Pulmonologist
Prokhina
Maria Egorovna
Experience 38 years
Pulmonologist
Make an appointment
Pulmonary edema is a pathological, very serious condition, which is characterized by the release of transudate into the lung tissue. As a result, gas exchange is disrupted, which leads to serious consequences, including death.
Emergency care for pulmonary edema is the only thing that can increase the patient’s risks of survival and recovery. A person in such a situation requires immediate medical attention.
Pulmonary edema itself is most often a complication that accompanies serious problems of organs and body systems, for example, the cardiovascular system, gastrointestinal tract, etc.
Causes
In fact, there are many causes of pulmonary edema - they are different for different diseases. Let us name, for example, a few general prerequisites:
- cardiosclerosis after a heart attack, acute myocardial infarction;
- hypertension, arrhythmia;
- heart failure;
- congenital or acquired heart defects;
- chronic bronchitis, lobar pneumonia, bronchial asthma;
- complications due to ARVI, measles, influenza, scarlet fever, whooping cough and other diseases;
- prematurity in newborns;
- serious kidney problems;
- traumatic brain injury, brain surgery, etc.;
- inhalation of toxic substances.
These and many other reasons are not direct factors contributing to the development of pulmonary edema. But against the background of such conditions, it can develop, which is necessarily taken into account during hospitalization with all of the above.
Dressler syndrome
This complication develops 2-6 weeks after myocardial infarction due to necrotic damage to the tissue of the heart muscle. Toxic decomposition products entering the patient’s blood cause an autoimmune reaction in the body. Dressler syndrome is characterized by the following symptoms:
- Sharp or pressing pain in the chest, often radiating to the shoulder or neck.
- Sometimes there is an increase in background temperature.
- The patient complains of severe weakness.
- Painful sensations may appear in the area where the lungs are located.
- A dry cough with blood may occur.
- Rashes appear on the skin.
- There is numbness in the left hand.
- Upon visual examination, the left side of the chest appears swollen.
Dressler's syndrome can occur as pleurisy, pericarditis or polyarthritis. This is a typical variant for this condition. The atypical form is expressed as cardiobrachial syndrome, which is indicated by high temperature and changes in blood tests.
Varieties
There are different types of pulmonary edema:
- fulminant. It develops extremely quickly, in a few minutes - the outcome in this case is only fatal;
- spicy. Symptoms increase over four hours and the risk of death is very high. Such swelling often occurs with heart attack, suffocation, and traumatic brain injury;
- subacute. The development of symptoms alternates between active and quieter stages. Occurs in liver failure;
- protracted. It can develop within twelve hours, even several days, and not have a clear manifestation. It manifests itself in heart failure, as well as chronic lung diseases.
Obviously, each option requires different actions. If the patient can still be saved, speed of response will be a key factor.
Reasons why infarction pneumonia develops
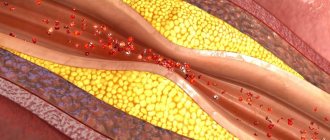
The following conditions are identified that provoke the development of blood clots:
- phlebeurysm;
- right ventricular heart failure;
- heart defects;
- rupture of a blood clot or inflammation of a vein.
In the presence of concomitant factors that aggravate the course of the underlying disease, the risk of developing infarction pneumonia increases significantly. These factors are:
- venous insufficiency in chronic form;
- overweight;
- taking estrogen;
- weakening of muscles;
- systemic diseases.
But even with such conditions, thrombophlebitis does not occur in every patient. There are several reasons leading to this condition:
- fracture of a tubular bone;
- atrial fibrillation;
- long periods of lying down, for example, when the patient is in a coma;
- poor blood circulation.
Ultimately, the combination of the above factors leads to the separation of small parts of blood clots, which subsequently settle in the vessels of the lungs, which subsequently leads to blockage of the artery. Impaired blood circulation in the lung due to narrowing of the artery leads to pulmonary infarction.
