The intestines, like all organs, require nutrition to ensure their smooth functioning. Not only the cells of the inner layer, but also the “residing” microorganisms need the supply of protein, vitamins, energy and plastic materials. In an adult, they weigh up to two kg.
Intestinal ischemia develops by analogy with changes in the coronary vessels of the heart, often simultaneously. It is not for nothing that it is called “abdominal toad” (angina pectoris - “angina pectoris”). Its result is a violation of the patency of the intestinal arteries with the subsequent formation of necrotic areas in the intestine.
Ischemic intestinal disease is a difficult disease to diagnose. Until now, it is impossible to provide accurate information about the prevalence among the population, since the pathology often occurs under other masks.
What arteries does the intestinal blood supply depend on?
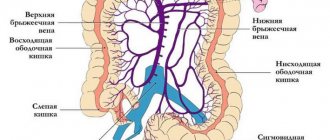
Blood supply in the abdominal cavity depends on three main arterial trunks:
- celiac artery,
- inferior and superior mesenteric (mesenteric).
They “take over” 40% of the body’s total blood flow. Between the vessels there is an extensive network of auxiliary collateral branches, which take on a compensatory role when blood flow through the main arteries is impaired.
The celiac trunk feeds the initial section of the intestine and all the organs of the gastrointestinal tract lying in the upper floor of the abdominal cavity. It extends directly from the abdominal aorta in the area of the diaphragmatic opening of the esophagus, and is only 2 cm in length. The place is known as one of the “favorite” localizations of atherosclerotic plaques.
Both mesenteric arteries branch into numerous branches and form a network of auxiliary vessels
The mesenteric arteries also arise from the abdominal aorta, but below the celiac trunk. The superior mesenteric artery supplies:
- small intestine (except duodenum);
- blind;
- ascending;
- ½ transverse colon.
From the inferior artery, blood flow is directed to:
- left half of the transverse colon;
- descending;
- sigmoid;
- rectum.
How does the peculiarity of the blood supply affect the risk of ischemia in the arterial area?
The location of the inferior celiac artery and a well-developed network of anastomoses between the branches make it less vulnerable to stenosis processes. Therefore, ischemia of the intestine located in the left half of the abdomen occurs quite rarely. This requires concomitant diseases with damage to the superior artery, collaterals or abdominal aorta.
The celiac trunk and superior mesenteric artery arise at right angles. This promotes thrombus formation, sedimentation of emboli, and microorganisms.
Surgeons noted the following patterns:
- Thrombosis and embolism are more common in the area of the superior mesenteric artery, and there are more opportunities for the development of inflammation (arteritis). Anatomically, separate sections of the intestine are identified between the branches of the outgoing small arteries, which represent the most likely areas of necrosis.
- Atherosclerosis often develops in the lower artery.
- The patency of the celiac trunk is more dependent on the anatomical features of the vessel.
The stages of development of intestinal ischemia are sequentially formed at a higher (acute process) or lower speed (chronic form). Morphological changes in tissues made it possible to identify:
- ischemia - the lack of blood flow into the intestinal walls is compensated by collateral vessels, metabolic processes in cells slow down, epithelial degeneration occurs, the production of enzymes and the breakdown of biochemical substances ceases, peristalsis is impaired (the function of promoting and removing waste);
- infarction - irreversible tissue necrosis (gangrene) in the intestinal area with disruption of the activity of the entire intestine;
- peritonitis - the addition of inflammation, thinning and rupture of the necrotic area with the release of contents into the abdominal cavity, a severe form of general damage to the body.
Risk factors
Common provoking factors for the development of intestinal ischemia are:
- diabetes mellitus, hypercholesterolemia syndrome, high blood pressure, smoking, old age, which cause atherosclerosis;
- strong pressure deviations below/above normal;
- cardiac dysfunctions such as arrhythmia, chronic failure;
- drug abuse;
- clotting factor impairment in antiphospholipid syndrome, hereditary hemoglobinopathy.
Why does ischemia occur?
The causes determine the type of ischemia. It is more convenient to divide them into:
- Extravascular (extravasal) - usually this is external pressure on the arteries from the falciform ligament of the diaphragm, enlarged nerve ganglia, tumors located in the area of the arteries. There may be anomalies in the location and origin of blood vessels, kinks, and increased tortuosity.
