Modern data on the mechanism of contraction of cardiac fibers and the conduction of nerve impulses along pathways are associated with the study of the electrophysiology of the heart. Understanding the role of these processes in the development of pathology helps to choose the right treatment for chronic heart failure, myocardial dystrophy, and cardiomyopathy.
Disruption of repolarization processes in the myocardium reveals the “secrets” of metabolic (metabolic) changes in the heart muscle, synthesis and conservation of energy reserves.
We will try to “translate” the scientific language of terms into an accessible interpretation of the biological properties of the cell.
Early ventricular repolarization syndrome - what is it? General information
Specific cardiac syndrome is found not only in patients with heart pathology, but also in absolutely healthy people. Early repolarization of the ventricles is called premature repolarization syndrome. Very often, WPW syndrome confused with premature repolarization, despite the fact that these are completely different pathologies.
Pathological changes on the ECG were considered normal for a long time, until a clear relationship with heart rhythm disturbances was revealed. The disease is asymptomatic, which greatly complicates timely diagnosis.
The syndrome of early (premature, accelerated) repolarization of the ventricles of the heart is characterized by specific changes in the electrocardiogram in the absence of obvious causes. ICD-10 code: I45.6
Phases
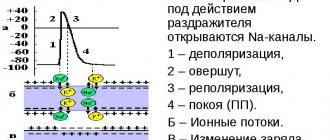
Five phases of development of PD can be clearly distinguished:
Rising (depolarization)
The occurrence of an action potential (AP) is associated with an increase in the permeability of the membrane for sodium ions (20 times compared to the permeability for K +, and 500 times compared to the initial permeability of Na +) and a subsequent increase in the diffusion of these ions along the concentration gradient into the cell, leads to a change (decrease) in membrane potential.
A decrease in membrane potential leads to an increase in membrane permeability to sodium by opening voltage-gated sodium channels, and an increase in permeability is accompanied by increased diffusion of sodium into the cytoplasm, which causes even more significant depolarization of the membrane. Due to the presence of positive feedback, depolarization of the membrane during excitation occurs with acceleration and the flow of sodium ions into the cell increases all the time. The intensity of the flow of potassium ions directed from the cell outwards in the first moments of excitation remains at the beginning. The increased flow of positively charged sodium ions into the cell first causes the disappearance of excess negative charge on the inner surface of the membrane, and then leads to recharging of the membrane. The influx of sodium ions occurs until the inner surface of the membrane acquires a positive charge sufficient to balance the sodium concentration gradient and stop its further passage into the cell. The sodium occurrence of PD is confirmed by experiments with changes in the external and internal concentrations of this ion. It was shown that a tenfold change in the concentration of sodium ions in the external or internal environment of the cell corresponds to a change in PD of 58 mV. When sodium ions were completely removed from the fluid surrounding the cell, PD did not occur. Thus, it has been established that AP occurs as a result of excess, compared to rest, diffusion of sodium ions from the surrounding fluid into the cell. The period during which the membrane permeability for sodium ions increases when sodium channels open is short (0.5-1 ms), followed by an increase in membrane permeability for potassium ions due to the opening of voltage-dependent potassium channels, and, consequently, increased diffusion these ions out of the cell. The “all or nothing” principle According to the “all-or-nothing” law, the cell membrane of an excitable tissue either does not respond to the stimulus at all, or responds with the maximum force possible for it at the moment. The action of the stimulus usually leads to local depolarization of the membrane. This causes the opening of sodium channels, which are sensitive to changes in potential, and through this increases sodium conductance, which leads to even greater depolarization. The existence of such feedback ensures regenerative (renewable) depolarization of the cell membrane. The magnitude of the action potential depends on the strength of the stimulus, and it occurs only when depolarization exceeds a certain limiting level specific for each cell. This phenomenon is called “all or nothing.” However, if depolarization is 50-75% of the limiting value, then a local response may occur in the cell, the amplitude of which is significantly lower than the amplitude of the action potential. The absence of an action potential at the pidboundary level of depolarization is explained by the fact that sodium permeability does not increase sufficiently to cause regenerative depolarization. The level of depolarization that occurs does not cause the opening of new sodium channels, so sodium conductance quickly decreases, and the resting potential in the cell is again established.