At the site of the infarction, there may be a complete lack of blood flow. When such an area becomes infected with various bacteria and microorganisms, infarction pneumonia is observed.
Symptoms
It is possible to describe the symptoms of pulmonary edema only in general terms, since certain types of pathology occur with blurred characteristics. Signs include the following:
- severe weakness;
- shallow, very rapid breathing;
- dry cough;
- dry wheezing;
- severe shortness of breath;
- puffiness of the face and neck;
- bubbling breathing and moist wheezing;
- foam at the mouth with a pink tint;
- lethargy, confusion;
- shallow breathing;
- thready pulse.
Some signs of pulmonary edema contradict each other for the reason that everything can start with one condition and end with another. For example, rapid breathing occurs for several minutes or hours, and then it weakens. In the fastest and most dangerous forms of edema, the patient's death occurs from suffocation (asphyxia).
Are you experiencing symptoms of pulmonary edema?
Only a doctor can accurately diagnose the disease. Don't delay your consultation - call
Diagnostics
If the symptoms of pulmonary edema are not pronounced, additional studies are required in parallel with emergency care:
- biochemical screening. This is a blood test;
- study of blood gases;
- ECG, ultrasound of the heart;
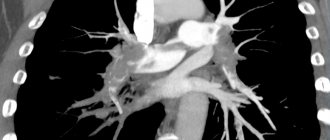
- X-ray of the chest area;
- pulmonary artery catheterization.
In many cases, diagnosis of pulmonary edema is possible immediately - only based on the signs that appear visually in the patient and without additional examination.
Treatment
There is not and cannot be a single program for the treatment of pulmonary edema. Emergency care for a patient includes measures to reduce venous return to the heart and supply humidified oxygen. Often the patient is transferred to mechanical ventilation, and a tracheostomy may be performed.
Various drugs are also additionally administered: analgesics, diuretics, drugs that reduce pressure in the pulmonary circulation, drugs for the heart, antibacterial agents and much more. Further, treatment of pulmonary edema, if the attack is removed, comes down to treating the underlying disease that caused this pathology.
The prognosis for edema is very serious. Depending on the causes of pulmonary edema, mortality can range from 20 to 90%. The sooner the problem is identified, the higher the chances of recovery. But in many cases, the patient can only be saved by timely treatment of those diseases that contribute to the occurrence of pathology - such prevention of pulmonary edema, for example, is the only way to reduce the risks of the fulminant form of the disease, which in itself is already fatal and cannot be treated.
Noninvasive ventilation for acute myocardial infarction
Acute heart failure (AHF) during myocardial infarction (MI) is the inability of the heart, as a pump, to pump the required volume of blood (cardiac minute volume (MCV) l/min), adequate to the metabolic needs of the body (providing basal metabolism), which is manifested by severe hemodynamic disorders and impaired gas exchange function of the lung. Failure of the pumping ability of the heart, due to ischemic damage to the left ventricular myocardium, leads to the development of hypoxemia - an early and permanent sign of circulatory failure, which underlies the clinical signs of AHF. The basis of the hypoxemic syndrome, by the mechanism of reducing blood oxygen saturation, involves two components of hypoxemia - central (cardiogenic - stagnation of blood in the lung) and peripheral (circulatory - slowdown of peripheral tissue blood flow).
Depending on the severity of clinical manifestations, according to the proposed classification by T. Killip, J. Kimball, there are 4 degrees of AHF in MI:
I degree - absence of clinical manifestations of heart failure;
II degree - wheezing in the lungs during auscultation, heard in an area of less than 50% of the pulmonary fields, or the presence of tachycardia in combination with III sound during auscultation of the heart - systolic ri;
III degree - wheezing in the lungs on auscultation of more than 50% of the lung fields in combination with rhinitis;
IV degree - pulmonary edema, clinical picture of cardiogenic shock [1].
