Most cases of angina are associated with a sharp increase in the level of physical or psycho-emotional stress. However, there are exceptions to this rule. Thus, Prinzmetal's angina, also called variant, vasospastic or spontaneous, usually develops in a patient who is at rest. The typical time for symptoms to occur is between midnight and the wee hours of the morning. The pain syndrome is intense, spreading to the head or arms, reminiscent of signs of seizures. It is more often observed in smokers, patients with high cholesterol or blood pressure, but can also occur in healthy people. Thanks to modern diagnostic methods and a thoughtful course of treatment while eliminating bad habits or factors, it is possible to significantly reduce the frequency of attacks and make them less painful.
Angina pectoris: general information
If, as you age, you begin to notice that heart pain occurs after physical activity, immediately consult a cardiologist. There is a high probability that you are developing a heart disease called angina pectoris FC 2. Attacks of pain pass, so many people tend to ignore them. However, the result and direct consequence is myocardial infarction. An even worse option: sudden cardiac arrest. Do not expose yourself to mortal risk - get examined using professional diagnostic equipment at the first symptoms of angina pectoris! Now you have a unique opportunity to undergo a free consultation with a specialist and a set of preparatory examinations when enrolling in a course of enhanced external counterpulsation or shock wave therapy of the heart:
Promotion
Just until the end of autumn, undergo a free consultation and a set of preparatory examinations* when registering for a course of enhanced external counterpulsation or shock wave therapy of the heart.**
Send a request
* Check the details of the Promotion by phone. **Has contraindications; consultation with a doctor is required.
Enhanced external counterpulsation (EECP) Cardiac shock wave therapy (SWTS)
Hurry up to apply, the promotion period is limited.
Additional Methods
Another option for diagnosing Prinzmetal's angina is a hyperventilation test. In this case, doctors ask the patient to breathe deeply and frequently for a short period of time, while measuring all his indicators.
In the case when, during an experiment, the concentration of hydrogen ions in the blood decreases, smooth muscles begin to contract. Previously, this technology was quite widespread, but recently it has been used less and less, since the level of reliability is not high enough.
What is cardiac angina?
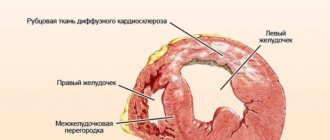
The disease is the most common form of coronary heart disease. Its danger should not be underestimated, because against its background heart failure develops quite quickly. Not far from a heart attack!
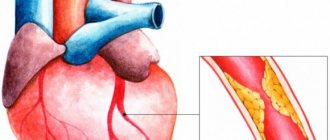
The disease develops in men after 55 years, in women - after 64. The reason is a partial (50-70%) narrowing of the coronary arteries that supply blood to the heart tissue. The narrowing occurs due to the deposition of atherosclerotic plaques on the walls of blood vessels and the formation of blood clots. They impede blood circulation, the heart lacks oxygen and nutrients. Especially during times of physical and emotional stress, when the heart muscle works actively and requires more oxygen. The arteries are not able to satisfy her need. That's when you experience attacks of pain.
Pathogenesis
The main pathogenetic mechanism is coronary artery spasm. Erosion forms in the endothelium, fibromuscular dysplasia forms, and the number of cells in the adventitia increases. The tone of the coronary vessels depends on the balance of vasodilator and vasoconstrictor factors. Among the vasodilating factors is nitric oxide. In atherosclerosis, the production of this factor by the endothelium is presumably reduced or it is actively degraded. As a result of this process, the activity of vasoconstrictor agents increases and spasm of the coronary arteries develops. An important role is played by a lack of NO and an excessive amount of endothelin.
Severe spasm leads to transmural ischemia, which is characterized by dyskinesia of the left ventricular wall. It can be recorded using EchoECG. The cause of ischemia is a pronounced transient decrease in oxygen delivery. The following factors lead to spasm of the coronary artery:
- taking cocaine
- smoking
- insulin resistance
- hypomagnesemia
- taking sumatriptan or ergotamine
- vitamin E deficiency
- staying in the cold
- hyperventilation
How does the disease develop?
It is at such moments that common signs of angina pectoris appear in women and men: you feel a lack of air, arrhythmia. At this time, chemical changes occur in the myocardium associated with metabolic disorders, a decrease in the synthesis of substances, and the accumulation of acids. The functions of the myocardium are gradually disrupted, and its metabolism changes.
