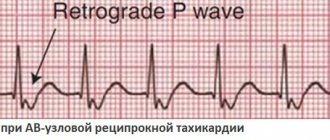
A pathological condition in which a person’s heartbeat rhythm is disturbed is called arrhythmia. Arrhythmia is divided into two types - tachycardia (increased rhythm) and bradycardia (slowed rhythm). It is often difficult for a non-specialist to understand from his own feelings how tachycardia and bradycardia differ.
Tachycardia
During attacks of tachycardia, the heart begins to beat faster than 90 beats per minute. If such a condition occurs as a result of physical activity or stress, then it is not considered a pathology and does not require treatment. But if there are signs of tachycardia that appear at rest, you should consult a cardiologist.
Types of tachycardia: sinus (rhythm disturbance of the sinus node in the right atrium), paroxysmal (rhythm disturbance outside the sinus node) and ectopic (differs from paroxysmal in that it develops very slowly).
Pathological tachycardia is caused by the following factors:
- myocardial damage;
- myocarditis,
- cardiac ischemia;
- birth defects;
- cardiomyopathy;
- complications after drug therapy.
Ventricular tachycardia cardioversion. Cardiac arrythmia
Arrhythmias requiring emergency treatment
Drugs and electrotherapeutic measures are used to treat arrhythmias. Antiarrhythmic drugs are used to treat hemodynamically stable arrhythmias, and electrotherapy for hemodynamically unstable arrhythmias. Electrotherapy includes:
- defibrillation or cardioversion
- stimulation for tachycardias (for example, treatment of ventricular tachycardias or atrial flutter)
— stimulation for bradycardia in the form of temporary transvenous or transcutaneous pacemakers (=pacemakers).
Defibrillation. During defibrillation, simultaneous depolarization of myocardial cells occurs, which creates a short-term asystole, during which the physiological pacemaker can again assume its function. The condition for this is a sufficient content of energy phosphates in myocytes.
Semi-automatic defibrillators (AED - automatic external defibrillator) are often used, installed in airports, shops, etc.
Cardioversion (or synchronized defibrillation) - electric shocks are given at a certain point in the cardiac cycle (synchronized with R-waves). The defibrillator recognizes the R wave and gives an impulse a few milliseconds after its maximum part and acts on the myocardium during the period of its repolarization. This prevents the development of possible ventricular fibrillation.
Therefore, cardioversion can only be used if there are R-waves on the ECG. Indications: atrial fibrillation, supraventricular and ventricular tachycardia. Defibrillation is used in unconscious and pulseless patients. The discharge during cardioversion is less than during defibrillation and ranges from 50 (atrial fibrillation) to 200 J (polymorphic ventricular tachycardia).
Bradycardia occurs when the heart rate is less than 60 bpm. For emergency situations, bradycardia with a heart rate less than 40 per minute is important. If the cause is known—electrolyte disturbances, increased vagal tone, cardiac tamponade, myocardial ischemia—then it is necessary to eliminate them.
For severe but hemodynamically stable bradycardia, atropine is first prescribed. However, it is necessary to exclude AV block below the His bundle (trifascicular block in the bundle branches), while the heart rate is about 30, the QRS complexes are deformed, dilated, the atria and ventricles contract independently of each other. Secondarily, catecholamines . If bradycardia persists, then a temporary pacemaker .
Atropine can be administered at a dose of 0.5-1 mg every 2-5 minutes up to a maximum dose of 0.04 mg/kg (70 kg person - approximately 3 mg). If IV access is not available, insertion into the endotracheal tube is acceptable. In this case, the dose is increased by 2-3 times and atropine is diluted in 10-20 ml of physiological solution. With blockade below the His bundle (2nd degree AV block, Mobitz II, III degree), atropine can lead to a paradoxical further decrease in frequency and worsening of the condition. In such cases, catecholamines are first used, or even better - stimulation right away.
Catecholamines (orciprenaline and adrenaline). They are used if the heart rate does not increase after atropine and immediately upon the onset of asystole along with resuscitation measures.
In such cases (when catecholamines are used for bradycardia), implantation of a pacemaker is necessary.
Catecholamines are administered as a bolus - orciprenaline 0.25-0.5 mg and/or adrenaline 0.02-0.1 mg (endotracheal administration 2-3 times the dose increased by 10-20 ml of saline solution).
