Tachycardia, which is characterized by increased heart rate, often has nothing to do with blood pressure readings. A high pulse with normal pressure, if it persists for a long time or occurs with a certain frequency, indicates the development of serious pathologies. To establish the cause and make an accurate diagnosis, you should undergo a full examination.
Validol
Validol belongs to the group of vasodilators and has a sedative effect. These tablets are good for high heart rate, but have virtually no effect on blood pressure levels.
Important! The product is indicated for sublingual (sublingual) use. Thanks to this, the therapeutic effect is achieved 3-5 minutes after the tablet is dissolved.
Contraindications:
- hypersensitivity to the components of the drug;
- sugar intolerance;
- diabetes mellitus (with caution).
Side effects:
- allergic reaction - itching, skin rashes, urticaria, Quincke's edema;
- lacrimation;
- nausea;
- dizziness.
Adverse symptoms disappear on their own after reducing the dosage or stopping therapy.
Why does rapid heartbeat occur?
The occurrence of rapid heartbeat can be triggered by various factors, including both the body’s natural reactions to the influence of external stimuli and the presence of pathological changes in organs or systems.
Rapid pulse has two forms of occurrence: physiological and pathological. Physiological palpitations appear against the background of psychoemotional disorders, excessive physical exertion, prolonged exposure to sunlight, overeating, insomnia, consumption of alcohol, caffeine, drugs, hormonal activity with increased arousal. Heart rhythm disturbances due to such influence factors are a natural compensatory reaction of the body. Treatment of physiological tachycardia is not required. To stop an attack, just calm down and rest.
The pathological form of a rapid pulse occurs due to the presence of concomitant diseases, in which rhythm disturbance acts as a symptom, and treatment of cardiac tachycardia with tablets is an integral process.
Such pathologies include:
- hypertonic disease;
- heart disease (myocarditis, cardiomyopathy, heart failure);
- pathologies of the endocrine system (hypothyroidism, hypoglycemia, diabetes mellitus);
- diseases of the hematopoietic organs (anemia, leukopenia);
- renal failure;
- malignant neoplasms;
- internal bleeding;
- brain damage;
- infectious pathologies.
Treatment of palpitations, which is determined solely by the attending physician, directly depends on the etiology of the condition.
In pregnant women, the condition is diagnosed in 70%. The increase in pulse rate in this category of patients occurs by 10-20 units even in a normal state. This process is natural, since a woman gains weight and often succumbs to stress. As a medicine for discomfort during tachycardia, you can use sedative drugs with a natural composition, for example, valerian or motherwort.
Asparkam
Asparkam is a medicine from the group of antiarrhythmics. It also does not cause a decrease in blood pressure. The daily dose for an adult is no more than 6 tablets, which must be divided into three doses.
Asparkam should be taken after meals.
Contraindications:
- increased sensitivity to the component composition;
- cardiogenic shock;
- severe myasthenia gravis;
- dehydration;
- increased content of magnesium and potassium in the body;
- oliguria;
- anuria;
- metabolic acidosis;
- atrioventricular block 2–3 degrees;
- liver dysfunction;
- high risk of developing edema.
Side effects:
Causes of rapid heart rate with normal blood pressure
- nausea, vomiting, epigastric pain;
- loose stools;
- dry mouth;
- abdominal discomfort;
- decreased blood pressure;
- myocardial conduction disturbance;
- paresthesia;
- convulsions;
- skin rashes;
- itching;
- facial redness;
- feeling of heat.
Pathological causes
A rapid pulse can be observed against the background of normal blood pressure with congenital and acquired heart defects. These pathological conditions are characterized by a variety of manifestations and have varying degrees of danger. In most cases, the problem can only be eliminated surgically.
Another common cause of rapid pulse associated with the development of cardiac pathologies are inflammatory diseases that affect the structure of the heart muscle. These are myocarditis, endocarditis, rheumatism, etc. Without appropriate therapy, these diseases pose a threat to life.
Rapid pulse also occurs for the following pathological non-cardiac reasons:
- Dehydration. When the body loses a lot of fluid, the blood thickens. This increases the load on the heart muscle, which causes it to contract more intensely.
- Infectious diseases. When the temperature rises, the body becomes intoxicated. In order to quickly remove harmful substances from the body and normalize the condition, the heart begins to pump blood faster.
- Neurotic diseases. The level of stress increases in such cases due to the release of large amounts of stress hormones.
- Hormonal disorders. As a rule, they are associated with dysfunction of the thyroid gland and adrenal glands. An increased amount of hormones leads to intoxication of the body. Against this background, the heart muscle begins to work more intensely.
- The occurrence of severe bleeding. This is due to a violation of the volume of blood circulating in the body. To provide tissues with the necessary amount of nutrients and oxygen, it is necessary to accelerate the pumping of hematological fluid through the vessels.
- Anemia. Most often, increased heart rate is observed with iron deficiency anemia. Additionally, increased fatigue with minimal physical activity and deterioration of the condition of the skin and nails are noted.
