your breasts and cause pain.
Causes
The causes of hypokalemia are quite varied, the main ones of which include:
- Insufficient intake of potassium from food (poor nutrition/strict diets), monotonous diet.
- Excessive consumption of sugar, coffee-containing drinks, alcohol.
- Excessive intake of sodium, cesium, thallium and rubidium into the body.
- Potassium loss due to various diseases of the gastrointestinal tract ( ulcerative colitis / pancreatitis ), various intestinal infections that manifest themselves with repeated diarrhea / vomiting .
- Primary/secondary hyperaldosteronism . Under the influence of aldosterone, the process of excretion of potassium ions by the kidneys is stimulated.
- Endocrine diseases ( thyrotoxicosis Itsenko-Cushing disease/syndrome , genetically determined dysfunction of the adrenal cortex).
- Kidney diseases ( interstitial nephritis / renal tubular acidosis ), occurring with tubular dysfunction, which leads to increased potassium excretion.
- Redistribution (changes in the ratio) of potassium between the interstitium and the cell - the transition from the extracellular space of K+ into the cells. Occurs with alkalosis (pH shift to the alkaline side).
- Neuropsychic overload, excessive stress factors.
- Use of high doses of glucocorticoids.
- Taking certain medications. The table below shows the main drugs that induce hypokalemia and the mechanisms of its development.
- Other causes are large area burns hypomagnesemia , Barter-Gittelman syndrome .
Treatment of hypokalemia
The department in which patients are treated is determined by the pathology that caused the decrease in K+ (nephrology, gastroenterology, etc.). Patients in serious condition must be transferred to the intensive care unit. To begin with, all medications that can lead to hypokalemia are discontinued. The main and primary task is to normalize K+ concentration and stop life-threatening rhythm disturbances.
- Correction of potassium deficiency.
In case of mild and stable condition of the patient, oral forms of potassium preparation (KCl) are prescribed as treatment. For severe hypokalemia, intravenous administration is preferable. When combined with metabolic acidosis, hydrocarbonate and citrate salts are used. To avoid hyperkalemia, the infusion rate should not exceed 10 mEq/hour. In order to reduce the renal excretion of potassium ions, potassium-sparing diuretics (spironolactone) are added to treatment. - Fighting arrhythmias.
In the vast majority of cases, replenishment of the K+ deficiency is sufficient to achieve sinus rhythm. In some situations it is necessary to use antiarrhythmic drugs (amiodarone, propafenone, flecainide). When ventricular fibrillation develops, the only treatment option is defibrillation.
Symptoms
Symptoms of hypokalemia depend on the level of potassium in the body, however, it should be borne in mind that plasma potassium concentrations do not accurately reflect the state of potassium balance. Symptoms and complaints of patients accompanying a decrease in potassium concentration in the body are nonspecific and quite varied, so in most cases we are not talking about the clinical picture, but about various clinical masks of hypokalemia.
The main signs of potassium deficiency are observed when its total amount decreases in the range of 10-30%; a decrease in potassium content below 1.5 mmol/l causes paralysis of the respiratory muscles. Symptoms of potassium deficiency in the body in women and potassium deficiency in the body in men manifest themselves with the same symptoms.
The first signs of potassium deficiency are associated with impaired neuromuscular excitability, which is caused by impaired polarization/depolarization of cell membranes and is manifested by asthenia / muscle weakness , increased fatigue , paresthesia /muscle spasms, and decreased tendon reflexes. With chronic hypokalemia, functional disorders and structural damage to both the peripheral and central nervous systems appear, which is realized by psycho-emotional disorders in the form of hypochondriacal, asthenic or anxiety-depressive syndromes.
Sensory disturbances manifest as mild paresthesia of the limbs/face or loss of tactile/pain sensitivity or severe hyperesthesia . Movement disorders correlate with the severity/duration of hypokalemia, ranging from mild muscle weakness of the upper and lower extremities, decreased tendon reflexes, to paralysis, including respiratory muscles. Hypokalemia can also manifest itself in symptoms/changes in the digestive system (intestinal paresis, flatulence , vomiting, paralytic intestinal obstruction constipation ), as well as in the genitourinary system ( polyuria , atony of the bladder , necrosis in the kidneys).
One of the most common manifestations of hypokalemia are disorders of cardiovascular activity, which are characterized by dilation of the cavities of the heart, decreased contractile function of the myocardium, the presence of systolic murmur at the apex of the heart, and decreased blood pressure .
The damaging effect of potassium ion deficiency in the body is well reflected in the ECG, which allows it to be used as a kind of indicator of latent hypokalemia. Characteristic ECG signs of hypokalemia include ventricular extrasystoles , T wave depression/inversion, QRS prolongation, pronounced U wave, and ST segment depression (Figure below).
As a rule, with potassium deficiency, there is a decrease in mental/mental activity, manifested in lethargy, apathy, and with a significant deficiency, the development of a coma is possible.
Associated disorders
Symptoms of the following disorders include hypokalemia. Comparisons can be useful for differential diagnosis:
- Bartter's syndrome is a metabolic disorder affecting the kidneys. Main symptoms include slow growth, weakness, excessive thirst and excessive urination. Bartter's syndrome is characterized by excessive loss of potassium through the kidneys.
- Hypokalemic periodic paralysis (HPP) is a disorder characterized by episodes of paralysis with loss of deep tendon reflexes and inability of muscles to respond to electrical stimulation. The cause of HPP is unknown. The paralysis may be limited to certain muscle groups or may affect all four limbs. Attacks usually last from 24 to 48 hours. Potassium levels are usually abnormally low (ie, hypokalemia).
