The principle of defibrillation: how the rhythm is restored
Defibrillation is the most important step in cardiopulmonary resuscitation.
The principle of operation is based on stopping fast, ineffective contractions of the heart chambers by creating an electrical discharge. Rhythm restoration is carried out using a high-energy (200-360 J) electrical impulse, which passes through the human body in 0.01 s and breaks the “vicious circle”. Technical steps of defibrillation: 1. An electric current is passed between two electrodes, which are applied at the base and apex. The direction of the impulse corresponds to the normal passage of excitation through the conduction system of the organ. 2. The simultaneous energy flow stops the spontaneous contraction of individual fibers and “synchronizes” cardiomyocytes. 3. After a short pause, the normal heart rhythm is restored, which is set by the sinus node (“driver”). If the first procedure is ineffective, defibrillation can be repeated with greater intensity after 2 minutes (after assessing the condition and performing chest compressions). The number of impulses is not limited.
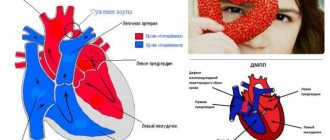
Ventricular fibrillation is a pathological condition that occurs when muscle tissue begins to contract chaotically and very quickly, up to 250-480 beats per minute. In such a rhythm, the ventricle is not able to adequately fill with blood and transfer it to the body. Without timely cessation of this process, the prognosis for survival is unfavorable.
Using a defibrillator in childhood
Ventricular tachycardia, pulseless ventricular fibrillation, is rare in children. However, if this happens, the same rescue measures apply as for adults.
The main difference between defibrillation in children is the choice of electrodes and the device itself, which is based on:
- Size. It is important that the elements cover the correct area of the sternum, but do not touch each other. If the baby weighs less than 10 kg, use pads.
- Device model and child's age. An automatic defibrillator should not be used on children under 8 years of age or weighing less than 25 kg because the defibrillator shock cannot be adjusted. The child's weight is important in determining the correct defibrillator setting. For every 1 kg, 2 J are measured. If there is no effect, the dose is doubled, to 4 J / kg.
Types of devices and their structure
A defibrillator is a medical device that generates powerful high-voltage electrical impulses.
Modern devices differ little from their predecessors, consisting of a capacitor, charging and discharge circuit with a pulse generation circuit - biphasic current. New models have a built-in electrocardiograph to assess the success of manipulations. Today there are the following types of devices (examples are shown in the photo):
Manual external defibrillator
Such a device requires professional skills. It is used in conjunction with a cardiograph, which, depending on the type of device, can be built-in or separate. The healthcare professional determines the heart rate and the shock needed.
Manual internal defibrillator
It is used in an operating room directly on an open heart. Has special “spoons” for applying a shock.
Automated external defibrillator (AED)
Designed specifically for inexperienced users or for non-medical personnel (police officers, firefighters, airport workers, train stations, stadiums and other public areas). The device independently detects the heart rhythm and chooses when defibrillation is required and when not.
Using an AED before specialized help arrives significantly increases the victim’s chances of survival. However, it does not replace the use of manual cardiopulmonary resuscitation (without artificial respiration).
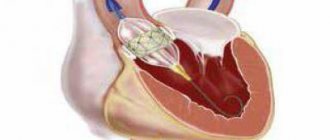
Implantable cardioverter defibrillator
This device is similar to a pacemaker (artificial pacemaker); some modern models can act as a pacemaker. The implant continuously monitors the patient's heartbeat and automatically delivers a small electrical shock (a process called cardioversion) if it detects a life-threatening arrhythmia. This does not cause discomfort and significantly prolongs life.
Portable cardioverter-defibrillator
The patient wears the cardioverter on a special belt. The device is necessary for those who are at the stage of preoperative preparation for implantation of a pacemaker. The discharges delivered by the device synchronize cardiac activity.
Carrying out the procedure
Emergency electrical stimulation consists of the following stages:
- The patient should be in a horizontal position on a flat surface.
- Remove excess clothing to leave your chest free.
- The electrodes should be coated with a special conductive gel. If it is not available, use gauze soaked in 7% sodium chloride solution.
- After selecting the power, the electrodes are charged.
- It is important to pay attention to the correct placement of the electrodes. The right electrode should cover the subclavian area near the sternum, the left electrode should be applied to the apex of the heart. In another embodiment, the left electrode is placed in the fifth intercostal space near the sternum, and the right electrode is placed under the scapula at the level of the second electrode. If the patient has a pacemaker, the left contact should not be closer than 8 cm from the device.