Bisoprolol
Bisoprolol is used to normalize pulse at high blood pressure. The active substance is bisoprolol fumarate. The drug belongs to the group of β1-blockers. It has the following effects: antianginal (elimination of symptoms of myocardial ischemia), antiarrhythmic (reduces heart rate), antihypertensive (normalization of blood pressure).
Important! The drug has a fairly large list of contraindications, so before you start taking it you need to make sure that they are absent.
During treatment, a person may experience:
- headache;
- dizziness;
- increased fatigue;
- flushes of blood to the face;
- sleep disorders;
- depression, hallucinations (rare);
- paresthesia;
- disruption of tear production;
- conjunctivitis;
- pain in the abdomen;
- nausea, vomiting;
- stool disorders - diarrhea and constipation are possible;
- muscle weakness;
- convulsions;
- increased sweating;
- bradycardia.
The drug is prescribed with caution to patients with psoriasis, diabetes mellitus in the stage of decompensation, predisposition to allergic reactions and those people whose work is associated with a high speed of psychomotor reactions.
Blood thinners for heart problems
Separately, it is worth considering blood thinners, which are prescribed to prevent the formation of dangerous blood clots. These medications include antiplatelet agents and anticoagulants, which have the side effect of increasing the risk of bleeding. If a doctor prescribes one of these drugs to a patient, this means that great care must be taken with any injury, surgery, or even dental procedures.
Antiplatelet agents
These drugs work by directly affecting the function of platelets in the blood. Platelets are special cells that help stop bleeding by sticking together and forming a clot.
List of drugs with antiplatelet action:
- clopidogrel (Plavix);
- prasugrel;
- tirofiban (aggrastat);
- dipyridamole.
Anaprilin
Anaprilin belongs to the group of beta-blockers. It has hypotensive, antiarrhythmic and antianginal properties. The active ingredient is propranolol. The drug is used if the blood pressure is high and the pulse is significantly increased.
The drug is effective in the initial stage of arterial hypertension, so the drug is used in young patients. A decrease in systolic pressure is accompanied by a decrease in the frequency of myocardial contractions.
Anaprilin is part of the group of beta-blockers
Contraindications:
- arterial hypotension;
- individual intolerance to the component composition;
- heart failure;
- atrioventricular block;
- sinus bradycardia;
- diabetes;
- predisposition to the development of bronchospasm;
- myocardial infarction;
- bronchial asthma;
- period of gestation and breastfeeding.
Side effects: bradycardia, bronchospasm, nausea, vomiting, muscle weakness, hypoglycemia, blurred vision, decreased potency, heart failure. If the regimen and dosage of the drug are not followed, the development of the following conditions cannot be ruled out: arrhythmia, convulsions, difficulty breathing, bronchospasm, dizziness, heart failure.
In case of overdose, Anaprilin can greatly reduce the pulse. The drug should absolutely not be combined with alcohol intake. In this case, death cannot be ruled out. The medicine cannot be combined with antipsychotics and tranquilizers. In the case of long-term course treatment with Anaprilin, the use of cardiac glycosides is recommended.
Symptoms of increased heart rate
Usually, when the pulse increases, the patient feels some discomfort in the heart area. It manifests itself primarily in the heartbeat (with a normal pulse, a person does not feel the work of his heart). The heart is pounding, “jumping out of the chest.” Pain of various types may appear behind the sternum or in the left half of the chest.
Due to deterioration of blood supply to the whole body, symptoms such as:
- dizziness;
- weakness;
- severe shortness of breath, with difficulty in inhaling;
- nausea;
- sleep disturbance;
- nausea and even vomiting;
- loss of consciousness.
All this precedes the detection of an increased pulse and very often requires the intervention of specialists.
Persen
Persen belongs to the group of herbal preparations. Extracts of valerian, lemon balm, and peppermint are used as active ingredients. Thanks to its complex composition, Persen has a calming (due to the presence of valerian), mild sedative and antispasmodic effect. The pulse-lowering ability is based on calming the human central nervous system.
Contraindications:
- individual intolerance to glucose, lactose;
- lack of sucrose;
- diseases of the biliary tract – gallstones, cholangitis and others;
- arterial hypotension;
- bearing a child and the period of breastfeeding;
- children's age - Persen is not prescribed to children under 12 years of age;
- intolerance to the component composition of the drug.
In the presence of gastroesophageal reflux disease, the drug is prescribed with caution. During treatment, allergic reactions and constipation may develop. The tablets should be taken orally with the required volume of any liquid.
Persen is a herbal preparation with a calming effect
The duration of the course is no more than 1.5 months. After stopping treatment, withdrawal syndrome does not develop. An overdose of Persen (in case of taking more than 60 or more tablets at the same time) is indicated by the appearance of nausea, general weakness, dizziness, and hand tremors. Treatment of the condition is symptomatic.
The drug should be taken carefully with antihypertensive and hypnotic drugs, since Persen enhances the effect of these medications. If such a need arises, dosage adjustments will be required.