- Intravascular (intravasal) - depend on atherosclerotic deposits from the inside, obstructing blood flow, or pronounced aorto-arteritis of an inflammatory nature with the accumulation of immune cells, proliferation of the inner membrane, impeding the passage of blood.
A computed tomogram revealed adhesive obstruction as the cause of small intestinal ischemia
Another option classifies intestinal ischemia into the following types.
Occlusive, associated with blocking of the vascular trunk by a thrombus, embolus, inflammatory changes. The main reasons are varied:
- heart defects that form a pathological communication between the atria and ventricles, through which blood clots from the veins of the lower extremities enter the left ventricle, aorta and mesenteric vessels;
- atrial fibrillation - promotes the separation of parietal intracardiac thrombi;
- congestive heart failure;
- pronounced vascular atherosclerosis.
Non-occlusive - independent of the condition of the arteries, occurs in 50% of cases. More often than not, the exact cause cannot be determined. Development is promoted by:
- Heart arythmy;
- low blood pressure in case of shock, fainting;
- irrational use of antihypertensive drugs that cause a sharp decrease in blood pressure;
- dehydration of the body;
- development of heart failure.
Depending on the underlying cause, intestinal ischemia can develop acutely (thromboembolism, shock) or take a chronic form (atherosclerosis, aortoarteritis).
Symptoms
Depending on the nature of the course, the symptom complex manifests itself in different ways. For example, the acute form appears suddenly, develops quickly and is characterized by pronounced symptoms. The chronic form is characterized by gradual development. The first sign of ischemia is a sharp, sharp pain located in the umbilical region and the upper right quadrant of the abdomen. If the back wall suffers from a lack of oxygen, this provokes violent peristalsis and a false urge to defecate. Early stages are characterized by the presence of:
- severe nausea;
- profuse vomiting;
- severe diarrhea with blood in the stool.
In acute manifestations, an infarction of the intestinal mucosa immediately occurs, then other symptoms develop. Already in the first hour the following clinical picture appears:
- wave-like, severe pain attacks after eating, lasting up to 2 hours, which go away on their own and reappear after a meal (feelings similar to appendicitis);
- sudden loss of body weight;
- refusal to eat;
- dyspeptic disorders;
- rise in temperature;
- disappearance of peristalsis.
At the same time, signs of severe intoxication of the body and peritonitis may develop.
Factors contributing to the development of intestinal ischemia
Risk factors that provoke the development of the disease may be:
- age period over fifty years;
- hypertension, causing pathology of the heart and blood vessels;
- diabetes;
- nicotine poisoning, which affects arterial tone, when smoking;
- increased levels of low-density lipids in the blood, which contribute to atherosclerosis;
- obesity;
- the presence of vascular pathology in the form of coronary, cerebral insufficiency, atherosclerosis of the vessels of the extremities;
- diaphragmatic hernia;
- previous abdominal surgeries;
- blood diseases, vasculitis with increased coagulability;
- long bed rest;
- women taking hormonal contraceptives.
Causes
There are two large groups of ischemia that occur for specific reasons:
- Occlusive ischemic disease. The pathology is provoked by thrombosis of the veins and venous channels, thrombosis, embolism of the mesenteric arteries, when atypical bodies are present in the blood. Predisposing factors are:
- heart valve replacement surgery;
- heart defects;
- atrial tachyarrhythmia.
Thrombosis usually causes a reduction in the evacuation function of the heart and atherosclerosis. Blockage of the mesenteric veins is a rare phenomenon that occurs due to peritonitis, increased clotting factor, increased pressure in the portal vein, and inflammation of internal organs.
- Non-occlusive ischemic disease. Refers to frequent occurrences. Most likely reasons:
- abnormal heart rhythm (arrhythmia);
- arterial hypotension;
- cardiac dysfunction;
- taking a certain group of medications;
- dehydration.
There are also acute, caused by thrombosis, and chronic, caused by atherosclerosis, forms of ischemia.
Types of ischemia
In addition to acute and chronic forms, types of intestinal ischemia are distinguished depending on the severity of the compensatory function of auxiliary vessels. They may reflect the stage of the disease:
- compensation - mesenteric blood flow is not impaired due to the expansion of collateral arteries, intestinal function is not affected;
- subcompensation - blood circulation in the layers of the intestine is supported by the maximum efforts of collaterals, glandular and epithelial cells perform a minimum of their functions;
- decompensation - foci of necrosis form in place of normal cells, the function is impaired.