- The discharge is applied to the electrodes touching the body with a force of 10 kgf.
- The result is checked. You may notice a pulse or ECG change.
- If there is no effect, the device will charge with increasing power.
After four unsuccessful attempts, it is concluded that there is no chance of saving the person. Manipulations may include chest compressions and artificial respiration between discharges. It is important that no one touches the patient or his body while the shock is being administered.
Cardioversion should be performed after special preparation:
- Performing an ECG.
- EchoCG. This is a patient's esophageal test to rule out the presence of blood clots in the chambers of the heart.
- Blood test for potassium.
- Stop taking glycosides 3 days before the procedure.
- Refusal from food and water 4 hours before the procedure.
Planned cardioversion requires prior patient consent for the procedure. This is done according to the following algorithm:
- Saturation of the patient's body with oxygen.
- Placing the patient under anesthesia.
- Prepare the electrodes as in the previous case.
- Pressure monitoring and ECG setup.
- Once the shock is delivered, it should be aligned with the QRS complex or R wave to prevent ventricular arrhythmia.
Indications
- ventricular (ventricular) fibrillation;
- ventricular (ventricular) tachycardia without pulse.
Defibrillation is not indicated if the heart has stopped completely (with asystole and pulseless electrical activity), or when the patient is conscious or has a pulse.
Defibrillation in emergencies
In critical situations, defibrillators can be used to stop ventricular arrhythmias. The patient in this case is unconscious.
There are several pathological conditions for which this treatment is indicated:
- Ventricular fibrillation, the rhythm in this case is accelerated and disrupted.
- Trembling as a rhythm, ordered but accelerated.
- Tachycardia when drug treatment is ineffective.
Sometimes, against the background of these disorders, arterial hypotension or circulatory failure is observed.
The clinical picture in this case develops according to the following scenario:
- The man loses consciousness.
- Heartbeats quickly increase.
- The pulse is not felt.
- The patient is considered clinically dead.
CPR should be performed within the first few minutes. If medical attention is not provided immediately, biological death may occur and electrical defibrillation will no longer be effective.
Execution technique
The algorithm for resuscitation by defibrillation, approved by the American Heart Association in 2015, is as follows:
- Make sure there are indications for defibrillation (assessed using ECG data).
- Initiate cardiopulmonary resuscitation (CPR) with oxygen support.
- First category.
- Continue CPR immediately for five cycles (one cycle consists of 30 chest compressions and 2 breaths). You need to make 100 clicks per minute. Accordingly, the CPR break will take exactly 2 minutes.) Place an intravenous catheter and endotracheal tube. Start ventilation at a rate of 10 breaths per minute. Do not check your pulse and rhythm until this time is over.
- Check pulse and heart rhythm.
- If the rhythm is restored, defibrillation is stopped and the patient is placed under observation.
- If the first shock does not give the desired effect, it is worth repeating the shock.
- Repeat the “rhythm check-defibrillation-CPR” cycle.
The steps listed above are performed only by medical personnel.
External automated defibrillators (EADs) are now in widespread use. They can be found at airports, train stations, shopping centers and other crowded places. They are designed so that every person, without prior preparation, can save someone’s life with the help of audio prompts.
- If you witness a person losing consciousness, make sure that he is not responding to external stimuli - speak to him loudly, jog lightly.
- Call 911 or have someone else do it.
- Check if the victim is breathing and if there is a pulse. If these signs are absent or irregular, begin CPR. Have someone prepare the VAD.
- Before using the VAD, make sure that you and the victim are on a dry surface and there is no spilled water nearby.
- Turn on the device. He will guide your further actions.
- Free the victim's chest from clothing and underwear. If it is wet, wipe it off. Apply the adhesive electrodes as shown on the screen (above the right nipple and towards the armpit from the left nipple).
- Deliver a shock. Do not touch the victim at this moment. The human body conducts current, and electrical defibrillation of a healthy heart will incapacitate the resuscitator.
- Perform CPR for 2 minutes. Use a VAD to check your heart rhythm. If he recovers, continue CPR.
- If fibrillation does not stop, repeat the shock.
- Continue the cycle of actions until medical help arrives.
Sudden cardiac arrest and its outcomes.