Pulse-slowing calcium antagonists - role in modern therapy of cardiovascular diseases
T
The term “calcium antagonists” was first proposed by Fleckenstein in 1969 to designate the pharmacological properties of drugs that had both coronary vasodilating and negative inotropic effects [1]. The effect of these drugs on the myocardium was very similar to the signs of calcium deficiency described by Ringer in 1882 [2]. The first representative of calcium antagonists, verapamil, was synthesized on May 21, 1959 by Dr. Ferdinand Dengel, 10 years earlier than the term “calcium antagonists” appeared. In 1963, clinical use of verapamil for the treatment of angina pectoris was initiated. In the 70s of the last century, two other representatives of calcium antagonists were created and began to be used in the clinic - nifedipine and diltiazem.
Classification of calcium antagonists
Calcium antagonists are a heterogeneous group of drugs. Based on their chemical structure, they are divided into dihydropyridines
(nifedipine, amlodipine, lacidipine, etc.),
phenylalkylamines
(verapamil),
benzothiazepines
(diltiazem).
Within each subgroup of antagonists, first-generation drugs are distinguished (tablets of regular duration of action, they are prescribed 3-4 times a day) and second-generation drugs (extended-release tablets or capsules, they are prescribed 1 or 2 times a day).
The classification of calcium antagonists is very important for the clinician, dividing all drugs into two large subgroups based on their effect on the tone of the sympathetic nervous system. The first subgroup is the so-called pulse-slowing calcium antagonists (or non-dihydropyridine calcium antagonists). These actually include two drugs - verapamil and diltiazem. The second subgroup is pulse-increasing calcium antagonists, or dihydropyridines.
Basic pharmacological properties
The properties of calcium antagonists that slow down the pulse are dominated by negative inotropic (decreased myocardial contractility) and negative chronotropic (decreased heart rate - HR) effects, as well as the ability to reduce atrioventricular conduction (Table 1). These properties are more pronounced in verapamil and to a slightly lesser extent in diltiazem. Due to these properties, non-dihydropyridine calcium antagonists reduce the tone of the sympathetic nervous system and reduce the myocardial oxygen demand. This action brings pulse-slowing calcium antagonists closer to b-blockers (interestingly, verapamil was also initially considered a b-blocker). The vasodilating effect of calcium antagonists that slow down the pulse also occurs, but is less pronounced than that of dihydropyridines.
The pulse-increasing properties of calcium antagonists are dominated by their ability to cause dilatation of peripheral arteries. Due to this, they increase the tone of the sympathetic nervous system and increase heart rate.
Clinical use
The above-described features of the action of the two subgroups of calcium antagonists leave an imprint on the features of their use in the clinic (Table 2). Both subgroups are used for the treatment of arterial hypertension and stable angina pectoris, as well as vasospastic angina. Dihydropyridine calcium antagonists are considered contraindicated in patients with unstable angina and acute myocardial infarction (see below), verapamil and diltiazem have been used successfully in these conditions.
Verapamil and diltiazem have antiarrhythmic properties (they form a separate group of antiarrhythmic drugs) and are widely used to treat supraventricular arrhythmias. Dosage forms of verapamil for intravenous administration are very effective in stopping paroxysmal supraventricular tachycardias. Both verapamil and diltiazem are often used successfully in persistent atrial fibrillation to control heart rate.
Non-dihydropyridine calcium antagonists have a fairly pronounced clinical effect in hypertrophic cardiomyopathy. It was shown that these drugs contributed to significant clinical improvement (decreased palpitations, shortness of breath, dizziness and weakness), and an increase in the duration of dosed physical activity [3].
There are conflicting opinions about the possibility and advisability of using calcium antagonists in heart failure. It is currently believed that, as a rule, calcium antagonists are not indicated for this condition. There is evidence that the addition of verapamil to ACE inhibitors improves left ventricular function.
Evidence-based medicine data
The high clinical effectiveness of calcium antagonists has led to these drugs being intensively studied in controlled randomized trials assessing the effect on the so-called “end points” - mortality rates and the likelihood of severe complications. As you know, it is these indicators that “evidence-based medicine” primarily focuses on.
Not all calcium antagonists have yielded positive results from such studies, for example, in acute myocardial infarction. However, the use of non-dihydropyridine antagonists in such patients has been successful. In the 80s In Denmark, 2 large randomized studies were conducted that examined the effect of verapamil on long-term outcomes of acute myocardial infarction
, -
DAVIT-1
(Danish Verapamil Infarction Trial) and
DAVIT-2
. The DAVIT-1 study included 1775 patients with acute myocardial infarction. On the 2nd week after admission to the hospital, patients were randomized into 2 groups: 878 were prescribed verapamil 120 mg 3 times a day, 897 patients received placebo. The study did not include patients with severe hypotension, atrioventricular and sinoatrial blockade, and severe congestive heart failure (which was understood as heart failure when it was necessary to prescribe furosemide at a dose exceeding 160 mg per day). The follow-up period for patients averaged 16 months [7].