Standard drug therapy (SMT) for acute myocardial infarction (AMI) complicated by AHF is quite well developed and regulated. The in-hospital mortality rate of MI complicated by AHF is 24%; in severe cases, with the need for artificial pulmonary ventilation (ALV) using tracheal intubation, according to domestic and foreign authors, it reaches 52% [2, 3, 4, 6, 7, 8, 9, 12].
Recent fundamental works, including a meta-analysis of a large number of studies of AHF, have shown the high effectiveness of the main methods of non-invasive (mask) artificial pulmonary ventilation (NIV) in the treatment of cardiogenic pulmonary edema (CPE), refractory to CMT: continuous positive airway pressure (CPAP - Continuous). Positive Airway Pressure), support with increased pressure during inspiration (PSV - Pressure Support Ventilation), support with increased pressure at the end of expiration (PEEP - Positive End-Expiratory Pressure) [13, 15, 19].
The British Thoracic Society guidelines recommend the use of CPAP in patients with persistent hypoxemia during complex medical treatment of AHF and reserving the use of two-level ventilation - PSV + PEEP for patients in whom CPAP does not improve [5].
Currently, the medical literature contains isolated reports on the use of NIV in the treatment of COL in patients with AMI [16, 17, 18]. These publications documented that the combination of inspiratory support with positive end-expiratory airway pressure (PSV + PEEP) was more effective in reducing work of breathing and respiratory distress than CPAP alone [10, 11, 14].
All of the above was the purpose of this work - to study the effectiveness of various methods of NIV in patients with AMI complicated by grade III-IV AHF, refractory to standard drug therapy.
Materials and methods. The study group included 94 patients with AMI, whose average age was 67.4 ± 5.5 years. Inclusion criteria were: large-focal AMI complicated by grade III–IV AHF according to the Killip–Kimball classification, respiratory failure and peripheral hypoxemia (resting respiratory rate (RR) > 25/min, H2O2 — transcutaneous < 90%), persisting for 1 hours against the background of ongoing SMT.
SMT included: oxygen through nasal cannulas or face mask, antiplatelet agents and anticoagulants, loop diuretics, nitroglycerin, ACE inhibitors, beta blockers; Patients with grade IV AHF were additionally prescribed catecholamines.
In order to objectify the effectiveness of the treatment, all patients underwent sounding of the right parts of the heart with measurement of mean pressure in the right atrium (RA), systolic and diastolic pressure in the right ventricle (SDP, DPPV), systolic and diastolic pressure in the pulmonary artery (SDPA, DPPA) , pulmonary artery wedge pressure (PAWP), with calculation of cardiac (CI) and shock indices (SI), left and right ventricular shock index (LVSI, IURP), total peripheral vascular resistance (TPVR), total pulmonary resistance (TPR). Before and after 60 minutes of NIV, blood samples were taken from the pulmonary and peripheral arteries to determine the acid-base state of the blood (ABC), hemoglobin concentration (Hb), oxygen and carbon dioxide tension (pO2, pCO2), oxygen saturation of Hb (HbO2) and calculation of the oxygen delivery index (IDO2), oxygen consumption index (IPO2), percentage of blood shunting in the lungs (Qs/Qt). NIV was performed on an RV-7200 device (USA) with atmospheric air (FiO2 - 21%) in three modes: CPAP, PSV and PSV + PEEP. In 85% of cases a face mask was used, and in 15% a nasal mask was used.
Depending on the NIV regimen, patients with AMI complicated by AHF were divided into three groups: group A-1 mask CPAP - 19 patients (11 men, 8 women), average age in the group - 59.7 ± 10.8 years; group A-2 with PSV ventilation mode - 27 patients (24 men and 3 women), average age was 68.3 ± 10.9 years; group A-3 combined ventilation mode PSV + PEEP - 48 patients (34 men and 14 women), average age in the group - 60.7 ± 12.5 years. By age, patients in groups A-1, A-2 and A-3 were comparable and did not differ statistically from each other (p > 0.05).