Overshoot
Depolarization of the membrane leads to a reversal of the membrane potential (the MP becomes positive).
In the overshoot phase, the Na + current begins to rapidly decrease, which is associated with the inactivation of voltage-dependent Na + channels (the open state time is milliseconds) and the disappearance of the electrochemical Na + gradient. Refractoriness One of the consequences of the disappearance of the Na + gradient is refractoriness - a temporary inability to respond to a stimulus. If the stimulus occurs immediately after the passage of the action potential, then excitability will not occur either with a stimulus strength at the threshold level or with a significantly stronger stimulus. This state of complete inexcitability is called the absolute refractory period. This is followed by a relative refractory period, when a suprathreshold stimulus can cause an action potential with a significantly lower amplitude than normal. An action potential of the usual amplitude under the action of a threshold stimulus can be evoked only after a few milliseconds after the preliminary action potential. The absolute refractory period limits the maximum frequency of generation of action potentials.
Repolarization
An increase in the potassium ion flow directed outward from the cell leads to a decrease in the membrane potential, which in turn causes a decrease in the permeability of the membrane to sodium ions, which, as indicated, is a function of the membrane potential. Thus, the second stage is characterized by the fact that the flow of potassium ions from the cell outward increases, and the counter flow of sodium ions decreases. This membrane repolarization continues until the resting potential is restored—membrane repolarization. After this, the permeability to potassium ions also drops to its original value. Due to the positively charged potassium ions released into the environment, the outer surface of the membrane again acquires a positive potential relative to the internal one.
Trace depolarization and hyperpolarization
In the final phase, the restoration of the resting membrane potential slows down, and trace reactions are recorded in the form of trace depolarization and hyperpolarization, due to the slow restoration of the initial permeability for K + ions.
Pathogenesis
Contraction of the chambers of the heart occurs as a result of changes in the electrical charge in myocardial cells - cardiomyocytes . As a result, sodium, calcium and potassium ions move into the intercellular space and back. The process is carried out in alternating main phases:
- depolarization – contraction;
- repolarization is relaxation before a new contraction.
Early repolarization of the ventricles is formed as a result of improper conduction of the impulse through the conduction system of the heart from the atria to the ventricles. To transmit the electrical impulse, abnormal conduction pathways . The development of the phenomenon is due to an imbalance between repolarization and depolarization in the basal regions and apex of the heart. Characterized by a significant reduction in the period of myocardial relaxation. On the ECG, along with the SRRS, a disturbance of repolarization processes in the myocardium is often recorded, in particular, a violation of the repolarization of the lower wall of the left ventricle.
Why does the heart contract?
The heart is “started” by an electrical impulse. It is formed from multiple electrical currents from the junction of heart cells.
Every living cell has its own negative electrical discharge inside. The difference between the external and internal voltage on the two sides of the cell membrane is 80-90 mV. This is the transmembrane potential. It does not change throughout life and is characteristic of each type of cell.
But cardiac cells are characterized by a change in potential due to the movement of ions (charged particles of sodium, potassium, calcium) through open tubules. Thanks to them, an electric current arises. It is also called the action potential.
Classification
In children and adults, early ventricular repolarization syndrome can have 2 development options:
- without damage to the cardiovascular system;
- with defeat.
According to the nature of the flow, they are distinguished:
- transitory form;
- permanent form.
Depending on the location of the ECG signs of SRGC, they are divided into 3 types.
- I characteristic signs are observed in a healthy person. ECG signs are recorded only in chest leads V1, V2. The likelihood of complications developing is extremely low.
- II ECG signs are recorded in the inferolateral and lower sections, leads V4-V6. The risk of complications is increased.
- III ECG changes are recorded in all leads. The risk of complications is the highest.
Causes
The true reasons have not been fully studied. There are only hypotheses for the occurrence of early repolarization:
- Genetic predisposition. Mutation of genes that are responsible for balancing the processes of the entry of certain ions into the cell and their release out.
- Disruption of the processes of contraction and relaxation of individual areas of the myocardium, which is characteristic of type I Brugada syndrome .