The leading cause of death in economically developed countries is coronary heart disease (CHD) [20, 22]. The cause of more than 60% of deaths in patients with coronary artery disease is sudden cardiac arrest (SCA) [39] due to the development of ventricular fibrillation (VF) or pulseless ventricular tachycardia (PVT); asystole; electromechanical dissociation (EMD). In European countries, 350,000–700,000 people die per year from SCA (depending on the criteria for its definition); in 80% of cases, SCA occurs in the prehospital stage and in 20% in hospital settings [9, 15, 19, 20, 22, 28]. According to the literature [12, 14, 15], over the past 20 years there has been a decrease in the incidence of VF, which is to a certain extent due to primary and secondary prevention of SCA. Along with this, the time at which the rhythm disturbance is recorded is of fundamental importance. Thus, in case of prolonged (>5-8 min) cardiac arrest at the prehospital stage, primary VF before resuscitation is recorded on average in only 25% (20-30%) of victims. However, if the electrocardiogram can be recorded in the first minutes of SCA, then primary VF can be 59-65% [14, 35]. According to [35], in public places (shopping centers, stadiums, airports, etc.) equipped with automatic external defibrillators (AED), VF and VTBP were the first witnesses to register SCA in 79% of victims. In recent years, in various regions of Canada and the United States, survival[] of revived patients with prehospital VF/VTbp ranges from 7.7 to 40% (median 22%) and for all causes of SCA (asystole, EMD and VF/VT) - 3 -12.6% (median 8.4%) [23, 34]. Of particular interest are studies of SCA at home. It turned out that it accounts for 60–80% of the total number of prehospital SCAs [15, 35]. According to M. Weisfeldt et al. [35], if the first witness of SCA had an AED at home, VF/VTBP was registered in 36% of victims; and in 25% of cases, if resuscitation was initiated by emergency medical services (EMS) personnel. At the same time, the maximum survival rate was on average only 12% (2.8 times less compared to the number of people living in public places equipped with AEDs).
With the development of SCA in the hospital, primary VF and VTBP are registered in various regions of the world in 23-35% of patients with an average survival rate of 23-37%. Another approximately 26% of patients with primary asystole or EMD may develop secondary (so-called terminal) VF during resuscitation [21, 27]. When hospital-acquired primary asystole and EMD develop (approximately 70% of SCA), survival rates average 11 and 12%, respectively. The authors found that if patients with primary asystole or EMD develop terminal VF/VTBP during resuscitation, survival is significantly reduced. Thus, with primary asystole it was 8% (without secondary VF/VTbp - 12%) and EMD - 7% (without secondary VF/VTbp - 14%) [21]. Thus, both prehospital and hospital SCA caused by primary VF/VTbp, in contrast to SCA caused by primary asystole and EMD, is characterized on average by a significantly higher (2.5-3 times) survival rate of revived patients.
Electrical ventricular defibrillation (VD) is a key link in the “chain of survival” after SCA caused by VF and VTbp. It has been established that if basic cardiopulmonary resuscitation (BCPR) is not performed at the prehospital stage, then each minute of delay in DF reduces delayed survival by 7-12%, and if carried out, then by 3-4% [8, 15]. In 2002, M. Weisfeldt and L. Becker [33], based on literature data, formulated the concept of a three-phase time-dependent resuscitation model. According to this model, the authors identified the most important method of treating cardiac arrest in each phase. Thus, during the first phase (electrical phase, duration about 4 min[] from the onset of SEP), the most important treatment method is DF. It has been established that in the absence of effective chest compressions (CHC), successful DF in the first 4 minutes of SCA often leads to restoration of cardiac output, but after 4 minutes this, as a rule, does not occur. It should be noted that early defibrillation (the first 2-5 minutes of SOS) is the most important factor that determines not only the success of resuscitation, but also survival, which can reach 49-74% [14, 32]. The second phase of revival is circulatory (4-10 minutes of SCA) and the 3rd phase is metabolic (after 10 minutes of cardiac arrest). During these two phases, oxygenation, external hypothermia, and a number of other resuscitation measures may be more important than urgent DF [18].
Revision of the international defibrillation protocol for SCA caused by refractory and rapidly relapsing VF/VTBP, valid until 2005.
