Sign up
+7
Cardiac surgery is one of the most difficult operations. The aortic valve replacement uses a miniature part created in a high-tech laboratory. Installing such a prosthesis is a painstaking and extremely responsible task, which only an experienced surgeon can handle. The operation requires serious preparation, and the recovery period also requires effort on the part of the patient.
When is valve replacement required?
The heart is responsible for delivering blood and oxygen to all tissues of the body. Any disturbances in the functioning of the organ inevitably have a negative effect on the body and require treatment. Often the problem can be solved conservatively, that is, without resorting to invasive intervention. But this does not always happen, and in some cases surgical replacement of the aortic valve cannot be avoided. The main problems of the aortic valve include:
- Congenital and acquired defects. This category includes any changes that interfere with normal blood flow and increase the workload of the heart.
- Valve stenosis, in which the ejection of blood into the aorta is impeded.
- Rheumatic diseases, streptococcal infection.
- Aneurysm, aortic dissection.
- Change in shape, valve damage, calcification, sagging valves.
- The valve does not close tightly, blood flows in the opposite direction.
- Inflammation.
Make an appointment with a specialist without queues, at a convenient time
Sign up
+7
When the pathology is at an early stage of development, it can often be eliminated without surgery. In serious cases, when medications cannot solve the problem, surgery is used. An artificial valve made in the laboratory, as well as an element of the patient’s own tissues, can be installed. The second option is cheaper, since you do not need to purchase an expensive prosthesis.
Department of surgical treatment of congenital heart defects (CHD)
Congenital heart defects (CHD) are a large group of anomalies of the intrauterine development of the heart and large vessels flowing into or leaving its cavities, varied in formation and anatomy.
CHD incidence statistics
According to various sources, the incidence of congenital heart disease varies from 2 to 15 cases for every 1000 newborns. In 2021, among more than 1.3 million newborns, about 12 thousand children with congenital heart disease were registered.
Compared to statistics 10 years ago, the frequency of detection of congenital heart disease in newborns has increased from 6 to 9 cases per every 1000 infants born, which is apparently due to improved means of early diagnosis of this serious and often life-threatening group of diseases in childhood.
Despite the fact that modern methods and technical capabilities of ultrasound examination (echocardiography) will make it possible to detect congenital heart disease in the fetus starting from 12-14 weeks of pregnancy with a high degree of probability (up to 96%), nevertheless, cases of late detection of this pathology are recorded both among children, as well as among adults.
At the end of 2021, more than 573 thousand patients (children and adults) with an established diagnosis of congenital heart disease were registered in Russia (population of about 147 million people). However, there is a high probability that the actual number of such patients may be higher, and the number of annually registered cases of this diagnosis will increase.
Survival prognosis
Undoubtedly, the natural (without medical intervention) course of the vast majority of various congenital heart diseases, as a rule, has an unfavorable prognosis and leads to a reduction in the duration and quality of life of the patient, often quite significantly. Up to 90% of newborns with so-called “critical congenital heart disease” do not survive beyond 1 year. Many of them die within the first weeks of their lives. According to statistics, congenital heart defects account for about 10% of the causes of infant mortality in Russia.
Causes of congenital heart disease
Among the most likely causes of the formation of congenital heart disease are genetic and chromosomal aberrations, viral infections of the mother during pregnancy, chronic endocrine and metabolic diseases, bad habits (smoking, drinking alcohol, etc.), teratogenic and mutagenic adverse environmental factors.
There are a great many congenital anomalies of the development of the heart and great vessels. Conventionally, the entire set of congenital heart disease can be subdivided depending on the age at which clinical manifestations (symptoms and consequences) are most pronounced and prognostically significant.
| Types of congenital heart disease | Age at which surgical treatment is usually necessary |
| Newborn period |
| First year of life |
| Over a year old |
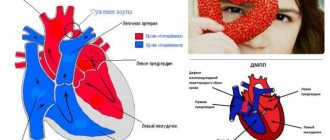
Some congenital heart diseases are characterized by severe disturbances of central hemodynamics soon after birth, forcing surgical treatment to begin already in the neonatal period (for example, simple transposition of the great arteries or obstructive forms of total anomalous drainage of the pulmonary veins).