What causes this disease? There are certain factors:
- high cholesterol levels;
- obesity when consuming excessive amounts of fats and carbohydrates;
- physical inactivity disrupts lipid volume;
- smoking causes oxygen starvation of cells and arterial spasm;
- arterial hypertension causes myocardial tension;
- anemia, intoxication contribute to oxygen starvation;
- diabetes mellitus increases the risk of ischemia;
- increased blood viscosity is a direct risk of blood clots;
- psycho-emotional stress (especially in women) worsens myocardial nutrition.
Risk factors [edit]
Some agents have been reported to cause an attack of variant angina. These agents include:
- recreational agents (eg, nicotine in tobacco and other forms, alcoholic beverages, marijuana, cocaine);
- catecholamine-like stimulants (eg, adrenaline, dopamine, various amphetamines);
- a drug that contracts the uterus, ergonovine;
- parasympathomimetic drugs (eg, acetylcholine, methacholine);
- anti-migraine medications (such as various triptans) and;
- chemotherapy drugs (eg 5-fluorouracil, capecitabine).
- High energy drink consumption has been associated with variant angina.
In addition, hyperventilation and virtually any stressful emotional or physical event (eg, exposure to cold) that is expected to cause a significant increase in blood catecholamine levels can cause variant angina. [3] [16]
Stable angina (tension): signs and symptoms
If periodic attacks that occur as a result of exercise last more than 1 month, doctors diagnose “stable angina.” The pain is relieved after taking nitroglycerin.
Depending on how strong the load can cause an attack in the patient, functional classes of the disease are distinguished.
- Angina pectoris FC 1 is characterized by good tolerability, and signs of angina in men and women are noticeable only with excessive stress.
- Angina pectoris FC 2 is manifested by some limitation in normal activities: an attack begins when walking more than 500 m, climbing to the 1st floor, or emotional excitement. With coronary artery disease and angina pectoris FC 2, the first hours after waking up are difficult to bear. Cold weather also has a negative effect.
- Angina pectoris FC 3 is already a serious limitation of normal physical and emotional activity. Obvious signs appear during normal walking at a distance of 150-200 m on level ground, or climbing one floor. Also, angina pectoris FC 3 develops due to anxiety.
- Stable angina pectoris FC 4 occurs after minimal exertion. The patient is unable to perform simple physical activities. This class closely borders on resting angina, i.e. one that is not associated with loads.
This classification allows the doctor to act more accurately when prescribing medications and treatments.
Description
Prinzmetal's angina is a disease characterized by cyclical attacks of chest pain resulting from spasm of the arteries supplying blood to the heart muscle.
In medical practice, you can find other names, such as variant, spontaneous, vasospastic angina. It was first described by the American cardiologist M. Prinzmetal in 1959. In total, about 3% of patients with coronary heart disease suffer from the pathology. According to my personal observations, the disease is more often found in heavy smokers who have diseases such as:
- arterial hypertension;
- peptic ulcer;
- chronic hepatitis of viral and toxic etiology.
Angina at rest: signs and symptoms
It is characterized by the manifestation of characteristic symptoms in a calm state - at night and especially in the morning after waking up. Typically, angina at rest is diagnosed using 24-hour monitoring. Most often, attacks are caused by increased blood pressure and psycho-emotional stress. Unfortunately, any troubles at work or family quarrel can provoke an attack. And sometimes it is enough to change the position of the body.
This type includes vasospastic angina, the cause of which is a sudden spasm of the coronary vessels. And also post-infarction - manifesting itself 10-14 days after the heart attack.
Forecast
Currently, this disease is considered by cardiological communities as a form of progressive coronary insufficiency similar to unstable angina. Consequently, the long-term prognosis of the pathology will, to put it mildly, not be the most optimistic. In 20% of cases, acute myocardial infarction (“heart attack”) develops in the first six months, and 10% of patients experience death. A long-term remission may occur with a resumption of symptoms years later. Sudden coronary death occurs in 0.5% of cases. The risk of complications depends on the following factors:
- frequency and severity of anginal attacks;
- current condition of the coronary vessels;
- adequacy of drug therapy;
- patient compliance, especially with regard to lifestyle correction.
Prinzmetal's angina (variant, vasospastic) today is a reason for scientific debate, because the question of the clarity of the pathogenesis of the disease remains incompletely studied.
Unstable angina: signs and symptoms
Unlike stable angina, this type of disease changes its behavior, so it is important to constantly be under medical supervision in the first two months after the first attack. Obvious symptoms of unstable angina: changing frequency, duration, intensity of attacks. They can also start at night.