Recent recommendations recommend that defibrillation be incorporated into pre- and hospital BCPR as quickly as possible. At the same time, the DF protocol and procedure should not negatively affect the quality of CGC [8, 14, 15]. In connection with the above, the main goal of changing the DF protocol, which was in force until the end of 2005, is to reduce the number and duration of breaks during external cardiac massage. To do this, instead of a series of shocks, it is recommended to apply only single shocks at intervals of 2 minutes [14, 15]. Analysis of literature data showed a significantly lower percentage of the interval of “interrupted compressions” with a single shock compared to serial application of 3 shocks. It was established that if the first discharge turned out to be ineffective, then the second discharge is ineffective. Therefore, rapid resumption of BSPR is better than serial application of the 2nd and, even more so, the third shock (even short repeated interruptions of CGC reduce the chance of VF conversion to another rhythm) [10, 14, 15]. The study [26] showed that in prehospital DF with single shocks, patient survival was significantly higher than with serial shocks (46 and 33%, respectively; p<0.01).
Electrical pulse shapes used to eliminate VF (mono- and bipolar).
It should be noted that the success of the first discharge using a bipolar pulse (BPI) is equal to or greater than the success of DF after applying 3 monopolar discharges (MPR) [15]. Based on these data, after 2005 the production of monopolar defibrillators was discontinued. However, they still continue to be used in everyday practice. The recommended value for the 1st and subsequent MPRs is 360 J (i.e., maximum). Experts believe that although there is a risk of myocardial damage from high-energy MPRs, it is much more important to eliminate VF as quickly as possible [14, 15]. According to T. Schneider et al. [29], the success of resuscitation using a BP trapezoidal pulse (set dose 150 J) at the prehospital stage was 22% (76 and 54%) greater than with a monopolar pulse (200-360 J). In this study, the pulse shape did not affect the survival of patients (28 and 31%). At the same time, upon discharge from the hospital in those revived with the help of BPI, good neurological recovery was noted in 78% of patients and only in 53% (p = 0.04) when using a monopolar impulse.
The success of the first shock depending on the type and dose of the bipolar impulse.
The optimal dose of the first BP shock has not been established. This is primarily due to the presence of 4 BP pulses of different types (morphology), as well as the method of compensating the resistance of the chest (SGK, Ohm). Depending on these variables, the energy gained and released to the patient can vary significantly [4, 14]. The currently recommended energy doses for BP pulses (trapezoidal, rectilinear and trapezoidal pulsating) were determined by experts after a thorough analysis of literature data [14, 15]. Thus, when eliminating prehospital VF with trapezoidal pulses of various durations (set dose 150–200 J), the success rate of DF reaches 86–98% [15]. The effectiveness of a straight-line pulse (set dose 120 J) was 88% in the prehospital stage in eliminating the first episode of VF and 80-84% in subsequent episodes of recurrent VF. The success of the first 3 shocks of 120 J at 2-minute intervals in eliminating the first episodes of VF reached 98% (88 out of 90 cases). Increasing the discharge energy to 150–200 J did not eliminate 2 episodes of VF (Zoll M-Series defibrillators, Zoll Medical Systems, USA) [17]. When using a trapezoidal pulsating impulse (set dose 130 J) in the prehospital stage, the success of the first shock was 90%[] (Fred defibrillators; Schiller Medical SAS, France) [13]. The hospital effectiveness of the domestic quasi-sinusoidal BPI (90-115 J) in eliminating the first episode of VF[] was 86-90%. The overall success of eliminating all episodes of recurrent VF with the first shock (set dose 115 J) reached 86%. It should be noted that almost all episodes of VF (99%; 129 out of 130 cases) were eliminated by applying from 1-2 to 4 shocks (65-195 J) [2]. In only one patient with recurrent VF/VTbp, 6 shocks were required to eliminate the third episode; of which 3 are of maximum energy (195 J). One of the likely causes of the development of stable VF/VTBP that arose against the background of heart failure was long-term administration of lidocaine [1, 6]. The overall success of the DF was 100%.