Transposition of the great arteries
Total anomalous pulmonary venous drainage
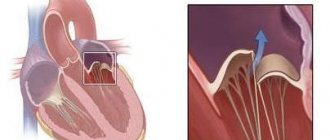
Other congenital heart defects occur with clinical compensation in the first few weeks or months of life, manifesting closer to the second half of life (ventricular or aortic-pulmonary septal defect, atrioventricular canal, SBUG).
Common atrioventricular canal
Ventricular septal defect
Common truncus arteriosus
There are congenital anomalies that do not appear clinically for a long time and are benign, which makes it possible to delay their surgical treatment until the second year of life and even later (atrial septal defect, partial anomalous drainage of the pulmonary veins).
Atrial septal defect
Moreover, there are a number of congenital heart defects, the correction of which is advisable to delay within the duration of the clinical compensation period in order to achieve better treatment results (corrected transposition of the great arteries, compensated forms of Ebstein's anomaly, moderate coarctation of the aorta).
Coarctation of the aorta
It should also be noted that the same nosological form of congenital heart disease, depending on the specific anatomy, can become a reason for surgery at different age periods. For example, a simple transposition of the great arteries forces an arterial switch operation to be performed in the first two weeks of life, whereas in combination with a large ventricular septal defect, the same anomaly can be operated on at the age of two months or older. Extreme forms of Ebstein's anomaly with hemodynamic atresia of the pulmonary artery and ductus-dependent pulmonary blood flow are “critical congenital heart disease of the newborn period.”
“Critical defects of the newborn period” account for about 30% of identified congenital heart defects and require immediate surgical care in the first weeks, or even days, of a child’s life.
Previously, this group of diseases was identified with a pathology incompatible with life. However, the capabilities of modern medicine have made it possible to achieve impressive early and long-term results in the treatment of many of this group of congenital heart diseases.
Critical UPS
Hypoplastic left heart syndrome
Pulmonary valve atresia
Tricuspid valve atresia
It is important to remember that a number of congenital heart abnormalities cannot be eliminated immediately, within the framework of one surgical operation. In such cases, to achieve optimal treatment results, it is divided into several stages, or phases, each of which is performed at different ages, starting from infancy. Also, it is almost never possible to exclude the possible need to perform additional surgical intervention even after a previously performed radical (that is, definitive) correction of a heart defect.
All operations for congenital heart disease can be divided into 4 categories:
| Radical operations (corrections) | When complete and final elimination of congenital heart disease is achieved and the child’s heart acquires an anatomical structure corresponding to a healthy heart or close to normal anatomy. Intracardiac circulation after such operations naturally becomes physiological (that is, normal). After treatment, the patient’s rate of development, quality and life expectancy does not differ from healthy peers and usually only needs preventive outpatient monitoring. As a rule, disability is removed. |
| Hemodynamic corrections | When the intracardiac circulation, as well as the anatomical structure of the heart, upon completion of treatment cannot be called “corresponding to a healthy heart.” However, such a correction ensures hemodynamics close to physiological, allowing the child to live, develop, and in the future, successfully adapt to society and create his own family. A person’s physical capabilities may be somewhat limited, but the disability is not completely removed. |
| Preparatory (intermediate) palliative operations | They are interventions that aim to prepare the heart and the body as a whole for subsequent radical or hemodynamic correction. There may be several such operations. Patients after such operations can be temporarily discharged from the hospital, but require systematic outpatient monitoring in order to monitor the clinical condition, correct drug therapy and determine the timing of the next hospitalization for diagnosis and continuation of surgical treatment |
| Definitive palliative (life-prolonging) operations | Currently, they are very rare and are performed on patients with incurable (inoperable) complex forms of cardiac anomalies or their incurable complications. Such operations are sometimes called a “bridge” to heart transplantation. |
From a prognostic point of view, all congenital heart defects can be divided into anomalies with a favorable prognosis and defects with an unfavorable prognosis.