During the observation period, 95 patients in the verapamil group and 119 patients in the placebo group died (p = 0.11). The incidence of major complications from the cardiovascular system in patients receiving verapamil (18%) was significantly lower compared to patients receiving placebo (21.6%, p = 0.03).
The data from the differentiated analysis turned out to be especially interesting. In patients without signs of heart failure in the acute period of myocardial infarction who received verapamil, the mortality rate was 7.7%, and in the same patients who received placebo it was 11.8% (p = 0.02). In addition, it was found that the effectiveness of verapamil differed in patients with and without signs of myocardial ischemia during an exercise test performed before the patients were discharged from the hospital. In patients with ST segment depression during physical activity, the use of verapamil helped reduce the incidence of complications from the cardiovascular system by 41%, and in patients without ST segment depression during physical activity, it did not affect their number. From this it was concluded that the main mechanism of the protective effect of verapamil is its ability to prevent the occurrence of myocardial ischemia.
The same study assessed the effect of verapamil in patients with concomitant arterial hypertension. There were 301 such patients. 149 of them received verapamil, 152 received placebo. The rate of recurrent myocardial infarction was 12.5% in the verapamil group; in the placebo group it was significantly lower (19.8%).
Shortly after the completion of the DAVIT-1 study, the DAVIT-2 study was initiated. It included 1775 patients with acute myocardial infarction. Treatment with verapamil (120 mg 3 times a day) began only in the 2nd week after the onset of the disease and lasted an average of 16 months. At the end of the study, mortality in the group of patients receiving verapamil was 11.1%, and in the group of patients receiving placebo - 13.8% (the difference was not significant). The incidence of recurrent myocardial infarction under the influence of verapamil decreased significantly (11.0% and 13.2%). It was also noted that under the influence of verapamil, the frequency of sudden death and “first cardiac event rates” significantly decreased [8]. Analysis of the results in different subgroups showed that in patients without signs of congestive heart failure, the administration of verapamil significantly reduced the mortality of patients (by 36%).
The ability of verapamil to influence the prognosis of coronary artery disease
was studied in another large multicenter randomized trial, which was conducted in Italy and was called
CRIS
(Calcium Antagonist Reinfarction Italian Study) [9]. It included 1073 patients who had suffered a myocardial infarction, without severe heart failure and who had no contraindications to the use of verapamil. 7-21 days after myocardial infarction, 531 patients were prescribed verapamil at a dose of 360 mg/day, 542 patients were prescribed placebo. The observation period for patients averaged 23.5 months. The difference in mortality between patients receiving verapamil and placebo was not significant, but the incidence of recurrent myocardial infarction among patients receiving verapamil was lower than among patients receiving placebo (39 and 49 people, respectively). In addition, patients receiving verapamil were significantly less likely to have angina (compared to patients receiving placebo).
A number of studies have examined the effect of verapamil in patients with stable ischemic heart disease. To the APSIS
(The Angina Prognosis Study in Stockholm) included 809 patients with stable angina pectoris who were prescribed either metoprolol at a dose of 200 mg once a day or verapamil retard at a dose of 240 mg twice a day [10]. The follow-up period for patients averaged 3.4 years. There were no differences between the groups of patients receiving verapamil and metoprolol in overall mortality, mortality from cardiovascular diseases, or the incidence of nonfatal myocardial infarction.
Diltiazem, like verapamil, has also been extensively studied in patients with coronary artery disease who have suffered myocardial infarction. In the MDIPT
(The Multicenter Diltiazem Postinfarction Trail) studied the effect of long-term diltiazem therapy on mortality and the likelihood of recurrent myocardial infarction. The study included 2466 patients with acute myocardial infarction (mostly large-focal), some of whom received diltiazem (240 mg per day), and some received placebo. Observation of patients lasted from 12 to 52 months. Overall mortality was the same in both groups of patients (167 and 166 patients, respectively). The frequency of “first recurrent cardiac event”, which was understood as either the development of repeated non-fatal myocardial infarction or death from cardiac causes, in the group of patients receiving diltiazem was significantly lower than in the group of patients receiving placebo (202 and 226 patients, respectively). A differentiated analysis showed that among patients without signs of pulmonary congestion, diltiazem caused a significant decrease in mortality and the incidence of recurrent myocardial infarction, and among patients with signs of pulmonary congestion, it slightly increased mortality and the incidence of recurrent myocardial infarction [11].
Calcium antagonists have also been intensively studied in arterial hypertension.
.
It should be noted that in this case, conflicting opinions are expressed about the advisability and even safety of using these drugs. No. 9 of the Breast Cancer Journal, 2003, provides a review of large randomized studies (in which more than 1000 people participated) in which calcium antagonists were used in patients with arterial hypertension (in total, 7 such studies have been performed in recent years) [12]. Of these, 2 studies used pulse-slowing calcium antagonists (verapamil - VHAS
- Verapamil in Hypertension and Atherosclerosis Study, diltiazem -
NORDIL
- The Nordic Diltiazem Study).
