Symptoms of arrhythmia
Manifestations of arrhythmia in a child may have different specifics. Each age group has its own characteristics. In newborns and infants, arrhythmia can manifest itself in the following symptoms:
- Refusal to eat.
- Slow growth.
- Intermittent sleep.
- Pallor.
- Dyspnea.
About half of all cases of arrhythmia in school-age children and adolescents are asymptomatic and are detected during routine medical examination.
In other cases, a sign of arrhythmia may be increased fatigue, exercise intolerance, pallor, decreased appetite, apathy, or, conversely, mild excitability. With a low heart rate, dizziness, pain in the heart area, and fainting may occur. Such manifestations require immediate intervention by specialists and hospitalization of the child. If you find similar symptoms in your child, make an appointment with our clinic specialists. Phone number for registration.
Heart rhythm disturbances in children
Posthypoxic complications of the cardiovascular system (CVS) in newborns range from 40 to 70% and represent an urgent problem in pediatric cardiology. In terms of frequency of occurrence, posthypoxic maladaptation states of the cardiovascular system are in second place after organic heart pathology in the neonatal period.
As a result of hypoxia in the fetus and newborn, the autonomic regulation of the heart and coronary circulation is disrupted, which can subsequently lead to the formation of persistent vegetative-visceral disorders, one of the manifestations of which is “posthypoxic syndrome of disadaptation of the cardiovascular system.”
What it is? This is a functional disorder of the cardiovascular system in a newborn and young child, which is associated with chronic antenatal (unfavorable course of pregnancy: long-term gestosis, threat of miscarriage, anemia during pregnancy, exacerbation of chronic diseases) and intranatal hypoxia (weakness of labor, premature birth, labor stimulation, cesarean section, umbilical cord entanglement). The clinical symptoms of this pathology are polymorphic, appear from the first days of life and are often disguised as other diseases. Therefore, the doctor has to carry out differential diagnosis with congenital heart defects, congenital carditis, and cardiomyopathies.
One of the common clinical variants of this syndrome in newborns is cardiac arrhythmia, most often in the form of supraventricular and ventricular extrasystole, rarely supraventricular paroxysmal tachycardia. These changes can occur even in the prenatal period and the first hours after birth.
The severity of the condition is usually due to hypoxic-traumatic damage to the central nervous system in the form of hyperexcitability syndrome, hypertensive-hydrocephalic and convulsive syndromes, impaired innervation of the heart, the condition of the myocardium (heart muscle) and hormonal status.
Extrasystole is a heartbeat that is premature in relation to the main rhythm. Depending on the location of the ectopic focus, atrial, atrioventricular and ventricular extrasystoles are distinguished. Depending on the location of the ectopic focus, atrial, atrioventricular and ventricular extrasystoles are distinguished. The problem of extrasystole attracts the attention of cardiologists due to its high prevalence and the possibility of sudden death. Ventricular extrasystole is considered the most unfavorable prognostically.
Are extrasystoles dangerous? Most arrhythmias in childhood are benign, reversible and do not pose a threat to the child’s life. In newborns and young children, they can lead to the development of arrhythmogenic cardiomyopathy or heart failure, contributing to early disability and even death. Ventricular extrasystole has an adverse effect on hemodynamics, causes a decrease in cardiac output and blood supply to the heart muscle, and as a result can lead to ventricular fibrillation and is associated with a risk of sudden death.
How do heart rhythm disturbances manifest? In approximately 40% of cases, rhythm disturbances in children are asymptomatic and are detected by chance (on an ECG), or during an objective examination during medical examination or after suffering viral or infectious diseases. Arrhythmias are manifested by palpitations, a feeling of interruptions in the work of the heart, and its freezing. In addition, the child may experience weakness, dizziness, fainting, shortness of breath, and periodically pale skin.