. The latter most often represent a combination of multiple congenital heart defects (often combined with malformations of other organs, multiple manifestations of dysembryogenesis and syndromic forms of genetic anomalies), which are not subject to radical correction and predetermine, even if hemodynamic or palliative surgery is performed, a low quality of the patient’s future life, limitation of its duration, deep disability and limited social adaptation. Patients with such anomalies are potentially considered candidates for heart or heart-lung transplantation. In cases of early prenatal (intrauterine) diagnosis of congenital heart disease with an unfavorable prognosis, the possibility of terminating the pregnancy for medical reasons should be considered in connection with the detection of a congenital heart defect incompatible with life in the fetus.
Classification of congenital heart disease
CHD can also be classified into simple (the patient has a single anomaly) and complex (a combination of several anomalies). In the WHO International Classification of Diseases, some frequently combined anomalies of heart formation are often combined into one nosological unit with appropriate coding, for example, “hypoplastic left heart syndrome” or “tetralogy of Fallot.”
Tetralogy of Fallot
Clinical manifestations (symptoms) of congenital heart disease
are not only very diverse, but also have a characteristic spectrum inherent in a specific age period of their natural course. For example, a large ventricular septal defect usually does not cause symptoms in the first few months of life due to the physiology of the lungs in newborns and infants. By six months of life, the child develops symptoms of heart failure (frequent colds, poor appetite, decreased exercise tolerance, shortness of breath, underweight, anemia, sleep disturbances) caused by excess blood flow in the lungs and overload of the left chambers of the heart. However, later, by 2-3 years of age and older, as irreversible dangerous sclerotic changes develop in the small vessels of the lungs, these symptoms spontaneously regress - a period of imaginary well-being begins. During this period, the patient is either conditionally operable or not operable at all. Subsequently, the clinical picture is characterized by symptoms of right ventricular circulatory failure and secondary deficiency of pulmonary blood flow against the background of sclerosis and obstruction of small vessels of the lungs.
Division of defects into “pale” and “blue” (cyanotic)
, widespread in popular scientific literature and online resources, is very conditional in nature, since it does not have a clear correlation with the hemodynamic patterns of the natural course of congenital heart disease and does not carry any prognostic value. Thus, two anomalies “simple transposition of the great arteries” and hypoplastic right heart syndrome are cyanotic congenital heart disease, but in the first case the possibility of radical correction predetermines a favorable prognosis, in contrast to the second of these congenital heart disease.
Congenital heart disease in adult patients is included in a special group
— corrected or uncorrected congenital heart disease in persons 18 years of age and older.
They are usually divided into primary and secondary. Primary
- a set of anomalies with a relatively favorable natural course, allowing one to survive childhood, first identified at the age of over 18 years or identified in childhood, but recognized as incurable (incurable).
This is a smaller cohort of patients. Secondary
– in the so-called “GUCH-patients” (the larger of the two cohorts). They are represented by a wide range of congenital heart anomalies previously operated on in childhood.
On the basis of the clinical departments of our Center, specialized in the treatment of patients with congenital heart disease, all types of open surgical, minimally invasive surgical (thoracoscopic) and X-ray endovascular interventions (including hybrid) are performed for a wide variety of congenital anomalies and tumor diseases of the heart and great vessels .
The center is equipped with all the necessary modern equipment for timely and complete diagnosis of congenital heart disease, including prenatal (intrauterine) diagnostics. Every year, about 3,500 patients with congenital heart disease receive the necessary surgical care at our Center. More than 900 X-ray endovascular procedures are performed for congenital anomalies of the heart and great vessels.
What types of valves are there?