Indications for a temporary pacemaker (artificial pacemaker):
— in case of myocardial infarction with the development of AV block of the second degree Mobitz II with a frequency of 2:1 and higher, AV block of the third degree, progressive block of both fibers
- for symptomatic bradycardia before implantation of a permanent pacemaker
- in case of intoxication with bradycardia
- in other emergency conditions with asystole or symptomatic bradycardia refractory to atropine.
Table 1. Tactics for bradycardia.
With tachycardia, the heart rate is more than 100 beats per minute. For emergency situations, tachycardia with a heart rate of more than 150 beats per minute is important. For the treatment tactics of tachycardia, hemodynamically stable and hemodynamically unstable tachycardias are distinguished.
For hemodynamically unstable tachycardias . which are accompanied by shock symptoms, loss of consciousness, pulmonary edema, antiarrhythmic drugs, defibrillation or cardioversion are urgently used. Treatment of hemodynamically stable patients depends on the type of tachycardia.
The strength of the shock during defibrillation depends on the type of tachycardia. For example, tachycardias with narrow QRS complexes, against the background of atrial fibrillation, respond well to a discharge of 50-100 J. Polymorphic ventricular tachycardias and ventricular fibrillation are defibrillated with a discharge of 200-300 J; if ineffective, the charge increases to 360 J. With persistent ventricular fibrillation Along with resuscitation measures, amiodarone (150-300 mg IV) is administered.
If the patient requires defibrillation or cardioversion and is conscious, sedatives (eg, midazolam) or analgesics (eg, morphine) are used before the procedure. The choice of analgesic should be based on the hemodynamic and respiratory status of the patient. If consciousness is maintained before cardioversion, amiodarone can be administered intravenously.
Rice. 1. Ventricular fibrillation.
Hemodynamically stable tachycardias are treated with medication. A 12-lead ECG is performed. According to ECG, tachycardia is divided into 2 groups, which require different treatment. To differentiate supraventricular and ventricular tachycardias, the decisive criterion is the width of the QRS complex. When the width of the QRS complex is less than 120 ms, arrhythmias originate above the His bundle - supraventricular. The exception is supraventricular tachycardias with bundle branch block and the presence of an additional bundle in Wolff-Parkinson-White syndrome (the QRS complex will be wider than 120 ms, but the tachycardias are supraventricular). When the QRS complex is more than 120 ms - ventricular tachycardia.
Table 2. Tactics for tachycardia.
Atrial fibrillation, atrial flutter. The QRS complex is less than 120 ms, the RR intervals are not the same. Treatment - either slow down conduction in the AV node (verapamil, β-blockers, glycosides), or cardioversion. Cardioversion can be performed only when atrial fibrillation has been present (documented) for less than 48 hours or thrombi in the atria of the heart have been excluded using intraesophageal ultrasound. In all other cases, normalize the rate and plan, if indicated, elective cardioversion.
Rice. 2. Atrial fibrillation and normal sinus rhythm.
Regular tachycardias with narrow QRS complexes. These are supraventricular tachycardias. First, vagal tests are used (carotid sinus massage, Valsalva maneuver). If ineffective, a bolus of adenosine is administered intravenously (6-12-18 mg in increasing order). In 95% of cases, such tachycardias disappear after adenosine. As an alternative or if adenosine is ineffective, calcium antagonists (verapamil 2.5-5 mg IV) and β-blockers are used. If even after these measures the tachycardia does not go away, then flecainide and propafenone are used.
Rice. 3. Supraventricular tachycardia.
Rice. 4. Supraventricular tachycardia and the effect of adenosine.
Tachycardia with wide QRS complexes. Typically of ventricular origin (80%). In some cases, however, it is supraventricular, when there is an additional abnormal path of impulse conduction from the atria to the ventricles (for example, in Wolff-Parkinson-White syndrome).
Rice. 5. Delta wave in Wolff-Parkinson-White syndrome.
When treating hemodynamically stable tachycardias with wide QRS complexes, many mistakes are made, because tachycardias of ventricular origin are incorrectly interpreted as supraventricular with bundle branch block. It is incorrectly believed that all tachycardias with normal hemodynamics and wide QRS complexes are necessarily supraventricular with bundle branch block. Therefore, any tachycardia with wide QRS complexes should be considered ventricular until proven otherwise. In some cases, however, when a supraventricular origin of wide QRS tachycardia is suspected, a bolus of adenosine can be administered for diagnostic purposes.
Rice. 6. Monomorphic ventricular tachycardia.