Examination plan for children with cardiac arrhythmias: 1. Assessment of clinical, anamnestic and genealogical data. 2. ECG examination (it is necessary to record a long ECG tape, since often NDCs are of an unstable nature and they do not have time to appear on a short tape). 3. Daily ECG monitoring. 4. Holter monitoring (HM) - long-term recording of an ECG (a day or more) on a special recorder, followed by decoding on a special analytical system. The method is available for any age, incl. and for newborn children. Today, the method is leading in the examination of children with disabilities. The uniqueness of the method is that ECG registration is carried out without restricting the patient’s free activity. The method has no contraindications. 3. Holter monitoring (HM) - long-term recording of an ECG (a day or more) on a special recorder, followed by decoding on a special analytical system. The method is available for any age, incl. and for newborn children. Today, the method is leading in the examination of children with disabilities. The uniqueness of the method is that ECG registration is carried out without restricting the patient’s free activity. The method has no contraindications. 3. Holter monitoring (HM) - long-term recording of an ECG (a day or more) on a special recorder, followed by decoding on a special analytical system. The method is available for any age, incl. and for newborn children. Today, the method is leading in the examination of children with disabilities. The uniqueness of the method is that ECG registration is carried out without restricting the patient’s free activity. The method has no contraindications. Ultrasound examination of the heart, or ECHO-cardiography (Echo-CG) 5. Consultation with a neurologist with NSG (neurosonography) and EEG (electroencephalography) of sleep 6. Consultation with an endocrinologist with an ultrasound of the thyroid gland and determination of hormonal status.
Principles of drug therapy for cardiac arrhythmias in children. Treatment of heart rhythm disturbances, especially life-threatening ones, is carried out strictly individually depending on their origin, form, duration, impact on the child’s well-being and the state of his hemodynamics. For all types of arrhythmias, cardiac and extracardiac causes should be treated simultaneously. Treatment should be comprehensive and include the prescription of neurometabolic, vascular drugs, cell membrane stabilizers and antioxidants. The interaction of these types of therapy makes it possible to ensure long-term remission and complete clinical recovery. There are situations when it is necessary to prescribe specialized antiarrhythmic therapy. Such changes include malignant arrhythmias and arrhythmogenic left ventricular dysfunction.
Clinical observation should be regular. Its frequency is determined depending on the underlying disease (rheumatism, non-rheumatic carditis, congenital heart disease, etc.), the form of arrhythmia and the characteristics of its course. Dynamic ECG recording and 24-hour ECG monitoring are required to assess the effectiveness of therapy.
Causes of arrhythmia
The causes of arrhythmia in a child are divided into several groups:
- Related to the work of the heart (cardiac causes).
These include congenital and acquired heart defects, carditis and cardiomyopathies, arterial hypertension, myocarditis, etc. This group also includes the consequences of severe infectious diseases such as tonsillitis, pneumonia, diphtheria. - Extracardiac causes.
These include diseases of the central nervous system, brain injuries and tumors, hereditary diseases, prematurity, complicated childbirth, etc. Conventionally, this group includes arrhythmia in adolescents, which is a consequence of the rapid growth of the body in conditions where the heart and blood vessels do not keep pace with the growth of muscles and skeleton.
Tachyarrhythmia
Tachyarrhythmia is a pathological condition accompanied by a disturbance in heart rhythm. If with tachycardia the heartbeats are rare and regular, then with tachyarrhythmia the rapid heartbeat is characterized by irregularity.
Causes
Tachyarrhythmia may be a consequence of the following factors:
- heart diseases - atherosclerosis, cardiomyopathy, heart failure, valve abnormalities;
- oncological and infectious diseases of the heart and blood vessels;
- allergic reactions;
- overdose of medications;
- diseases of the lungs and endocrine system;
- systematic use of alcoholic beverages and drugs.
A separate functional class of causes is distinguished, which include vegetative-vascular dystonia and electrolyte imbalance.
The following groups of medications can lead to tachyarrhythmia:
- antiarrhythmic drugs;
- sympathomimetics;
- tricyclic antidepressants;
- adenylate cyclase inhibitors.
8
24/7
Symptoms
The onset of an attack of tachyarrhythmia is accompanied by an attack of fear, which further complicates the patient’s condition. It is extremely important at this moment to calm down and relax - this will allow the condition to normalize faster.
Signs of tachyarrhythmia:
- increased heart rate more than 100 beats per minute;
- difficulty breathing, feeling of lack of air;
- dizziness;
- increased sweating;
- chest pain;
- disturbances of consciousness;
- lowering blood pressure;
- nausea;
- fainting.
An acute attack is manifested by sudden discomfort in the heart, increased heart rate, and weakness. Due to impaired blood flow, the patient may lose consciousness. In case of an acute attack of tachyarrhythmia, assistance should be provided urgently.
The chronic form manifests itself with less severe symptoms. As a rule, the disorder is manifested by the occurrence of shortness of breath and periodic pain in the sternum.