In group A-1, the course of AMI was complicated by grade III AHF in 15 patients, grade IV AHF in 4. In group A-2, grade III AHF was recorded in 22 patients, grade IV HF in 5. In group A-3, grade III AHF was observed in 38 patients, stage IV HF in 10. With PSV artificial ventilation mode, the inspiratory pressure averaged 17.0 ± 5.9 cmH2O; with PEEP, expiratory pressure averaged 5.4 ± 1.4 cmH2O; average inspiratory pressure PSV + PEEP - 17.6 cmH2O.
The doses and rate of administration of SMT drugs in all patients before and during NIV were almost the same (p > 0.05). When comparing the initial parameters of hemodynamics and gas exchange between groups A-1, A-2 and A-3, no significant differences were noted (p > 0.05).
Statistical processing was carried out using the statistical analysis application package Statistica v.6.0; parametric and nonparametric reliability criteria were used.
Treatment results and their discussion. The dynamics of central hemodynamics and blood gas composition in AMI patients with AHF under the influence of various modes of auxiliary ventilation during spontaneous breathing (groups A-1, A-II, A-III) are presented in
,
,
.
Respiratory support in the CPAP mode from 5.0 to 13 cm H2O led to clinical improvement in 93% of patients, which was expressed in a decrease in patient agitation, a decrease in tachycardia and shortness of breath, and an improvement in peripheral circulation (a positive change in the color, temperature and humidity of the skin) , at the same time, moist congestive rales in the lungs significantly decreased or completely disappeared. Positive clinical dynamics were accompanied by a statistically significant decrease in preload (PPWP mmHg) by 25% and afterload (TPPL) by 13.5% for the left ventricle against the background of a decrease in heart rate (HR) by 10.3% and an increase in pumping function left ventricle (LVRI) by 8.3%, a decrease in the right ventricular performance index by 13.3%.
A decrease in PAWP indirectly indicated unloading of the pulmonary circulation, which led to significant positive changes in gas exchange indicators: an increase in arterial blood oxygenation (HbO2a, %) by 5.6% and mixed venous blood (HbO2a, %) by 11.2% with a statistically significant decrease shunting blood in the lungs by 43%. A decrease in the percentage of blood shunting in the lungs, with an improvement in arterial blood oxygenation, was accompanied by a significant increase in oxygen delivery to the executive organs and tissues: IDO2 increased by 6% (p < 0.0005) with a significant decrease in IPO2 by 12.2% (p < 0. 01), which is associated with a decrease in the work of the respiratory muscles against the background of a decrease in respiratory rate by 23.1%.
Thus, total respiratory support in the form of CPAP with an average pressure of 9.0 ± 0.3 cm water column led to a significant decrease in respiratory rate, heart rate, hydrostatic pulmonary capillary pressure, blood shunting in the lungs, afterload for the left ventricle and was accompanied by an increase in oxygenation of the arterial and venous blood, shock index and oxygen delivery to executive organs and tissues.
Respiratory support with PSV also resulted in rapid clinical improvement and patient stabilization in 91% of cases. Hemodynamic and gas exchange data are presented in.
Inspiratory pressure support led to a significant decrease in hydrostatic pressure in the pulmonary capillary (PCP), systolic pressure in the pulmonary artery and right ventricle by 19.2%, 20% and 25%, respectively, which was accompanied by a decrease in the work of the right ventricle by 16.2% and restoration of the efficiency of the left ventricle of the heart by 17.5%. In total, these changes contributed to a significant decrease in heart rate by 7.4%.