In the VHAS
1414 patients with arterial hypertension (blood pressure above 160/95 mmHg) were included. Some patients began treatment with verapamil retard, some patients with chlorthalidone (this drug is the standard diuretic). After 1 month, in case of insufficient effect, captopril was added to the treatment. In both groups, an identical and statistically significant decrease in blood pressure was recorded. After 2 years of follow-up, the incidence of cardiovascular events in the verapamil group was 42 per 707 people, and in the chlorthalidone group - 43 per 707 people [13].
In the NORDIL
More than 10,000 patients with arterial hypertension participated. One group of patients received diltiazem, the other group received a b-blocker and/or a diuretic. After 5 years of follow-up, the frequency of endpoints in both groups was the same. The incidence of stroke in the group of patients receiving diltiazem was significantly lower [14].
It should also be mentioned that the large controlled study INVEST
(International Verapamil SR/trandalopril Study) in more than 22,000 patients with arterial hypertension and coronary heart disease, in which a prolonged form of verapamil was chosen as the main drug [15]. The INVEST results demonstrate that verapamil-based treatment for these patients is as effective in reducing mortality rates and the risk of cardiovascular complications and strokes as beta-blocker therapy.
Thus, according to most large randomized studies, the administration of calcium antagonists in patients with arterial hypertension is no less effective than the administration of antihypertensive drugs of other groups.
Contraindications for use
Contraindications to prescription for pulse-slowing calcium antagonists are quite different from those for dihydropyridine calcium antagonists. Verapamil and diltiazem should not be prescribed for sick sinus syndrome, atrioventricular block, or severe sinus bradycardia (resting heart rate less than 55 beats per minute).
As already noted, it is undesirable to prescribe verapamil and diltiazem for severe heart failure.
Side effects
Verapamil and diltiazem are significantly less likely than dihydropyridine calcium antagonists to cause swelling in the legs. They are not characterized by side effects associated with excessive vasodilation, which are typical for dihydropyridine calcium antagonists (tachycardia, feeling of heat, redness of the skin, etc.).
The most common side effect of verapamil and diltiazem is the appearance of atrioventricular block. Verapamil also often causes constipation, especially in older people. However, the frequency of this side effect is often exaggerated. Thus, on average, the incidence of constipation when taking verapamil is 4% [15].
Practical recommendations
Thus, calcium antagonists that slow down the pulse are very effective drugs, in no way inferior to dihydropyridine calcium antagonists. Moreover, in a number of conditions they have significant advantages over dihydropyridines (after myocardial infarction, with unstable angina, in the presence of concomitant supraventricular arrhythmias). It is important that pulse-slowing calcium antagonists can be used in cases where there are obvious indications for the use of beta-blockers (for example, after myocardial infarction), but when these drugs cannot be prescribed due to contraindications to them (for example, with bronchial asthma, insulin-dependent diabetes mellitus).
It should be remembered that effective doses of non-dihydropyridine calcium channel blockers vary between patients. On average, they are 240-480 mg per day for verapamil, 180-360 mg per day for diltiazem. Of course, at present preference should be given to second-generation drugs, which are prescribed 1-2 times a day. One of these drugs is Verogalid-ER
, containing 240 mg verapamil per tablet.
References:
1. Fleckenstein A., Tritthart H., Fleckenstein B., Herbst A., Grun G. Eine neue Gruppe kompetitiver Ca++ -Antagonisten (Iproveratril, D6000, Prenylamin) mit starken Hemeffekten auf die elektromekanische Koppelung im Warmbluter-myocard. Pflugers Arch 1969:307:R25.
2. Ringer S. A further contribution regarding the influence of the different constituents of the blood on the contraction of the heart. J. Physiol. Lond. 1882; 4: 29-42.
3. Toshima H., Koga Y., Nagata H., Toyomasu K., Itaya K. et al. Comparative effects of oral diltiazem and verapamil in the treatment of hypertrophic cardiomiopathy. Double-blind crossover study. Japanese Heart J. 1986; 27: 701-715.
4. Report of the Holland Interuniversity Nifedipine/Metoprolol Trial (HINT) Research Group. Early treatment of unstable angina in the coronary care unit: a randomized double-blind placebo-controlled comparison of recurrent ischaemia in patients treated with nifedipine or metoprolol or both. Br. Heart J 1986; 56: 400 – 413.
5. Secondary Prevention Reinfarction Israeli Nifedipine Trial (SPRINT). A randomized intervention trial of nifedipine in patients with acute myocardial infarction. Eur. Heart J 1988; 9: 354-364.
6. Goulbourt U., Behar S., Reicher-Reiss H. et al. Early administration of nifedipine in suspected acute myocardial infarction. The Secondary Prevention of Reinfarction Israel Nifedipine Trial 2 Study. Arch. Intern. Med. 1993; 153: 345 – 353.
7. The Danish Study Group on Verapamil in Myocardial Infarction. Verapamil in acute myocardial infarction.Eur. Heart J 1984; 5: 516 - 528.
8. The Danish Study Group on Verapamil in Myocardial Infarction. The effect of verapamil on mortality and major events after acute myocardial infarction. (The Danish Verapamil Infarction Trial II - DAVIT II). Am. J. Cardiol. 1990; 66: 33I - 40I.