Three types of elements can be used to replace an unhealthy valve:
- Biological. They suggest recreating a new valve from the patient’s own tissues. Such a valve will last about 10-15 years, after which the operation will need to be repeated. This is due to the gradual wear and tear of the element and its inevitable degenerative changes. With this approach, anticoagulants need to be taken only for the first six months after surgery.
- Mechanical. Such a valve is manufactured in a laboratory and requires constant use of anticoagulants (for the entire life of the patient). Such prostheses are installed mainly in patients who have not reached old age.
- Donor. This option is used only in extreme cases, as there is a risk of rejection of donor tissue by the patient's body. The outcome of such an operation is difficult to predict, and the possibility of complications cannot be excluded. In order for the valve to take root, doctors need to carry out therapy that suppresses the recipient’s immunity so that the immune system does not begin to fight the foreign element. As with the installation of an artificial valve, the patient is advised to take lifelong anticoagulants to exclude the possibility of thrombus formation.
- Available: doctor’s appointment from 1500 rubles
- Convenient: open daily from 8:00 to 21:00
- Quickly: we will carry out all the diagnostics at the first appointment
- Complete: has all the necessary equipment
Preparation for lower extremity vein bypass surgery
Before surgery, the patient should undergo a number of preparatory measures:
- Comprehensive examination of the cardiovascular system (narrowed blood vessels can be in all parts of the body);
- Take a general blood test;
- Get an ECG and ultrasound of blood vessels.
It is important to tell your doctor right away what medications you are taking. Based on this data, the phlebologist will determine which medications you should continue to use and which ones you should exclude before surgery.
What types of operations are used
Aortic valve reconstruction or replacement can be performed in two ways:
- On an open heart.
- Minimally invasive method.
Modern cardiac surgery actively uses methods that make it possible to replace heart valves without cutting the chest. An operation without an opening will cost more than a classic open one. This approach reduces the likelihood of risks and facilitates the recovery period. Access can be through an artery in the shoulder or leg using a catheter. Local or general anesthesia is required, the total time of the operation using a catheter is about one to one and a half hours.
Abdominal surgery with an incision in the chest lasts longer and is cheaper compared to minimally invasive surgery. During valve replacement, the patient is connected to an artificial circulatory system. The risk for the patient is slightly higher than with the endoscopic method, but there is no risk of deformation of the conducting vessels.
Modern techniques are available in clinics in Israel and Germany.
Examples of prices for cardiac bypass surgery
For a foreigner who needs to undergo surgery with plastic surgery of 3 valves in Moscow from one of the best specialists, it will cost about a million rubles, excluding rehabilitation costs. For a healthcare worker in Russia, the same procedure will cost about 700,000 , also excluding rehabilitation. Coronary artery bypass surgery on a living beating heart (without artificial blood flow) for Russian citizens will cost about 200,000 rubles , for foreigners approximately 350,000 .
Postoperative period
The recovery period is the most important stage, which has its own characteristics. For the first time after replacing the valve, physical activity and strong psychological experiences are prohibited. Caution must be exercised for at least three years after the intervention. Professional athletes can return to full training only after six years. Taking anticoagulants prescribed by a doctor is a must. It is also very important to regularly check the condition of the body and monitor for possible concomitant pathologies.
In fact, the valve itself will not affect the patient's future health in any way. If irreversible changes have occurred, the patient needs constant monitoring by a cardiologist.
General multicomponent effect of laser therapy
In general, the effect on the heart and blood vessels when using laser irradiation consists of the following improvements:
- Relieving spasms
- Expansion and strengthening of blood vessels
- Improving blood microcirculation
- Reducing blood viscosity and increasing coagulability (the risk of blood clots is reduced, and microthrombi are resolved)
- Increased hematopoiesis
- Normalizes heart rate and reduces the likelihood of arrhythmias
- Increased cardiac contractile function
- Reduction in blood cholesterol, normalization of many blood parameters
- Increasing the bactericidal properties of bloodReducing ischemic zones
- Improving oxygen metabolism
- Increased oxygen content in tissues