Respiratory pressure support during inspiration in patients of group A-2 led to an effective improvement in gas exchange rates: a decrease in blood shunting in the lungs by 35.1%, restoration of the oxygenating function of the lung - an increase in the oxygen content in arterial blood by 4.5%, an increase in oxygen delivery by 12.9% and a decrease in the O2 consumption index by 7.2%. A statistically significant decrease in heart rate by 13.3% indirectly indicates an improvement in the gas exchange function of the lung, confirmed by a decrease in PCO2 in arterial blood by 5.6%. In turn, a decrease in respiratory rate helps to reduce energy consumption for the work of the respiratory muscles, leading to a decrease in IPO2.
Respiratory support in the PSV + PEEP mode in patients of group A-3 also led to rapid clinical improvement and stabilization of the condition in 92% of observation cases. Positive clinical dynamics were confirmed by objective data presented in.
The table shows that NIV in the PSV + PEEP mode was accompanied by a significant decrease in heart rate by 14.2%, a decrease in hydrostatic pulmonary capillary pressure by 26%, with an increase in left ventricular performance by 14.4%, and an increase in pressure in the right atrium by 83 .3%. The increase in pressure in the right atrium (an indicator of central venous pressure) is due to an increase in intrathoracic pressure due to increased pressure during inhalation and exhalation of the NIV respiratory cycle (on average by 17.6 cm H2O), which is accompanied by an increase in resistance to blood flow to the right ventricle. Indicators of blood pressure, resistance of the systemic and pulmonary circulation, pressure and work of the right ventricle did not change significantly.
It follows from the table that NIV in the PSV + PEEP mode led to a rapid decrease in shortness of breath (RR decreased by 30%), an improvement in the oxygenation of arterial and mixed venous blood by 6% and 9.8%, respectively, and a decrease in the degree of shunting of venous blood in the lungs by 31.8% and an increase in oxygen delivery to executive organs and tissues by 4%. Improvement in gas exchange function of the lung is documented by a decrease in pCO2 in arterial blood by 7.8%.
In a retrospective analysis (for one year) of medical records of patients with AMI complicated by AHF, who underwent standard artificial ventilation using tracheal intubation, hospital mortality was 39.6%. In our studies, in the overall group of patients with AMI complicated by AHF who received NIV in various modes, hospital mortality was 25.5% (24 patients).
Conclusion
With myocardial infarction, there is a violation of the contractile state of the heart muscle, leading to a decrease in the pumping activity of the heart and, as a consequence, to an increase in end-diastolic pressure, in particular in the cavity of the left ventricle. A physiologically significant increase in left ventricular end-diastolic pressure or left atrial pressure invariably leads to a retrograde increase in pressure in the pulmonary vessels and forms post-capillary, passive pulmonary hypertension. In accordance with the Starling equation, with an increase in hydrostatic pressure in the pulmonary circulation, the rate of fluid filtration through the microvascular endothelium in the pulmonary interstitium increases. When fluid is filtered faster than it is removed by the lymphatic system, perivascular, interstitial, and then alveolar pulmonary edema develops.
At the first stage of compensation, with an increase in interstitial pressure, J-receptors are stimulated with an increase in the volume of ventilation, which helps to increase lymph outflow and, as a result, minimizes the risk of progressive interstitial edema and subsequent alveolar flooding.
From a mechanical point of view, fluid retention in the pulmonary circulation can be represented as restrictive disorders, manifested by changes in lung volumes, a decrease in the elastic properties of lung tissue due to edema of the interstitium, flooding of the alveoli - functional units, which overall leads to a decrease in the gas exchange function of the lung.
The hemodynamic factor - an increase in pressure in the venous bed of the pulmonary circulation during AMI - is accompanied by heterogeneous disorders of lung ventilation, which are restrictive (decreased elasticity of the lung tissue) and obstructive (increased airway resistance due to swelling and bronchospasm) in nature.
A progressive decrease in lung capacity and its distensibility lead to an increase in negative pressure in the pleural cavity necessary for inhalation; consequently, to an increase in the “work of breathing”, increasing the proportion of the cardiac output required to provide energy for the mechanics of breathing.