9. Rengo F., Carbonin P., Pahor M., De Caprio L., Bernabei R., Ferrara N., Carosella L., Acanfora D., Parlati S., Vitale D., CRIS Investigators. A controlled Trial of verapamil in patients after acute myocardial infarction: results of the Calcium Antagonist Reinfarction Italian Study (CRIS). Am. J. Cardiol. 1996; 77: 365 – 369.
10. Rehnqvist N., Hjemdahl P., Billing E., Bjorkander I., Erikssson SV, Forslund L., Held C., Nasman P., Wallen NH Effects of metoprolol vs verapamil in patients with stable angina pectoris. The Angina Prognosis Study in Stockholm (APSIS). Eur. Heart J 1996; 17: 76 - 81.
11. The Multicenter Diltiazem Postinfarction Trail Research Group. The effect of diltiazem on mortality and reinfarction after myocardial infarction. N.Engl. J. Med. 1988; 319: 385 – 392.
12. Martsevich S.Yu. The role of calcium antagonists in modern treatment of cardiovascular diseases. Russian medical journal 2003; 11: 539-541.
13. Rosei E. A., Dal Palu C., Leonetti G. et al. Clinical results of the Verapamil in Hypertension and Atherosclerosis Study. VHAS Investigators. J Hypertens 1997; 15: 1337-1344.
14. Hansson L., Hender T., Lund-Johansen P. et al. Randomized trial of effects of calcium antagonists compared with diuretics and beta-blockers on cardiovascular morbidity and mortality in hypertension: the Nordic Diltiazem (NORDIL) study. Lancet 2000; 356: 366-372.
15. Speders S; Sosna J; Schumacher A; Pfenningsdorf G. Efficacy and safety of verapamil SR 240 mg in essential hypertension: results of a multicentric phase IV study. J Cardiovasc Pharmacol. 1989; 13 Suppl 4: S47-9
St. Petersburg study on the basis of the city Antiarrhythmic Center, conducted by T.N. Novikova, S.A. Zhemchuzhny, E.O. Pavlova, A.A. Fomicheva, “Evaluation of the effectiveness and tolerability of Verogalid (verapamil 240 mg; sustained-release tablets)”
Purpose of the study
1. Assess the effectiveness and tolerability of Verogalide (verapamil 240 mg; sustained-release tablets).
2. Compare the effectiveness of Verogalide and short-acting verapamil.
Material and methods
29 patients were examined, average age 62.4+10.5 years, 16 women, 13 men with diseases of the cardiovascular system (Table 1).
Concomitant diseases are presented in Table 2. The most common concomitant diseases were those for which other antiarrhythmic drugs, except verapamil, were contraindicated. 4 patients had no concomitant diseases.
Rhythm disturbances that complicated the course of the underlying disease are presented in Table 3.
Before switching to Verogalide, all patients received verapamil at an average daily dose of 188.0+56.7 mg. The patients were switched to taking Verogalid at an average daily dose of 193.3 + 60.2 mg (the difference with the average daily dose of verapamil is not significant, p = 0.820).
The following indicators were monitored during the month:
- heart rate (2 times a day: in the morning, before taking Verogalid and in the evening);
- blood pressure (2 times a day: in the morning, before taking Verogalid and in the evening);
- number of angina attacks;
- number of rhythm disturbances.
The data were processed using the statistical software package Statistica for Windows version 5.5, developed by StatSoft Inc. (USA) in 1995-2000.
results
The average values of heart rate and blood pressure while taking short-acting verapamil and Verogalide are presented in Table 4.
The average values of heart rate and blood pressure while taking Verogalid were lower than the values recorded while taking verapamil, but the difference turned out to be statistically significant only for the morning heart rate and systolic blood pressure, both morning and evening.
Of the two patients with atrial extrasystole, in one it completely disappeared while taking Verogalid.
The number of episodes of atrial tachycardia while taking short-acting verapamil averaged 5 per week. While taking Verogalid, the number of episodes of atrial tachycardia decreased by more than 2 times and amounted to 2-3 episodes per week.
In one patient with paroxysmal reciprocal atrioventricular tachycardia, the number of paroxysms (PRAVUT) while taking verapamil reached 8 per day. During the month of taking Verogalid, PRAVUT was not registered.
Three patients with paroxysms of atrial fibrillation, due to the presence of contraindications to the administration of other antiarrhythmic drugs, received short-acting verapamil and then were switched to taking Verogalid. A decrease in the number of paroxysms of atrial fibrillation was recorded while taking Verogalid - from 0.8 episodes per week while taking short-acting verapamil to 0.2 episodes per week while taking Verogalid.
Control of the frequency of ventricular responses while taking Verogalide was more adequate than when taking short-acting verapamil. As for painful ischemic episodes, out of 23 patients suffering from ischemic disease in combination with or without arterial hypertension, only one patient did not experience a reduction in the number of painful episodes.