Classification
There are 2 forms of cardiac tachyarrhythmia:
- sinus;
- paroxysmal.
Sinus tachyarrhythmia is characterized by a constant disturbance of the rhythm, while paroxysmal tachyarrhythmia is manifested by sudden attacks. Paroxysmal tachyarrhythmia also has its own varieties: flutter and fibrillation of the atria or ventricles.
In the sinus form, the heart rate is recorded in the range of 80-160 beats per minute.
Depending on the location (the chamber of the heart in which the disorder is observed), the following types are distinguished:
- Supraventricular. It can be atrial and atrioventricular. In both forms, the heart rate varies from 135 to 160.
- In the ventricular form, impulses originate in the ventricles. The consequence of the ventricular form can be the development of atrial fibrillation, a dangerous condition that can be fatal.
Symptoms of supraventricular tachyarrhythmia are more often recorded in children and adolescents. In some cases, manifestations disappear on their own, without any intervention.
It is divided into 2 types:
- atrioventricular;
- atrial
With the atrioventricular type, additional impulse pathways are observed. It is characterized by rare attacks that can last a long time - up to several days.
Atrial tachyarrhythmia develops due to increased generation of impulses. Extraordinary cardiac contractions lead to the development of hypertrophy, resulting in a risk of heart attack and sudden death.
Atrial arrhythmias are in turn divided into:
- atrial fibrillation;
- atrial tachycardia.
8
24/7
Atrial fibrillation is recorded mainly in older people and is accompanied by atrial mismatch.
Ventricular tachyarrhythmia is accompanied by an increase in heart rate from 120 to 240 beats. May cause ventricular fibrillation and death.
Diagnostics
Any form of tachyarrhythmia can be recorded using an ECG. In addition to the electrocardiogram, other diagnostic methods are also used. For example, in the paroxysmal form, an ECG cannot be performed during an attack, so Holter monitoring is used. Diagnosis using Holter involves taking readings within 24 hours. Moreover, in some cases the examination lasts not one day, but several.
Additional examinations can be carried out using the following methods:
- EchoCG. A research method that allows you to analyze the condition of the chambers of the heart. This is an ultrasound diagnostic, thanks to which it is possible to identify defects that provoke tachyarrhythmia. It plays a big role in determining the etiology of the disorder.
- Examination of the condition of internal organs, liver, kidneys, thyroid gland.
- Blood tests - general and biochemistry.
- Duplex scanning of the aorta.
- Coronary angiography – studies of blood vessels.
Treatment
Tachyarrhythmia can be functional and a variant of the norm. In children and adolescents, respiratory functional tachyarrhythmia occurs, which is accompanied by an increase in heart rate during inhalation and a slowdown during exhalation. The condition is associated with the immaturity of the autonomic nervous system and goes away with age. This form does not require treatment.
Tachyarrhythmia can be short-term - it is caused by increased physical activity, overwork, lack of sleep, and caffeine abuse. It does not lead to circulatory problems.
Indications for treatment of tachyarrhythmia are:
- disturbances of heart rhythm and impulse conduction, accompanied by deterioration of local or general blood circulation;
- repeated attacks of tachycardia.
Treatment tactics are determined by the cause that led to the heartbeat disturbance. For hyperthyroidism, medications are prescribed that reduce the production of thyroid-stimulating hormone. In this case, consultation with an endocrinologist is required.
If the functioning of the central nervous system is disrupted, treatment should be carried out by a neurologist.
The manifestation of tachyarrhythmia requires an urgent determination of its form and mechanisms of development. When choosing treatment tactics, all factors influencing cardiac activity, as well as previously used treatment methods, are taken into account. First, the underlying disease is eliminated, then measures are taken to normalize the heart rate.
As a rule, calling an ambulance is not required if an attack of tachyarrhythmia with a known method of suppression begins. However, in some cases, the patient's response to a previously used and successful treatment may change. This is typical for cases of acute coronary insufficiency and acute inflammatory processes in the heart.
Drug treatment of tachyarrhythmia is carried out using the following groups of medications:
- beta blockers;
- antiarrhythmic drugs;
- anticoagulants;
- sedatives.
Antiarrhythmic drugs are cardiac glycosides. These include Digoxin, Verapamil, Lidocaine, etc. The drug can only be prescribed by a doctor; the patient is required to strictly adhere to the dosage specified by the specialist.