In the table
the installation energy of the first discharge (115-130 J), its success in eliminating the first episode of VF with 3 different types of BPIs and the real range of energy allocated to the patient (Ev, J) with SGC from 40 to 100 Ohms are presented. According to the presented data, with equal (almost 90%) success of the first shock, the real effective energy that eliminates the first episode of VF was greater for straight and pulsating pulses (by 13 and 25%, respectively) than for the domestic quasi-sinusoidal BPI. According to experimental data from F. Qu et al. [25], the type of BPI, all other things being equal, has a significant impact on the threshold energy of the DF. Thus, according to studies conducted on isolated rabbit hearts [25], the threshold energy when using a modified Gurvich sinusoidal pulse[] was 28% less than that of a modified trapezoidal pulse, and 32% less (p<0.05) than for the modified straight-line Zoll pulse. According to the results of our studies (models of domestic pigs with a high SHC = 100 Ohm), the threshold energy of the DF in 2 trapezoidal BPIs turned out to be significantly higher in all animals (on average by 34 and 41%) than in the quasi-sinusoidal BPI [4]. When using a rectilinear BPI compared to a quasi-sinusoidal one, it was more often necessary to apply a greater (16%) threshold energy [5].
Doses of the second and subsequent discharges.
Recommendations [14] suggest both fixed and escalating dose strategies: to date, there is no reason to change this strategy [15]; with a fixed dose tactic, one should first of all proceed from the data presented in the table on the success of the 1st BP discharge[].
Protocol for carrying out BCPR and defibrillation for SCA (recommendations 2010) [15].
If DF is indicated, then a single shock should be applied (preferably BPI), then immediately after it, without determining the rhythm and pulse, resume CGC. In this case, BSPR (30 CHCs and 2 artificial breaths) is carried out for 2 minutes; only after this do they make a short pause (optimally <5 s) to assess the rhythm (in recent years, the first models of manual and automatic defibrillators have appeared, with the help of which it is possible to assess the rhythm against the background of CHC). It should be noted that with prolonged VF, if the first shock is successful, the pulse is rarely determined immediately after it. Therefore, stopping cardiac massage to attempt to determine the pulse[], if a hemodynamically effective rhythm is not restored, will only worsen coronary blood flow and, accordingly, the contractile function of the myocardium. If VF/VTBP is recorded, a second shock is applied and immediately after it, without determining the rhythm and pulse, continuous CGCs are continued [].
The duration of the LSPR is 2 minutes, then a short pause (optimally <5 s) to control the rhythm. If VF/VTbp is detected, a third shock is applied followed by rapid continuation of CPR for 2 minutes. Immediately after resumption of CHC, 1 mg of adrenaline is administered and then 300 mg of amiodarone[]. If the first 3 shocks fail to restore spontaneous circulation, the administration of epinephrine may improve myocardial blood flow and increase the likelihood of success with the fourth shock.
The transport time of the drug to vital organs is 1.5–4 minutes [36]. If an organized rhythm (regular, narrow QRS complexes) is detected after 2 minutes of CPR, the pulse should be assessed. However, its determination, during which the CGCs are stopped, should not exceed 10 s. Any doubt about the presence of a pulse requires immediate resumption of BCPR. The use of capnography can help determine the presence of spontaneous circulation without interrupting CGC [15]. Adrenaline is reintroduced after approximately 3-5 minutes. During preparation for DF, the shock should not be delayed to administer the drug [14]. The further algorithm of DF and BSLR is similar to the above sequences [15]. Resuscitation should be carried out as long as VF/VTBP is registered.
Shallow-wave (<0.3 mV) VF defibrillation.
When small-wave VF is eliminated, most often it quickly recurs or asystole or a hemodynamically ineffective rhythm develops. Therefore, if the first shock is not effective, it is better to continue BCPR instead of applying a second shock. In shallow-wave VF, it is especially important to perform high-quality continuous cardiac massage. When recording small-wave VF, repeated shocks will only increase myocardial damage as a result of both the direct action of electric current and indirectly due to forced pauses in cardiac massage. If small-wave VF is difficult to differentiate from asystole, DF should not be performed. Instead of DF, it is better to continue CPR [14].
Strategy for CPR before defibrillation in case of prolonged SCA (the time from the moment of SCA to the onset of resuscitation exceeds 4-5 minutes).
In a hospital setting (the duration of SOS is often more than 4 minutes), it is recommended to immediately perform DF, since there are no clinical data confirming the clear benefit of performing 2-3 minutes of BCPR before applying the first shock [14, 15]. Outside the hospital (the duration of SCA before the onset of EMS is often >8 min), this resuscitation strategy resulted in increased resuscitation success and survival only when CPR was performed by experienced paramedics who quickly intubated the trachea and administered 100% oxygen. The remaining studies found no positive results. In this regard, according to experts, each EMS manager must decide for himself whether to conduct a “special period” of CPR at the prehospital stage before applying the first shock or not, since there is no convincing data either for or against this strategy [14, 15] .