In turn, unstable angina is divided into:
- into classes depending on the nature and severity (initial, subacute and acute stages);
- into groups according to the conditions of occurrence (primary, secondary, post-infarction);
- into groups during therapy (the disease develops during procedures, medication, intensive treatment).
Characteristics
Prinzmetal's angina is clearly visible on the ECG. This study shows characteristic changes. They usually appear during an attack, and when it ends, the indicators gradually return to normal. From the diagram you can see that during an attack the RS-T segment rises above the isoelectric line. The T turns into a tall prong. These are key features that help distinguish variant angina from other subtypes of angina.
Changes in QRS are diagnosed: Q becomes a pathological wave, R becomes larger than normal, QRS widens.
Failures in the functioning of the ventricle lead to disturbances in the rhythm of the heartbeat. In particularly difficult cases, ventricular fibrillation is diagnosed. In addition, atrioventricular conduction is affected. When the pain syndrome passes, Prinzmetal's angina is characterized by a fairly rapid restoration of all indicators to standard values.
To diagnose the disease, it is customary to resort to a bicycle ergometer test and coronary angiography.
Symptoms of angina in women and men
Pain
Most patients report the following symptoms of an angina attack. First of all, cutting, pressing pain in the chest. Many people complain that their heart “burns” or their throat “tightens.” At the same time, you instinctively want to press your hand or fist to your chest. Often the pain migrates to the left shoulder, neck, arm, and shoulder blade. It may grow or disappear suddenly. Symptoms clearly and distinctly appear during exercise, when the patient is diagnosed with IHD angina pectoris FC 2.
Pain can occur after physical exertion, stress, high blood pressure, or overeating. At night - due to stuffiness or low air temperature. Often the attack is accompanied by arrhythmia.
External symptoms and signs of angina pectoris
It is quite simple to identify an attack by its external manifestations. Pay attention to the following signs of angina: the person turns pale, sweat appears on the forehead, his face expresses suffering; fingers lose sensitivity, hands become cold; the patient breathes intermittently and rarely; the onset of an attack is accompanied by a rapid pulse.
Important point
Prinzmetal's angina is characterized by attacks that are very severe and last for a long time. In many ways, this is where the Latin name for the manifestation came from - “anginal pain”, since in Latin ango means “soul”.
An attack of angina is characterized by a feeling of compression of the heart. Pain syndrome manifests itself in the sternum on the left, in the scapula. Often the pain radiates to the arm or shoulder. The sensations are burning, hard to bear, giving rise to the fear of death. Most often, attacks occur in the early morning and at night. When the intensity of the pain syndrome is high, tachycardia is provoked, the rhythm of the heartbeat is disrupted, and the patient literally bleeds into sweat. There are frequent cases of hypotension leading to loss of consciousness.
What can the disease be confused with?
As for diseases not related to the cardiovascular system, based on the symptoms and signs, angina pectoris can be mistaken for:
- osteochondrosis of the cervical or thoracic spine;
- vegetative-vascular dystonia;
- gastrointestinal diseases (diaphragmatic hiatal hernia);
- pleurisy, pulmonary embolism;
- pinched nerves.
Usually this disease is confused with the onset of myocardial infarction. The signs are really very similar. The main difference is that an attack of angina is relieved by taking nitroglycerin. In case of a heart attack, the medicine does not work or relieves pain only slightly and temporarily.
Specifics of conducting an ECG
Since it is known that Prinzmetal’s angina is most accurately determined by ECG, but the data must be taken exactly during the attack, if this pathology is suspected, the patient is prescribed a 24-hour study. This is called Holter monitoring in medicine.
By studying the patient's body, doctors receive reliable information about ischemia, including the moment when pain begins. The patient, in turn, must keep as complete a diary as possible throughout the day, describing actions and sensations every hour. Next, doctors compare the diary and ECG and draw conclusions about the presence and degree of development of the pathology.
Where can I get diagnosed and treated?
Rest assured that your heart is not in danger! If the first symptoms and signs of angina appear, consult a qualified healthcare provider. Cardiologists at the CBCP Center for Circulatory Pathology are ready to help you. The clinic will offer professional consultation and modern types of diagnostics, through which the doctor will receive objective, detailed and accurate information about the disease.
If you discover serious violations, do not despair! The level of medicine at CBCP makes it possible to effectively treat complex cardiovascular diseases using medicinal and non-surgical methods.