Verogalide was well tolerated by 96.6% of patients. Only one patient, who suffered from a paroxysmal form of atrial fibrillation, noted an increase in extrasystole while taking Verogalid and refused to take it. On the 7th day after returning to taking short-acting verapamil, the patient developed a paroxysm of atrial fibrillation (no paroxysms of atrial fibrillation were recorded while taking Verogalid).
conclusions
- Verogalide, the modern dosage form of verapamil, is well tolerated by patients.
- Due to the uniform concentration of the drug in the blood throughout the day, stable control of blood pressure, heart rate and antianginal effect is ensured.
- The drug is able to control not only PRAVUT, atrial tachycardia, but also, possibly, the paroxysmal form of atrial fibrillation - due to the ability to lengthen the refractory period of the atrial myocardium. However, the latter assumption requires further, more thorough confirmation.
- The effectiveness of Verogalide is superior to that of short-acting verapamil in controlling heart rate, blood pressure, anginal episodes and preventing supraventricular arrhythmias.
Valerian
To normalize a rapid pulse with normal blood pressure, you can use valerian tablets. They contain an extract from the plant as the main active ingredient. The drug helps not only to lower the heart rate by reducing the degree of excitability of the central nervous system, but also has a hypnotic and sedative effect.
Important! The sedative effect develops slowly but is stable.
Contraindications:
- individual reaction to the components of the tablets;
- depression and other conditions accompanied by central nervous system depression;
- galactose intolerance;
- lack of lactase;
- glucose-galactose malabsorption syndrome.
Side effects:
- increased drowsiness;
- dizziness;
- feeling depressed;
- poor performance;
- headache;
- nausea;
- allergic reactions - skin rashes, itching, local swelling - in case of intolerance to the component composition of the drug.
To eliminate unpleasant symptoms, it is necessary to reduce the dosage or completely stop taking Valerian. According to the instructions, adults and children over 12 years of age need to take one or two tablets three times a day. They must be swallowed without chewing, washed down with the required volume of any liquid.
The decrease in heart rate, due to a decrease in the excitability of the central nervous system, occurs slowly. For this reason, the drug is not suitable for emergency use. An overdose is indicated by:
- dizziness;
- drowsiness;
- headache;
- lethargy, general weakness;
- hand trembling;
- dilated pupils;
- visual and hearing impairment;
- feeling of tightness behind the sternum.
Treatment of the condition involves gastric lavage and taking activated carbon tablets. If necessary, carries out symptomatic therapy. Valerian enhances the effect of ethanol, antispasmodics and sedatives. If a person simultaneously takes synthetic sedatives, he needs constant medical supervision.
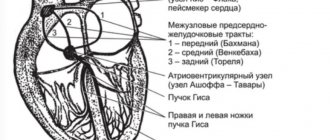
Features of the treatment of heart rhythm disorders
If patients experience irregular beating of the upper chambers of the heart, arrhythmia is diagnosed. For example, after a good amount of stress, the atria become out of sync with the lower chambers, called the ventricles. When this happens, not all the blood is pumped out of the heart. This can cause blood to fill the atria, which can cause clots to form. If one of these clots begins to move, it can restrict blood flow to the brain, which in turn can lead to a stroke.
Arrhythmia can lead to stroke
People with arrhythmia may suffer from strong and irregular heartbeats both on a regular basis and in certain abnormal life situations. Fortunately, modern pharmaceuticals offer many medications for the treatment of arrhythmia. Cardiologists usually do not recommend treating heart problems with natural remedies, but rather immediately start taking synthetic drugs.
Only tablets will quickly and effectively help regulate and control your heart rhythm and its speed. As a positive side effect, patients may notice a decrease in high blood pressure and an overall feeling of well-being. In addition, most of the following medications will also help prevent blood clots.
New generation of drugs
New generation drugs that reduce the pulse to normal but do not reduce blood pressure include Ivabradine and Coraxan
Ivabradin
Ivabradine belongs to the group of antianginal and anti-ischemic drugs. The decrease in heart rate at rest occurs by approximately at least 10 beats per minute. The myocardium works in a more relaxed mode. Additionally, there is a decrease in oxygen consumed by the heart muscle.
Contraindications:
- myocardial infarction;
- significant reduction in blood pressure;
- bradycardia;
- cardiogenic shock;
- sinoatrial block;
- chronic heart failure;
- lactation;
- presence of an artificial pacemaker;
- unstable angina;
- pregnancy;
- allergy to the active ingredient;
- age up to 18 years.
When using Ivabradine, the likelihood of developing bradycardia is minimal
Side effects:
- bradycardia;
- headache;
- dizziness;
- extrasystoles;
- fainting conditions;
- muscle cramps;
- nausea;
- diarrhea/constipation;
- shortness of breath, etc.
Coraxan
Coraxan belongs to the group of antianginal drugs. The active ingredient of the drug is ivabradine. The medicine helps normalize heart rate without having any effect on blood pressure.