In cases where drug treatment is not enough, surgery and installation of a pacemaker may be performed.
Surgical intervention is performed in the form of catheter ablation. This is a minimally invasive but very effective treatment method. During the operation, part of the contractile fibers of the heart that provoked the arrhythmia is destroyed.
The type of operation also depends on the cause of the arrhythmia. For atherosclerotic vascular lesions, stenting is used. Atrial septal defects are corrected using plastic surgery. Mitral valve defects require replacement. Heart transplantation is performed for dilated cardiomyopathy.
The intervention can be carried out using a laser, electric current, or low temperatures.
Prevention
To prevent the development of tachyarrhythmia, experts recommend:
- Give up bad habits: avoid alcohol abuse and quit smoking;
- lead an active lifestyle and spend more time outdoors;
- give up strong coffee and tea;
- bring your weight back to normal, avoid overeating;
- include potassium, magnesium, calcium, and unsaturated fatty acids in the diet;
- do an ECG every year, promptly and completely treat chronic diseases.
Treatment in children
The sinus form of tachyarrhythmia in a child does not require special treatment. Sports activities are allowed in the absence of organic pathologies of the heart and diseases of the central nervous system. In the presence of serious diseases (oncological, inflammatory), mandatory treatment by a cardiologist is required.
Forecast
If untreated, tachyarrhythmia can lead to the development of the following complications:
- thromboembolism;
- arrhythmogenic shock;
- ischemic stroke;
- acute myocardial infarction.
Signs of thromboembolism are sudden shortness of breath, blueness of the skin of the neck and face.
Arrhythmogenic shock is accompanied by loss of consciousness. The person’s condition immediately becomes grave. There is a sharp drop in blood pressure and the skin turns white.
With moderate hemodynamic disturbances, the following may develop:
- cardiac asthma;
- angina attacks at rest;
- decrease in cardiac output in combination with oliguria and decreased temperature of the extremities.
The sinus form of tachyarrhythmia is considered the safest. A favorable prognosis is also observed with the paroxysmal form of tachyarrhythmia and the chronic form of atrial fibrillation.
The ventricular form can lead to sudden death. Therefore, it is necessary to consult a specialist in time for qualified treatment.
8
24/7
Diagnosis of arrhythmia
To make an accurate diagnosis, consultation with a pediatric arrhythmologist or pediatric cardiologist is necessary. The initial examination by a specialist includes:
- Studying the medical history.
- Carrying out a full examination (palpation, percussion, auscultation).
If an arrhythmia is suspected, the doctor will refer the child for instrumental diagnostics:
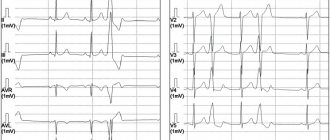
- Electrocardiography
is a universal method that allows you to evaluate the work of the heart in a specific time period. - Daily Holter monitoring.
A more accurate method compared to conventional electrocardiography, as it records the work of the heart over a long period of time (days), including sleep, physical activity, various periods of activity, etc. - Load tests.
This is an analysis of cardiac activity during physical activity of varying intensity.
This method can only be used with older children. After making a diagnosis, an arrhythmologist or pediatric cardiologist may prescribe examinations aimed at identifying the causes of the disease:
- EchoCG
(echocardiography or ultrasound of the heart). Allows you to identify organic causes of the disease, for example, heart defects, tumors, etc. - Radiography.
This method is aimed at identifying extracardiac causes of arrhythmia, for example, pathology of the spine, large vessels. - EEG.
Electroencephalography is indicated in cases of suspected connection of arrhythmia with brain diseases.
The SM-Doctor clinic for children and adolescents is equipped with only modern diagnostic equipment, which allows our specialists to make an accurate diagnosis and prescribe timely treatment for the disease.
Treatment of arrhythmia
Treatment methods for arrhythmia in children depend on the causes and variant of the identified disorders.
Only an arrhythmologist (pediatric cardiologist) makes a decision on the need to treat arrhythmia. Self-treatment of the disease is strictly prohibited. This threatens the child with complications and the development of dangerous symptoms. However, given the often asymptomatic nature of many rhythm disturbances, including life-threatening ones, parents themselves should pay great attention to the problem.
To make an appointment with children's ari, fill out the online form or call us at +7 (495) 292-59-86.