Clinicians distinguish the following forms:
- Ischemia of the colon - occurs against the background of a cancerous tumor, the diagnosis is made by colonoscopy, surgical removal of the tumor allows all symptoms to be relieved.
- Acute mesenteric ischemia - develops suddenly, treatment requires emergency surgery. The diagnosis is very difficult to make. Even taking into account all the signs from blood tests, ultrasound, and angiography does not show sufficiently reliable symptoms. The final diagnosis is made after opening the abdominal cavity on the operating table. This is where decisions about treatment options are made.
- Chronic mesenteric ischemia - since the disease develops gradually, there is enough time for examination and confirmation of the diagnosis. Often detected in patients with inflammation of the colon, which is regarded as ischemic colitis. Angiography of the peritoneal vessels makes it possible to clarify the nature of the disease.
- Ischemia associated with thrombus formation in the mesenteric vein - stagnation of blood below the thrombus leads to compression of the arterial trunks. Often observed in patients with increased blood clotting.
Clinical picture
Symptoms of intestinal ischemia depend on the form of the disease and the location of the affected branch of the vessel. Different types have their own preferential reasons. Therefore, the clinic is somewhat different.
Acute intestinal ischemia is characterized by:
- sudden development of sharp abdominal pain localized in the upper right and near the navel, quickly spreading throughout the entire abdomen;
- the urge to defecate due to increased intestinal motility;
- diarrhea, blood in stool;
- nausea with vomiting;
- temperature increase.
In the acute form, there is pain when touching the skin and palpation of the abdomen, but there are no peritoneal symptoms
Chronic ischemia occurs gradually, symptoms develop over years. The patient complains of:
- paroxysmal pain in the abdominal cavity, occurring half an hour after eating and lasting up to three hours (“abdominal toad”);
- the pain often does not have a specific localization or is bothersome around the navel, in the area of the large intestine (ischemic colitis);
- over several months the pain becomes more intense;
- at the beginning of the disease, the pain is relieved by antispasmodics, but over time the drugs do not alleviate the patient’s condition;
- you have to refuse food for fear of pain, so you lose weight;
- weight loss is also associated with malabsorption of nutrients;
- the stomach is almost constantly swollen, rumbling, pronounced noises are heard on auscultation;
- tendency to diarrhea followed by constipation;
- frequent nausea and vomiting.
Clinical features for different forms of ischemia
With ischemia of the colon, the symptoms appear moderately, complications are rare. Elderly people get sick more often. Symptoms are expressed in paroxysmal pain in the left half of the abdomen. The following factors take part in the development:
- atherosclerosis of mesenteric vessels;
- condition after surgery on the heart, blood vessels, abdominal organs, and gynecological diseases in women;
- injury in the abdominal area;
- general sepsis;
- artery thrombosis;
- hypotension;
- intestinal obstruction due to tumor, hernia, severe adhesions;
- spastic contraction of blood vessels during treatment with migraine drugs, hormonal agents;
- sports activities, especially running;
- the influence of chronic use of drugs such as cocaine and amphetamine.
A catheter from the femoral artery runs along the spine; a contrast agent injected into the abdominal aorta shows a “stump” of the mesenteric artery with its complete obstruction
Acute mesenteric ischemia most affects the small intestine. Her reasons:
- thromboembolism from the heart into the mesenteric vessels after heart surgery, attacks of paroxysmal fibrillation;
- may manifest itself during exacerbation of chronic ischemia in the vessels.
Ischemia due to a thrombus in the mesenteric veins occurs when:
- acute and chronic pancreatitis (inflammatory process in the pancreas);
- in case of any intestinal infection;
- liver cirrhosis;
- cancerous tumor in the digestive organs;
- intestinal diseases (ulcerative colitis, Crohn's disease);
- increased blood clotting, hormonal therapy;
- abdominal injuries.
Features of the postoperative period
After the operation, the patient is under the supervision of medical personnel for some time. The state of health and digestion processes are gradually normalized. In the early period after surgery, it is recommended to take medications and correct the condition after anesthesia.
If the patient has a stent installed, anticoagulant and antiplatelet drugs are indicated, which are necessary to prevent thrombus formation.
In order to evaluate the result of treatment, the attending physician conducts a study of the condition of the blood vessels and observes the patient over time. It is necessary to attend prescribed consultations and studies, as there is a risk of relapse of the pathology.