For such tachycardias, hemodynamically stable with wide monomorphic regular QRS complexes, amiodarone or, as an alternative, ajmaline is recommended. The use of ajmaline is practiced in Germany. One of its advantages is that it also has a beneficial effect on supraventricular tachycardias. It can also be used for atrial fibrillation with Wolff-Parkinson-White syndrome, while adenosine, verapamil and cardiac glycosides are contraindicated. One of the reasons is that conduction through the anomalous additional bundle is accelerated due to the shortening of the refractory period of the cells of this bundle and the simultaneous slowdown of conduction in the AV node.
Also, for such tachycardias in cases where there is a heart attack or ischemic damage, lidocaine is sometimes used. Other antiarrhythmics, such as propafenone, flecainide, play a secondary role as reserve drugs.
When treating polymorphic ventricular tachycardias, it is of great importance to identify “torsades de pointes” arrhythmias against the background of congenital or acquired syndrome of prolongation of the QT interval. The ECG shows a typical sinusoidal waveform on the ECG. Pathogenesis - there are multiple areas of discharged myocardium, so drugs that slow down repolarization, such as sotalol and ajmaline, cannot be used. Magnesium is prescribed in high doses (1-2 g IV) or b-blockers, catecholamines, lidocaine, electrical stimulation.
Rice. 7. Tachycardia of the “pirouette” type.
For polymorphic ventricular tachycardias, which are not a consequence of delayed repolarization, but, for example, arose as a result of ischemic changes or dilated cardiomyopathy, amiodarone is used intravenously (150-300 mg). At the same time, correction of electrolyte disturbances and treatment of ischemic changes should be carried out. It is also possible to use β-blockers and lidocaine.
Rice. 8. Polymorphic ventricular tachycardia.
Tests on the topic arrhythmia.
1). What medications are used to treat life-threatening bradycardia?
a) sodium channel blockers, such as lidocaine, which affect the spontaneous depolarization of pacemaker cells to increase heart rate
b) only adrenaline, because with bradycardia it is very important to increase blood pressure
c) intravenous or endotracheal administration of atropine or catecholamines
d) statins and ACE inhibitors are used together with β-blockers to have a long-term effect on risk factors for cardiovascular diseases
e) There are no medications to treat life-threatening bradycardia.
2). What is the best thing to do for hemodynamically unstable bradycardia that is resistant to medications?
a) mouth-to-nose artificial respiration
b) external cardiac massage through the chest
c) percutaneous or transvenous endocardial stimulation, before this, if necessary, external cardiac massage
d) continuation of alternate administration of atropine and adrenaline
e) defibrillation to activate the pacemaker
3). What parameter should be used when choosing a method of therapy (defibrillation or drug treatment) for tachycardia?
a) according to heart rate on the ECG
b) the width of the QRS complex is decisive
c) due to underlying heart disease
d) by hemodynamic stability or instability during tachycardia
e) according to the patient’s subjective sensations of pain
4). What should be done in case of hemodynamically unstable tachycardia with progressive loss of consciousness?
a) administration of adenosine in increasing doses
b) immediate IV administration of amiodarone is better than all other measures, especially the administration of other drugs
c) rapid cardioversion or defibrillation
d) intubation and intravenous administration of catecholamines to stabilize blood circulation
e) endocardial stimulation to stop tachycardia
5). What is the optimal treatment for hemodynamically stable atrial fibrillation of unknown duration?
a) oral anticoagulants to reduce the risk of stroke
b) cardioversion to restore rhythm and prevent electrical remodulation of the myocardium
c) drug frequency control, cardioversion after excluding thrombi in the atria of the heart
d) class IC antiarrhythmics for painless cardioversion without prior exclusion of thrombi
e) potassium, magnesium and amiodarone
6). What treatment is recommended for symptomatic atrial flutter?
a) rapid cardioversion due to the danger of the impulse passing through the AV node with a frequency of 1:1
b) with an accurate diagnosis, administration of adenosine
c) the same as with atrial fibrillation
d) emergency catheter ablation of the cavo-tricuspid isthmus
e) anticoagulants for several weeks, because the risk of thromboembolic complications is as high as with atrial fibrillation
7). What treatment is used for hemodynamically stable rhythmic tachycardia with narrow QRS complexes?