Hospital automatic external defibrillation.
Over the past 20 years, in economically developed countries of Europe and America, AEDs have been used along with manual defibrillators [14, 15, 34]. Initially, AEDs were used only during prehospital resuscitation by trained nonmedical individuals. However, in the last 10 years, AEDs have begun to be used in multidisciplinary hospitals. This is due to the fact that the average delay time for conventional defibrillation by the resuscitation team is often from 5 to 10 minutes, especially in departments where there is no monitoring of patients. Given the results, experts from the European Resuscitation Council began to consider the performance of hospital defibrillation by the resuscitation team as a strategic mistake. This is explained by the fact that in many cases the resuscitation team cannot quickly arrive at the site of an SCA that occurred in a multidisciplinary hospital [14]. To date, there have been few comparative studies of the use of AEDs and manual defibrillators in hospital settings. Thus, A. Zafari et al. [38] demonstrated greater survival when DF was performed using an AED compared to using a conventional (manual) defibrillator. In another similar study [16], these differences were absent. A mannequin study found that AED use significantly increased the likelihood of delivering 3 shocks, but increased the time to shock delivery with AED use [15].
Expert opinion [14] suggests that the use of AEDs in hospitals should be considered as a way to expedite early defibrillation (target: less than 3 min from SCA), primarily in departments where providers are not trained to recognize arrhythmias or where defibrillators are rarely used. . To do this, it is necessary to train a sufficient number of hospital staff in BCPR using an AED so that the first shock is delivered within the first 2-3 minutes from the moment of SCA [15]. According to a multicenter study [11], the survival rate of patients who underwent defibrillation in the first 2 minutes of DF reached 39.3%, and after 2-3 minutes (“delayed” DF) - 22.2%. Delayed DF was recorded in 30% of patients in this study.
AED operating modes.
Most AEDs can be used in both semi-automatic and manual modes, but there are few studies comparing these modes. Some publications show that the semi-automatic mode reduces the time before the first shock is applied both in a hospital setting and at the prehospital stage; the latter resulted in greater success in eliminating VF and delivery of fewer shocks. However, before delivering the shock, the semi-automatic mode requires a longer interruption of the CGC for automatic rhythm analysis (about 20 s or more). When using manual defibrillators and some AED models, you can continue CBC while the defibrillator is charging. In these cases, the interruption of the CGC before applying the discharge is reduced to 5 s or less []. A shorter pre-shock pause and shorter overall duration of “interrupted compression” periods increase vital organ perfusion time and the likelihood of return of spontaneous circulation. Trained individuals can perform DF manually, but this requires experience in rapid electrocardiogram analysis [cit. according to 15].
The most important changes in the 2010 European Revitalization Council Guidelines [15]:
— the fundamentally important role of uninterrupted cardiac massage is emphasized. Significantly greater attention is being paid to minimizing CGC cessation before and immediately after shock delivery;
— for the first time, it is recommended to continue CGC while charging the defibrillator;
— DF (discharge application) should not interrupt the CGC for more than 5 s (even a 5-10 second pause will reduce the chance of success of the applied discharge);
— in case of refractory and rapidly relapsing VF, adrenaline 1 mg is administered after the third single shock immediately after the resumption of CGC. Amiodarone 300 mg is also given after the third shock;
— application of serial shocks (up to 3 times) is recommended only in cases where SCA occurred in the presence of a doctor and there is a defibrillator next to the patient;
- the role of the precordial stroke is no longer emphasized;
— in the case of SCA at the prehospital stage, EMS personnel must provide high-quality resuscitation until the delivery of the defibrillator and its preparation for shock application; however, an additional 2 to 3 minute period of CPR before rhythm analysis and shock delivery is no longer recommended in routine practice. However, for some medical services that arrive at the scene fully equipped, it would be reasonable to administer a 2-3 minute period of CPR, as there is no evidence either for or against this resuscitation strategy.
The authors of the recommendations suggest using gel-impregnated pads when using defibrillators with manual electrodes to reduce electrode-skin resistance. Electrode pastes and gels without pads may spread between the defibrillator electrodes during cardiac massage, creating a potential risk of sparking during shock delivery.
[]Survival rate (delayed) is the ratio of the number of revived patients who survived to be discharged from the hospital to the total number of patients revived at the prehospital stage of resuscitation.