All of the above changes lead to disturbances in the ventilation-perfusion ratios underlying cardiogenic-respiratory hypoxemia, which are aggravated by the appearance of additional intrapulmonary blood flow shunts, reaching more than 10% of the MVR in volume.
In patients with AMI complicated by acute left ventricular failure, the “work of breathing” is increased due to decreased compliance of the lung tissue and increased airway resistance (interstitial and bronchial edema); energy costs for the work of breathing in conditions of reduced CI reach 30% of cardiac output. Consequently, by reducing the energy costs of breathing using NIV, it is possible to reduce the proportion of SI directed to the respiratory muscles, redistributing it to other parts of the cardiovascular system.
NIV during spontaneous breathing of a patient with high blood pressure in various modes (CPAP, PSV PEEP), in addition to reducing the work of breathing, helps to “squeeze” the liquid part of the blood from the alveoli and interstitium of the lung tissue into the bloodstream, which ensures more efficient gas exchange and neutralizes the negative effect of the shunt in the lung.
Thus, respiratory support in various modes - CPAP, PSV and PSV + PEEP - turned out to be an effective method of treating COL, refractory to standard drug therapy, in patients with AMI. Against the background of NIV, clinical improvement and positive changes in parameters not only of hemodynamics, but also of gas exchange were observed. The effectiveness of various NIV techniques and the nature of their impact on indicators such as respiratory rate, heart rate, PP, MPAP, PAWP, IDO2, pO2a, pO2la and Qs/Qt turned out to be similar. A difference was noted when using PSV and PSV + PEEP in the degree of influence on the growth of LVRI and a decrease in CO2 tension in arterial blood.
It can be assumed that respiratory support regimens using PSV and PSV + PEEP will be more effective in patients with AMI complicated by AHF with concomitant hypoventilation and hypercapnia.
Although both PSV and CPAP demonstrate similar efficacy, from a practical point of view, CPAP is cheaper and more accessible in clinical practice, so CPAP may be considered the preferred method in patients suffering from AMI with cardiogenic pulmonary edema.
For questions regarding literature, please contact the editor.
A. M. Shilov , Doctor of Medical Sciences, Professor S. P. Grachev , Candidate of Medical Sciences, Associate Professor of MMA named after. I. M. Sechenova , Moscow
Questions and answers
What causes pulmonary edema?
There are dozens of factors that contribute to the development of this pathology. They are associated with other diseases of different body systems. Clinical recommendations for pulmonary edema are largely determined by the situation.
Can pulmonary edema lead to death?
Yes, the risk of death in the case of such a pathology is very high, and for the fulminant form it is the only possible outcome of events. This is an extremely dangerous condition that requires immediate professional help.
How to treat pulmonary edema?
This is done exclusively in medical institutions, most often in intensive care. Only doctors know everything you need to know about the symptoms and treatment of pulmonary edema in adults or children - the pathology cannot be eliminated without special knowledge and skills.
What are the features of pulmonary edema in children?
Unlike adults, this pathology occurs much less frequently in children due to other diseases. The underlying cause is usually allergies or exposure to toxins. Or the cause may be congenital anomalies of various body systems.
Post-infarction angina
Attacks of heart pain most often occur in the first day and for 14 days after a heart attack. Statistics show that almost every fourth patient experiences such attacks after a heart attack. They are expressed in severe pain in the chest. Painful sensations can spread to the scapular region, lower jaw, and left arm.
Sometimes the pain is so severe that it can only be relieved with the help of medications. An attack of angina pectoris can be triggered by even the slightest physical activity, and the development of such symptoms at rest cannot be ruled out. As the patient's condition worsens, an increase or decrease in blood pressure is observed. In rare cases, the attack is not accompanied by pain, but then there is a disturbance in the heart rhythm. Post-infarction angina is dangerous because an attack can provoke a recurrence of myocardial infarction.