- Changes in cardiomyocyte action potentials. The process is associated with the mechanism for the release of potassium ions from cells. This also includes increased susceptibility to a heart attack during ischemia .
According to statistics, accelerated repolarization syndrome is typical for 3-10% of healthy people of all ages. Most often, changes are recorded in young people aged 30 years, in people leading a healthy lifestyle and in athletes.
Nonspecific factors influencing the development of early ventricular repolarization syndrome:
- congenital form of hyperlipidemia , which provokes the development of atherosclerotic changes ;
- long-term use of certain medications, or overdose (for example, beta-agonists);
- connective tissue dysplasia , which is characterized by additional chordae in the ventricular cavity;
- high blood cholesterol
- electrolyte imbalance;
- neuroendocrine changes;
- hypertrophic cardiomyopathy;
- heart defects : congenital, acquired;
- disturbances in the functioning of the autonomic nervous system;
- hypothermia of the body;
- excessive physical activity.
The structure of heart cells
Using electron microscopy, it became possible to study the structure of heart cells. Myofibrils—protein fibers of two types—were identified: thick fibrils turned out to be myosin, and thin ones turned out to be actin.
During the contraction process, thin fibers slide over thick ones, actin and myosin combine to form a new protein complex (actomyosin), muscle tissue shortens and tenses. When you relax, everything returns to normal. Between them there are bridges through which chemicals are transferred from one cell to another.
Symptoms
Clinical symptoms are observed only in the form of the disease that is accompanied by disturbances in the functioning of the cardiovascular system:
- loss of consciousness, fainting ;
- rhythm disturbances ( tachyarrhythmia , extrasystole , ventricular fibrillation );
- vagotonic, hyperamphotonic, tachycardial, dystrophic are formed under the influence of humoral factors on the hypothalamic-pituitary system;
- systolic and diastolic dysfunction of the heart caused by its hemodynamic disorders ( pulmonary edema , hypertensive crisis , shortness of breath , cardiogenic shock ).
Molecular mechanisms of action potential generation
The active properties of the membrane that ensure the occurrence of an action potential, based mainly on the behavior of voltage-gated sodium (Na +) and potassium (K +) channels. The initial phase of AP is formed by the input sodium current, later potassium channels open and the output K + -current returns the membrane potential to the initial level. The initial ion concentration is then restored by the sodium-potassium pump.
During the PD, channels pass from state to state: in Na + channels there are three main states - closed, open and inactivated (in reality everything is more complicated, but these three states are enough for description), in K + channels there are two - closed and open.
The behavior of the channels involved in the formation of PD is described in terms of conductivity and calculated through transfer coefficients.
Carryover coefficients were derived by Alan Lloyd Hodgkin and Andrew Huxley.
Conductivity for potassium GK per unit area
| , |
| Where: |
| an — Transfer coefficient from closed to open state for K+ channels [1/s]; |
| bn — Transfer coefficient from open to closed state for K+ channels [1/s]; |
| n — Fraction of K+ channels in the open state; |
| (1 - n) - Fraction of K + channels in the closed state |
The conductivity for sodium G Na per unit area
is more difficult to calculate, since, as already mentioned, in voltage-dependent Na + channels, in addition to the closed / open states, the transition between which is a parameter, there are also inactivated / not inactivated states, the transition between which is described through a parameter
| , | , |
| Where: | Where: |
| am — Transfer coefficient from closed to open state for Na + channels [1/s]; | ah — Transfer coefficient from inactivated to non-inactivated state for Na + channels [1/s]; |
| bm — Transfer coefficient from open to closed state for Na + channels [1 / s]; | bh — Transfer coefficient from non-inactivated to inactivated state for Na + channels [1 / s]; |
| m — Fraction of Na + channels in the open state; | h — Fraction of Na + channels in a non-inactivated state; |
| (1 - m) - Fraction of Na + channels in the closed state | (1 - h) - Fraction of Na + channels in the inactivated state. |
Tests and diagnostics
The main changes are recorded precisely on the electrocardiogram. Some patients simultaneously experience clinical symptoms of cardiovascular diseases, but most often patients feel absolutely healthy and do not notice any changes.