a) adenosine after vagal tests, alternatively if verapamil or class IC antiarrhythmics are ineffective
b) cardioversion with energy 50-100 J
c) amiodarone (300 mg/30 min) followed by administration for 7-10 days at a rate of 50 mg/h
d) electrical stimulation via transvenous electrodes
e) cardiac glycosides, potassium and magnesium
8). Regular tachycardias with wide QRS complexes:
a) are supraventricular tachycardias with bundle branch block
b) supraventricular tachycardia with bundle branch block in cases where they do not lead to hemodynamic instability
c) tachycardias of ventricular origin and until evidence to the contrary should be treated as ventricular tachycardias
d) tachycardia with additional conduction bundle during atrial flutter
e) tachycardia due to prolongation of the QT interval
9). What is used for polymorphic ventricular tachycardia in connection with prolongation of the QT interval?
a) ajmaline to stop tachycardia and shorten the QT interval
b) IV magnesium and lidocaine, as well as stimulation and catecholamines to increase heart rate
c) IV amiodarone for effect on the QT interval
d) sedation, for example, diazmepam
e) class Ic antiarrhythmics (flecainide, propafenone), with signs of heart failure additionally cardiac glycosides
Bradycardia
Bradycardia is a condition in which the heart rate slows to 50–30 beats per minute. A slow pulse is considered normal in athletes and young healthy people (if the person does not experience discomfort, dizziness or fainting).
With a reduced heart rate, a person feels dizzy and weak, and cold sweat appears. Due to slow blood flow, organs do not receive enough oxygen. In some cases, fainting may occur.
Bradycardia occurs sinus and with heart block. It develops against the background of the following diseases:
- sclerotic changes in the myocardium;
- meningitis;
- brain tumor;
- hypothyroidism;
- liver damage;
- typhoid fever.
Bradycardia also develops with nicotine, lead poisoning or as a result of drug treatment with glycosides.
The basic rules of heart rhythm are regularity and clarity. At any time of the year, our fiery engine beats its beat monotonously. But sometimes glitches occur. Let's figure out why.
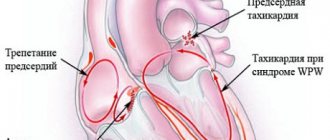
Heart rhythm disturbances (simply arrhythmia) are a group of diseases of the heart and blood vessels, which are based on irregular heartbeats of varying frequencies.
If the heartbeat quickens, they talk about tachycardia, slows down - about bradycardia, breaks out “out of turn” - about extrasystoles, but if the heart impulse makes forced stops along the way or jumps, as if over bumps, it’s about heart block.
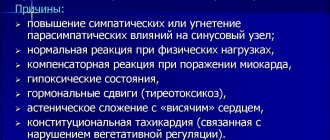
Causes of heart rhythm failure
The uniqueness of the heart muscle lies in its self-starting “clock” mechanism. Impulses generated in the heart lead to its contraction and, as a consequence, to the release of blood to the periphery.
When something interferes with the heart, it is forced to slow down or speed up, and sometimes even freeze, as if waiting for help. Under the influence of harmful factors, the impulse can get lost in “its own yard” or meander around the neighborhood in search of a way out.
The following can also disrupt the smooth functioning of the heart:
- nearby organs (thyroid and pancreas, gall bladder),
- medicines,
- germs and viruses,
- heat and cold.
How long the heart can withstand it depends on the strength and time of exposure to the harmful factor. When it copes, the changes are superficial. “The clouds have cleared” - the heart is beating as if nothing had happened. If the lesion sweeps through like a hurricane and affects the structure of the heart, the prognosis for recovery is not so favorable.
Symptoms of arrhythmia
Whether you feel an arrhythmia or not depends on many factors:
- cheerfulness of your spirit,
- state of the nervous system,
- sensitivity
- and tolerance to any changes in the body.
There are people who have no complaints at all. They look with undisguised surprise at the doctor who discovered a failure in the heart. Others, on the contrary, cannot sleep and work peacefully, feeling a slight somersault in their chest. Both have the right to be.
The classic manifestation of rapid heartbeat (tachycardia) is a feeling of pulsation in the heart area, accompanied by anxiety.
If the frequency at rest is too high (over 120 beats/min), the heart does not have time to rest and be fully filled with blood, which leads to reduced blood output and oxygen starvation. Then pain sets in, a feeling of constriction in the chest and lack of air.
If the pulse - with bradycardia - slows down so much (up to 40 beats/min) that the organs do not receive enough blood, weakness, dizziness, and even loss of consciousness occur.