Diagnostic features
Despite the fact that modern science has already well studied Prinzmetal's angina, the symptoms and treatment of this pathology, diagnosing the disease is still a serious problem. It was not possible to develop an instrumental method showing sufficient reliability.
Coronary angiography is considered the most correct and informative method. In this case, the heart vessels are examined by injecting a contrast agent into the patient’s body, after which X-ray irradiation is performed.
If a contrast agent is injected into the body or a catheter is placed in the vessel, this can provoke a spasm. It is this fact that is studied during medical experiments on a patient, since such a spasm of the vessel makes it possible to speak with a high degree of reliability about Prinzmetal’s angina. The drug ergonovine is usually used, which enhances the ability of smooth muscles to contract. To remove the narrowing, nitroglycerin is injected into the vein.
Links[edit]
- "A variant of angina". www.escardio.org
. Retrieved April 2, 2021. - Wu, Taixiang; Chen, Xiyan; Deng, Lay (November 24, 2021). "Beta blockers for unstable angina". Cochrane Database of Systematic Reviews
.
2017
(11):CD007050. DOI: 10.1002/14651858.cd007050.pub2. PMC 6486012. - ^ abcdefghijklmnopqrs Ahmed B, Creager MA (April 2021). "Alternative causes of myocardial ischemia in women: an update on spontaneous coronary artery dissection, vasospastic angina, and coronary microvascular dysfunction". Vascular Medicine (London, England)
.
22
(2): 146–160. DOI: 10.1177/1358863X16686410. PMID 28429664. - ^ ab Swarup S, Grossman SA (2018). "Vasospasm of the coronary arteries." PMID 29261899. Quote journal requires |journal=(help)
- ^ ab Prinzmetal, Myron; Kennamer, Rexford; Merliss, Reuben; Wada, Takashi; Bohr, Nazi (1959). "Angina I. Variant form of angina." American Journal of Medicine
.
27
(3): 375–88. DOI: 10.1016/0002-9343 (59) 90003-8. PMID 14434946. - ^ab Parkinson, John; Bedford, D. Evan (1931). "Electrocardiographic changes during short-term attacks of angina." Lancet
.
217
(5601): 15–9. DOI: 10.1016/S0140-6736(00)40634-3. - Brown, G.R.; Holman, Delavan W. (1933). "Electrocardiographic study during an attack of angina." American Heart Journal
.
9
(2): 259–64. DOI: 10.1016/S0002-8703(33)90720-6. - Kemp HG, Jr.; Vokonas, P.S.; Cohn, P. F.; Gorlin, R. (June 1973). “Anginal syndrome associated with normal coronary arteriograms. Report on six years of experience." American Journal of Medicine
.
54
(6): 735–42. DOI: 10.1016/0002-9343 (73) 90060-0. PMID 4196179. - Smolensky MH, Portaluppi F, Manfredini R, Hermida RC, Tiseo R, Sackett-Landin LL, Haus EL (June 2015). “Daily and round-the-clock modeling of human diseases: cardiac, vascular and respiratory diseases, conditions and syndromes.” Sleep Medicine Reviews
.
21
: 3–11. DOI: 10.1016/j.smrv.2014.07.001. PMID 25129838. - ^ abcd Harrison's Cardiovascular Medicine 2/E
(2nd ed.). New York: McGraw-Hill Education/Medical. 2013-08-02. ISBN 9780071814980. - Seguela PE, Iriart H, Achar R, Montaudon M, Roudaut R, Thambo JB (April 2015). "Eosinophilic heart disease: molecular, clinical and imaging aspects". Archives of Cardiovascular Diseases
.
108
(4):258–68. DOI: 10.1016/j.acvd.2015.01.006. PMID 25858537. - Kajihara N, Tachiyama Y, Takefus T, Takada A, Takata A, Saito K, Meroi T, Yasui W (2013). "Eosinophilic coronary periarteritis (vasospastic angina and sudden death), a new type of coronary arteritis: a report of seven autopsy cases and a review of the literature." Virchows Archiv
.
462
(2):239–48. DOI: 10.1007/s00428-012-1351-7. PMID 23232800. - Kounis NG (October 2016). "Kunis syndrome: an update on epidemiology, pathogenesis, diagnosis, and therapeutic management." Clinical Chemistry and Laboratory Medicine
.