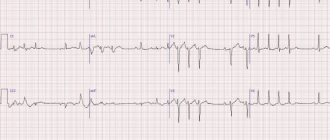
Early ventricular reoplarization syndrome on ECG:
- elevation of the ST segment above the isoline;
- the convexity when raising the ST segment is directed downwards;
- an increase in the R wave with a parallel decrease in the S wave or its complete disappearance;
- point J is located above the isoline, at the level of the descending knee of the R wave;
- expansion of the QRS complex on the ECG;
- a “notch” is recorded on the descending limb of the R wave.
Early ventricular repolarization syndrome in children
The reasons for the development of early repolarization syndrome in children can be very different:
- lack of sleep and irregular daily routine;
- excessive emotional stress;
- physical overload;
- constant anxiety, stress or nervous fatigue;
- isolation, lack of healthy emotional contact with parents;
- hypothermia;
- poor quality and unbalanced nutrition.
A similar syndrome can be recorded on an ECG in any child who reacts too emotionally to the assessment of his knowledge at school, takes current events to heart, and is overloaded in extracurricular activities. Lack of proper rest and intensive training in sports clubs can negatively affect the child’s well-being.
Story
The main provisions of the membrane theory of excitation were formulated by the German neurophysiologist Yu. Bernstein
In 1902, Julius Bernstein put forward a hypothesis according to which the cell membrane allows K+ ions into the cell, and they accumulate in the cytoplasm. The calculation of the resting potential value using the Nernst equation for the potassium electrode satisfactorily coincided with the measured potential between the muscle sarcoplasm and the environment, which was about -70 mV. According to the theory of Yu. Bernstein, when a cell is excited, its membrane is damaged, and K + ions leave the cell along a concentration gradient until the membrane potential becomes zero. The membrane then restores its integrity and the potential returns to the resting potential level.
This model was developed in their 1952 work by Alan Lloyd Hodgkin and Andrew Huxley, in which they described the electrical mechanisms responsible for the generation and transmission of a nerve signal in the squid giant axon. For this, the authors of the model received the Nobel Prize in Physiology or Medicine for 1963. The model is called the Hodgkin-Huxley model
In 2005, Thomas Heimburg and Andrew D. Jackson proposed the soliton model, based on the assumption that the signal propagates through neurons in the form of solitons - stable waves propagating along the cell membrane.
Forecast. What is the danger of early ventricular repolarization syndrome?
Modern cardiologists work to prevent and prevent the development of pathology, which can lead to death. That is why patients with early ventricular repolarization syndrome should be regularly monitored by a cardiologist to monitor the dynamics of the ECG and to identify hidden symptoms of other pathologies. It is not the syndrome itself that is dangerous, but the consequences it can lead to in the absence of proper treatment of the causative disease.
Persons who play sports are recommended to undergo examination at specialized physical education clinics, assessing their condition before and after intensive training, as well as before competitions.
There is no clear data on the transition of SRGC to a serious pathology. The risk of death increases significantly with alcoholism , abuse of fatty foods and smoking. A timely and complete competent examination will help to identify or exclude the true cause and avoid problems in the future.
Action potential propagation between cells
At a chemical synapse, after the action potential wave reaches the nerve terminal, it causes the release of neurotransmitters from the presynaptic vesicles into the synaptic cleft. Transmitter molecules released from the presynapse bind to receptors on the postsynaptic membrane, resulting in the opening of ion channels in the receptor macromolecules. Ions begin to enter the postsynaptic cell through open channels, change the charge of its membrane, which leads to partial depolarization of the membrane and, as a consequence, provoking the generation of an action potential in the postsynaptic cell.
In the electrical synapse there is no “mediator” of transmission in the form of a neurotransmitter. But the cells are connected to each other using specific protein tunnels - conexons, so ionic currents from the presynaptic cell can stimulate the postsynaptic cell, causing the generation of an action potential in it. Thanks to this structure, the action potential can propagate in both directions and much faster than through a chemical synapse.
- Scheme of the process of nerve signal transmission at a chemical synapse
- Diagram of the structure of an electrical synapse