Extrasystoles (or extraordinary contractions) are often not felt at all. Although in emotional people they manifest themselves as sensations of freezing, tumbling in the chest, which sometimes causes panic.
Well, intracardiac blockades are not at all visible to the “naked eye” unless they are accompanied by a decrease in heart rate.
The absence of complaints about arrhythmia sometimes turns into disaster. Seeking medical help in such cases is delayed, which means that the heart does not receive the medications it needs on time.
Arrhythmia is a signal from the heart that there is a problem
It is important to remember: any arrhythmia is a signal of an imbalance in the body.
Arrhythmia cannot be ignored due to the unpredictability of the consequences.
Of course, it may happen that you live to be 100 years old without experiencing those same somersaults in your heart. It is much worse when obvious episodes of rapid heart rate, left unattended, trigger atrial fibrillation, a disease that leads to disability. According to statistics, the frequency of this rhythm disorder after 50 years of age doubles with each subsequent decade of life: from 0.5% at the age of 50-59 years to 9% in 80-89 year olds (Bruggenjurgen B., Rossnagel K., Roll S. et al “The impact of atrial fibrillation on the cost of stroke: the Berlin acute stroke study,” Value Health, 2007, Vol. 10, pp. 137–143).
If you feel interruptions, hurry to get an ECG
At home, “catching” a rhythm failure is difficult, but possible. Sometimes it is visible on the screen of a semi-automatic blood pressure monitor in the form of a cardiac complex icon.
Some tonometers have a special arrhythmia indicator (PAD technology), which allows you not to miss a “lost” pulse.
This option is suitable for those who have no complaints about heart function.
If there is no shortage of disturbing sensations (fading and increased heart rate worries you all day long), go to the clinic, do an ECG and show it to a therapist or cardiologist. And follow your doctor's recommendations.
Do not self-medicate arrhythmias
Many antiarrhythmic drugs have side effects and can provoke rhythm disturbances, which means there is a risk of increasing the disturbances or transforming them into a more severe form.
An experienced doctor will listen to the heart, count the pulse, compare the data with the ECG and only then prescribe treatment. If the interruptions are not caught by a regular ECG tape, heart contractions will be assessed on a long tape or from a daily ECG recording (using Holter monitoring).
Treatment: tablets for some, pacemakers for others
As a rule, arrhythmia is treated with tablets. The most harmless of interruptions respond well to treatment with sedatives.
In case of rapid heartbeat and extrasystoles, medications are prescribed that slow down the pulse. If several extrasystoles are found during bradycardia (when the pulse is already rare), it is fought with drugs that increase the pulse.
If there are many interruptions and they worsen the quality of life, they resort to antiarrhythmic drugs. When changes in the heart have affected its structure, it is not always possible to reduce complaints to zero. Then the medications must be taken long-term under ECG monitoring.
Pacemaker. Photo from wikimedia.org
Installing a pacemaker (a device designed to maintain the heart rhythm) is an extreme measure that is not necessary for everyone. It is given only in cases of severe heart block, leading to prolonged cardiac arrest and, as a consequence, fainting. If this problem occurs, the patient will be referred to an arrhythmologist. In Belarus, there are arrhythmologists in large interdistrict centers, regional hospitals and the Republican Scientific and Practical Center “Cardiology”.
How to live with arrhythmia
The appearance of arrhythmia in any case will require a revision of the usual way of life: changing habits, routines, attitudes towards physical activity and nutrition. Be sure to find a doctor who you can see regularly. He will help monitor the work of the heart, knowing the individual characteristics of the course of the arrhythmia, select medications for emergency care and, if necessary, for continuous use.
Managing arrhythmia is a joint work of the doctor and the patient, and they are treated not only with drugs and devices, but also with a kind word spoken from the heart.
Main photo of the article from yourmusiclessons.com
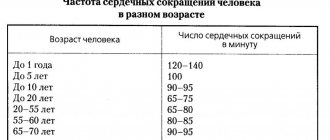
Diagnosis of tachycardia and bradycardia
When visiting a therapist, the doctor will prescribe a number of tests. The main type of diagnosis of arrhythmia is an ECG. There are many ECG signs to identify one or another type of arrhythmia. After the doctor determines what type of arrhythmia is developing in the patient, he will prescribe the optimal treatment.
The Medicenter clinic network employs qualified cardiologists and has modern equipment installed. With us you can undergo a comprehensive examination, establish or confirm your diagnosis and receive treatment recommendations.