54
(10): 1545–59. DOI: 10.1515/KU-2016-0010. PMID 26966931. - “What is a sore throat?” . National Heart, Lung, and Blood Institute. Retrieved April 28, 2010.
- "Prinzmetal's Angina, Variant Angina and Inversa Angina". American Heart Association. Retrieved June 20, 2015.
- ^ B s d e g Harris JR, Hale GM, Dasari TW, Schwier NC (September 2016). "Pharmacotherapy of vasospastic tonsillitis." Journal of Cardiovascular Pharmacology and Therapeutics
.
21
(5): 439–51. DOI: 10.1177/1074248416640161. PMID 27081186. - ^ abc Nishizaki M (December 2021). "Life-threatening arrhythmias leading to syncope in patients with vasospastic angina". Journal of Arrhythmia
.
33
(6):553–561. DOI: 10.1016/j.joa.2017.04.006. PMC 5728714. PMID 29255500. - ^ abcd Kundu A., Vaze A., Sardar P., Nagy A., Aronou V.S., Botkin N.F. (March 2021). "Variant angina and aborted sudden cardiac death." Current Cardiology Reports
.
20
(4): 26. DOI: 10.1007/s11886-018-0963-1. PMID 29520510. - Yoo, Sang-young; Kim, Chan-Young (2009). "Update on the mechanisms of vasospastic angina". Korean Journal of Circulation
.
39
(12): 505–11. DOI: 10.4070/kcj.2009.39.12.505. PMC 2801457. PMID 20049135. - Egashira, Kensk; Katsuda, Yusuke; Mohri, Masahiro; Kuga, Takeshi; Tagawa, Tatuya; Shimokawa, Hiroaki; Takeshita, Akira (1996). "Basal endothelial nitric oxide release at the site of spasm in patients with variant angina." Journal of the American College of Cardiology
.
27
(6):1444–9. DOI: 10.1016/0735-1097 (96) 00021-6. PMID 8626956. - Sun, Hongtao; Mohri, Masahiro; Shimokawa, Hiroaki; Usui, Makoto; Urakami, Lemmy; Takeshita, Akira (February 28, 2002). "Coronary microvascular spasm causes myocardial ischemia in patients with vasospastic angina." Journal of the American College of Cardiology
.
39
(5):847–851. DOI: 10.1016/S0735-1097(02)01690-X. PMID 11869851. - Yasue, Hirofumi; Toyama, Masato; Kato, Hirofumi; Tanaka, Satoru; Akiyama, Fumiya (February 1976). "Variant Prinzmetal's angina as a manifestation of alpha-adrenergic receptor-mediated coronary artery spasm: Documentation by coronary arteriography." American Heart Journal
.
91
(2):148–155. DOI: 10.1016/s0002-8703(76)80568-6. PMID 813507. - ^ abcd Hung MJ, Cherng WJ (January 2013). "Coronary vasospastic angina: current understanding and role of inflammation". Acta Cardiologica Sinica
.
29
(1): 1–10. PMC 4804955. PMID 27122679. - ^ abc Thadani U (August 2014). "Problems with Nitrate Therapy and Nitrate Tolerance: Prevalence, Prevention, and Clinical Implications." American Journal of Cardiovascular Drugs: Drugs, Devices, and Other Interventions
.
14
(4):287–301. DOI: 10.1007/s40256-014-0072-5. PMID 24664980. - "NORVASC-amlodipine besylate tablet". DailyMed
. 2019-03-14. Retrieved December 19, 2021. Vasospastic Angina: NORVASC has been demonstrated to block constriction and restore blood flow in coronary arteries and arterioles in response to calcium, epinephrine potassium, serotonin and thromboxane A2 analogue in animal models and in human coronary vessels in vitro. This suppression of coronary spasm is responsible for the effectiveness of NORVASC in vasospastic angina (Prinzmetal's angina or its variant). - ↑
Takagi Y, Takahashi J, Yasuda S, Miyata S, Tsunoda R, Ogata Y, Seki A, Sumiyoshi T, Matsui M, Goto T, Tanabe Y, Sueda S, Sato T, Ogawa S, Kubo N, Momomura S, Ogawa H, Shimokawa H (September 2013).
"Prognostic stratification of patients with vasospastic angina: a comprehensive clinical risk assessment developed by the Japanese Coronary Spasm Association". Journal of the American College of Cardiology
.
62
(13): 1144–53. DOI: 10.1016/j.jacc.2013.07.018. PMID 23916938.