[]According to experimental studies in pigs, coronary perfusion pressure after the onset of VF during the first 15 s decreases from 60 to 15 mmHg. and then slowly (within 3.5-4 minutes) reaches zero [30]. Studies on animals and mathematical models of resuscitation with chest compressions only have shown that the supply of oxygen in the arterial blood is depleted 2-4 minutes after SCA [cit. according to 15].
[]Late-term survival was 74% if the first shock was delivered within the first 3 minutes of SOS, and 49% if within the first 4.4 ± 2.9 minutes.
[]Experimental and theoretical studies of trapezoidal pulsatile impulse [3, 31] do not agree with the presented data on its clinical effectiveness [22]. This is also indirectly confirmed by the results of the dose-dependent effectiveness of electrical cardioversion of atrial fibrillation [7].
[]The duration of the first episodes of VF is from 1-2 to 8 minutes; with rapid recurrence of VF/VTbp, the total duration of resuscitation was 20-30 minutes or more in several patients.
[]The domestic quasi-sinusoidal pulse (Gurvich-Venin) used in the clinic differs in its characteristics from the modified Gurvich pulse [25].
[]When using a bipolar defibrillator with a maximum energy of 360 J, we recommend delivering a first shock of at least 200 J (usually a trapezoidal shock).
[] It has been established that in 50% of cases it takes more than 24 s to determine the central pulse (the optimal time is 5-10 s).
[]With the development of post-defibrillation asystole, cardiac massage often transfers it to VF, which is easier to eliminate than asystole.
[]Drugs must be administered only against the background of CHC. According to the recommendations [14], adrenaline should be administered 2 minutes after the second single shock, i.e. before applying the third shock. Analysis of literature data [24] showed that in the case of amiodarone use, compared to lidocaine, only early survival increases, i.e. the number of people who were revived at the prehospital stage and survived to be admitted to the hospital.
[]More precisely, a semi-automatic external defibrillator is a device that automatically analyzes the rhythm and sets the charge dose; but the discharge is applied manually. Full automatic DF mode includes automatic discharge; This mode is used only in specialized departments.
[]According to an experimental study, the optimal time for interrupting the CGC before applying a discharge is no more than 3 s [37]. The ideal situation is to apply a shock against the background of continuous cardiac massage.
Further tactics of assisting the patient after an attempt to restore rhythm
If defibrillation is successful, the patient requires observation and care. Often, applying an electrical discharge through the conduction system can cause the development of arrhythmia. Neurological disorders associated with temporary cerebral hypoxia are also possible.
Main goals of further actions:
- diagnosis and treatment of the causes of cardiac arrest;
- minimizing negative consequences on the nervous system.
To do this, the following conditions must be met:
- conducting an ECG in 12 leads;
- conducting encephalography in cases of impaired consciousness (coma) and in patients with epilepsy;
- emergency reperfusion (restoration of blood flow) if the cause of cardiac arrest is myocardial infarction;
- maintaining stable blood pressure and blood glucose levels;
- oxygen supply;
- control of body temperature (within 35-36 ˚C);
- consultation with a neurologist.
Resuscitation actions are stopped:
- if resuscitation measures carried out within 30 minutes are ineffective;
- when declaring death based on irreversible cessation of brain function.
conclusions
Nowadays, not only every ambulance, but also many public spaces are equipped with a defibrillator. According to statistics, the prevailing number of sudden cardiac arrests occur outside medical institutions.
The sooner a victim who has lost consciousness receives first aid, the higher his chances of survival and health. It is possible to bring a patient with ventricular tachycardia or fibrillation back to life if the heart is started with a defibrillator while simultaneously performing cardiopulmonary resuscitation.
Knowledge of the principles of CPR and your concern can save someone's life.
Contraindications
In defibrillation, the patient's life is most important, all other factors are ignored. The only contraindication is complete cardiac arrest. However, during planned cardioversion, manipulations cannot be performed if:
- The patient is taking cardiac glycosides. Otherwise, it may cause ventricular fibrillation.
- Chronic course of heart failure in the stage of decompensation.
- During the procedure, the patient suffers from an acute infectious disease.
- There are contraindications to the use of anesthesia.
- Electrolyte disturbances were detected.
- There are blood clots in the atria.
- Multiple atrial or sinus tachycardia is diagnosed.
- Ventricular hypertrophy or dystrophy is observed.