In order to receive treatment, you must consult a doctor. After the diagnostic methods have been carried out and an accurate diagnosis has been made, the doctor will, if necessary, set a date for intervention.
Diagnosis of the disease
For diagnosis, general blood and stool tests play a supporting role. Leukocytosis indicates ongoing inflammation. Increased coagulability indicates the possibility of blood clot formation. In a stool analysis, the mass of undigested food particles, blood cells, and elements of inflammation are determined.
Angiography involves injecting a contrast agent into the femoral artery through a long catheter to the abdominal aorta, followed by a series of images. The technique is very important for quickly making a diagnosis and deciding on treatment.
Magnetic resonance angiography allows for a layer-by-layer study of blood flow in the vessels.
Doppler study is carried out to assess the speed of blood flow and determine the specific location or area of the narrowed vessel, the location of the blood clot, and its size.
Colonoscopy - using a flexible endoscopic tube inserted into the rectum, the condition of the mucous membrane is studied and the extent of intestinal damage is revealed.
Esophagogastroduodenoscopy is performed with an endoscope to identify changes in the initial parts of the small intestine.
Laparoscopy - in an operating room, an endoscope is inserted into the abdominal cavity through a small incision to obtain visual information
Treatment methods
If intestinal ischemia is suspected, antibiotics must be prescribed to prevent infection and peritonitis, and drugs that dilate blood vessels.
Treatment of local inflammatory process of the intestine is provided.
If narrowing of the arterial beds is possible due to taking medications, then they are canceled.
When coagulability increases, antiplatelet agents and anticoagulants are prescribed to reduce thrombus formation.
If necrotic areas of the intestine are identified, they must be removed and the ends sutured. If this is not possible, a colostomy is formed with an opening on the skin of the abdomen. The patient will need to wear a colostomy bag.
At the same time, angioplasty of the narrowed artery is performed by inserting a balloon with a stent. Such an operation can be performed immediately after angiography.
For chronic ischemia, surgical treatment consists of creating an artificial vessel to bypass the thrombosed one.
If compression is caused by mechanical tumor growth, strangulation of a hernia, or adhesive obstruction, then the success of restoring arterial patency depends on the timely removal of these obstacles.
Operation
Several techniques are used:
- Bypass surgery to bypass the blocked area with removal of the necrotic part of the wall or thrombus. The shunt can be made in the form of a synthetic prosthesis or made from the patient's femoral vein.
- Angioplasty with bypass to widen the narrowed area.
- Transaortic endarterectomy with removal of atheromatous plaques through the abdominal cavity.
- Stenting with the installation of a stent (wire cylinder) at the site of narrowing, which prevents re-narrowing. The technique can be used as an adjunct to angioplasty.
After intestinal surgery, treatment is carried out with medications.
Possible consequences
The most common are:
- necrosis of the intestinal wall - occurs when there is insufficient compensatory forces, dead tissue undergoes rupture and the contents enter the abdominal cavity, this causes severe peritonitis;
- narrowing of the intestine - let’s assume that as a result of a chronic process, scar tissue appears in small areas as a result of healing; it fuses with other loops of the intestine, with the mesentery.
Scars form a new mechanical obstruction due to narrowing of the intestine
Mesenteric venous thrombosis
This condition develops against the background of blockage of a vein by a blood clot. The veins come from the intestinal tissues, therefore, when they are blocked, the blood does not find a way out of the organ. As a result, blood accumulates in the vessels, their walls thicken. Bleeding may occur in this area. Causes:
- infection of the peritoneum;
- severe abdominal injury;
- tumor formation in the gastrointestinal tract;
- certain types of hormonal treatments;
- intestinal inflammation such as Crohn's disease, diverticulitis, ulcerative colitis;
- pathologies that prevent the formation of blood clots.
Preventive measures
To take good care of your vessels you need to:
- stick to vegetable dishes, cereals in the menu, eat salads and fruits every day;
- limit the consumption of spicy meat products, fatty and fried meat and fish, legumes, smoked meats, canned food;
- stop smoking;
- fight low mobility, walk more, play sports;
- control and prevent chronic diseases.
Timely consultation with a doctor and examination will help prevent severe ischemia. Acute abdominal pain should not be treated independently under the pretext of food poisoning. If they have not occurred for the first time, or there are other consequences of arterial damage (myocardial infarction, stroke), then one should remember about systemic vascular damage and take measures to prevent complications.