Contraindications:
- acute period of myocardial infarction;
- intolerance to the components of the drug;
- bradycardia (with heart rate less than 60 beats per minute);
- cardiogenic shock;
- renal/heart failure;
- arterial hypotension;
- non-adaptive artificial pacemaker;
- age up to 18 years.
Coraxan can be taken with caution and under constant medical supervision (in a hospital setting) in the following cases: congenital long QT syndrome, recent ischemic stroke of the brain, second-degree atrioventricular block.
Coraxan is a dose-dependent drug, therefore, if the prescribed dosage is exceeded, the development of the following side effects cannot be ruled out:
- feeling of heartbeat;
- atrioventricular block;
- acquired weakness of the sinus node;
- atrial fibrillation;
- headache;
- allergic reactions;
- increased drowsiness, fatigue;
- general malaise.
Causes of increased heart rate
The normal heart rate for a healthy person is 60-90 beats per minute. These figures are relatively arbitrary; they guide doctors in their work. Practice shows that people with a pulse of 55 or 98 can feel quite satisfactory, unless, of course, they are among those who look for sores in themselves only based on the numbers on the tonometer display.
Most often, the pulse quickens under the influence of emotional or physical stress. This is a normal process aimed at satisfying the body’s increased needs for oxygen. However, tachycardia can also occur under the influence of other factors:
- panic attack;
- taking certain medications;
- drinking excessive amounts of coffee and caffeinated drinks;
- taking amphetamines;
- smoking;
- drinking alcohol;
- deficiency of potassium and magnesium in the blood;
- increasing the production of thyroid hormones;
- a sharp release of adrenaline and norepinephrine with pheochromocytoma;
- myocardial ischemia in coronary heart disease.
By the way, people often fall into a state close to panic when using automatic blood pressure monitors with a low-quality heart rate monitor. To avoid this, it is best to learn how to measure the pulse by feeling it on the radial artery of the hand. You need to feel the pulsation on your wrist with your index, middle and ring fingers, count the number of beats in 30 seconds and multiply by two.
Additional recommendations
High pulse and low blood pressure are a serious condition, since many drugs intended to normalize heart rate further reduce blood pressure. Beta-blockers, cardiac glycosides, medications intended to replenish magnesium and potassium deficiency, drugs with a sedative effect, and tranquilizers can stabilize the pulse and at the same time increase blood pressure.
For low pulse and high blood pressure, medications should be selected by the attending physician. With such a combination, there are no emergency remedies. The most commonly used long-acting antihypertensive (BP-lowering) drugs are:
- angiotensin receptor blockers – Valsacor, Lozap;
- ACE inhibitors – Capoten, Enalapril;
- alpha-blockers – Tonacardin, Doxazosin;
- diuretics – Hypothiazide, Furosemide.
The majority of these drugs are available only by prescription. Regardless of the type of problem that arises, medications should be selected by a specialist. Self-medication can only aggravate your well-being and provoke deterioration. This is why it is so important to obtain specialized medical advice.
How to quickly lower your heart rate at home
In cases of tachycardia, it is extremely important to provide assistance as quickly as possible. Complications of this condition can be quite serious: pulmonary edema and cardiogenic shock are deadly conditions that, without emergency assistance, lead to the inevitable death of the patient. Fortunately, more often the increase in heart rate occurs for physiological reasons, and in these cases you do not even have to take pills that lower your heart rate.
The first thing to do is to conduct one of the vagal tests. These are certain manipulations that cause an increase in the work of the vagus nerve, which inhibits the work of the heart:
- Valsalva maneuver - drawing air into the chest and exhaling it with the mouth and nose closed. Of course, you won’t be able to exhale, but that’s not the goal;
- deep, quick inhalation and slow exhalation;
- light massage of the eyeballs;
- washing your face with cold water or immersing your face in a basin of cold water (carry out only in the presence of another person);
- irritating the root of the tongue with a spoon, as when trying to induce vomiting (if an episode of vomiting occurs, it’s okay).
Each of the above actions can be carried out for no more than 30 seconds. In many cases, this is enough to reduce the heart rate by 20-30 beats.
However, situations also arise in which vagal tests alone are not enough, and then you have to take pills or administer medications intravenously. For tachycardia use:
- adenosine;
- beta blockers (metoprolol, bisoprolol, labetalol, etc.);
- calcium channel blockers (verapamil, amiodarone);
- cardiac glycosides (digoxin, corglycon, strophanthin);
- sodium channel blockers (procainamide, disopyramide);
- potassium channel activators (lidocaine).
All these drugs can only be used as prescribed by a doctor and in a clearly indicated dosage. The Dobrobut.com website strongly recommends not using them as self-medication - it can be dangerous!
For increased heart rate and low blood pressure, doctors usually prescribe one of the drugs that increases blood pressure along with an antiarrhythmic drug. In emergency settings, this is most often phenylephrine (Mezatone). In cases where a decrease in pressure is caused by a global disturbance of the systemic circulation (usually this occurs when the pulse increases to critical values - 150 and above), an intravenous drip infusion of dopamine, a specific agent for raising blood pressure, is possible.