- Metabolic alkalosis is a disorder characterized by elevated levels of bicarbonate in the blood. Symptoms include irritability, neuromuscular hyperexcitability, low blood potassium levels (hypokalemia), muscle weakness, gastrointestinal dysmotility, and excessive urination.
To find other disorders that include hypokalemia as a symptom, enter “Hypokalemia” as a search term in the disease database.
Tests and diagnostics
The diagnosis is based on laboratory and instrumental methods of examining the patient:
- Laboratory research. The blood CBS and concentrations of potassium, magnesium, and sodium are determined. A biochemical blood test determines the concentration of urea and creatinine; in urine analysis - the presence of chlorine/relative density.
- Hormone tests. The level of aldosterone/renin is determined, and the renin-aldosterone ratio is calculated. According to indications, tests are carried out for 17-OH-progesterone, cortisol , thyroid-stimulating hormone .
- Electrocardiography. The ECG looks for characteristic ECG signs of hypokalemia (QT interval prolongation, ST segment depression, presence of a U wave).
- Instrumental research. Ultrasound/CT of the adrenal glands, ultrasound of the kidneys with Dopplerography. According to indications - echocardiography.
- In addition to determining the potassium content, diagnosing the causes of hypokalemia is also important, the algorithm of which is shown in the figure below.
Diet
There is no special diet, but adjusting the diet to include foods rich in potassium is a critical component of correcting hypokalemia. For this purpose, it is recommended to include in the diet dairy products (milk, cottage cheese and sour cream), legumes, oatmeal/buckwheat, mushrooms, potatoes, bread with bran, tomato, sea fish (mackerel, pollock, salmon, tuna, sprat), cabbage (cauliflower/white cabbage/broccoli), carrots, cucumbers, greens (parsley, spinach), seaweed, fresh fruits (peaches, bananas, kiwi, avocados, apricots), nuts, dried fruits (prunes, dried apricots, raisins), compotes, black tea, cocoa, tomato juice, freshly squeezed juices (grape, orange, carrot), chocolate.
Unnatural sugar-containing drinks (lemonade, Coca-Cola, Fanta, Pepsi) should be limited/completely excluded from the diet. The consumption of salt is also subject to restrictions, but at the same time, a salt-free diet is not allowed. It is important to consider that most of the potassium dissolves in water during heat treatment, so you need to boil foods in a minimum amount of water.
How to compensate for potassium deficiency
Pharmaceuticals offers a variety of pharmaceutical drugs, for example: Asparkam, Potassium Orotate, Panangin, Normin at an affordable price to replenish the reserves of an important macronutrient. Replenishing the body means normalizing nutrition, which is important for women during pregnancy with hypokalemia.
The macronutrient is found in large quantities in the following products:
- porridge (oatmeal, buckwheat, barley),
- bananas,
- dried fruits,
- nuts,
- pumpkin,
- melons,
- watermelons,
- mushrooms,
- meat,
- freshly squeezed carrot juice,
- apples,
- celery,
- sprouted wheat grains.
Patients with hypokalemia should avoid consuming strong coffee, sweets, and alcohol. It is recommended to steam dishes made from foods high in potassium in the oven for the purpose. However, during treatment and prevention, one should not overdo it and forget that an excess of potassium is just as harmful as its lack. May cause increased stress on the kidneys.
If patients have to take long-term courses of laxatives and diuretics, then it may be worth discussing with their doctor the selection of a replacement for potassium-sparing diuretics. It is important for athletes to consume foods containing natural minerals every day.
Prevention
Preventive measures boil down to:
- A balanced diet with a sufficient amount of potassium-containing products without violating the rules of heat treatment.
- Eliminating low-calorie diets and giving up bad habits.
- Sleep/wake optimization.
- Limiting mental and nervous overload.
- Replacing (if possible) diuretics and other medications that help remove potassium from the body. If it is impossible to replace them, it is necessary to regularly undergo laboratory testing to determine the concentration of potassium in the serum.
- Limiting table salt consumption.
- Periodic use for the preventive correction of hypokalemia Panangin (1 tablet 3 times a day) for 3 weeks.
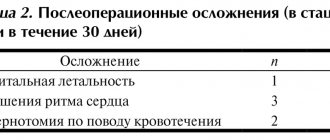
Consequences and complications
The most significant complication of hypokalemia is cardiac arrhythmia ( ventricular fibrillation / ventricular tachycardia ), which can be fatal in the absence of timely qualified medical care. In some cases, respiratory failure may develop due to weakness of the intercostal muscles/diaphragm. Hypokalemia increases sensitivity to cardiac glycosides, which is accompanied by the risk of glycoside intoxication. Rarer complications are intestinal obstruction and the development of chronic renal failure .
List of sources
- Nascimento L. Hyperkalemia and hypokalemia // Difficult diagnosis: In 2 volumes / Ed. R.B. Taylor, vol. 1. M., Medicine, 1992, p. 302-322.
- Manual of clinical laboratory diagnostics. Part 3: Clinical biochemistry/Ed. prof. M.A. Bazarnova, prof. V.T. Morozova. K., Vishcha school, 1986, p. 216-223.
- Sokovets T.G., Bogdanov E.I. Hypokalemic myoplegia//Kazan Medical Journal. 2013. pp.933–938.
- Molashenko N.V., Platonova N.M., Yukina M.Yu. and others. Primary aldosteronism. Collection of methodological recommendations. Ed. E.A. Troshina. Tver: Triad; 2021.
- Heitz U. Water-electrolyte and acid-base balance. Per. from English M.: Binom; 2009.