What does ESR show?
ESR is not a specific indicator for any particular disease, that is, it is impossible to establish a specific diagnosis based on its increase.
This test is considered useful for identifying hidden forms of various diseases and determining the activity of chronic inflammatory conditions. ESR can also serve as an indicator of the effectiveness of therapy.
However, measuring ESR is in no way used to diagnose cancer.
What are the reasons for increased ESR?
An elevated ESR is a sign of any disease associated with significant tissue damage, inflammation, infection, or malignant cancer.
In all infectious and inflammatory diseases, the immune system responds by increasing the production of immunoglobulins. This in turn increases the tendency of red blood cells to aggregate and form red blood cell columns. Repeated studies of ESR make it possible to evaluate the dynamics of the infectious process and the effectiveness of treatment.
Also, the ESR is influenced by many other factors that determine the physicochemical state of the plasma: viscosity, electrolyte composition of the plasma, the ratio between cholesterol and lecithin in the plasma, the content of acids in it, etc.
The main reasons for increasing ESR:
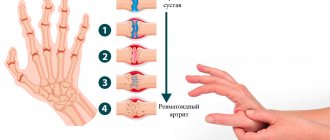
- Any inflammatory process in the body, for example, arthritis, accelerates ESR due to the production of large amounts of “acute phase proteins of inflammation.”
- A number of diseases in which tissue damage occurs - myocardial infarction, destructive pancreatitis, etc.
- Surgical interventions are also accompanied by an increase in ESR.
- A decrease in the number of red blood cells in patients with anemia also leads to an increase in ESR.
- All infectious diseases are usually accompanied by an acceleration of ESR.
- Obesity.
- An error during a blood test, for example, incorrect temperature conditions.
- An increase in ESR is observed in elderly patients.
Yu.V. Pervushin, V.V. Velkov*, L.S. Putrenok.**
State Educational Institution of Higher Professional Education Stavropol State Medical Academy of Roszdrav, Department of Clinical Laboratory Diagnostics FPO, *CJSC "DIAKON", Pushchino, Moscow Region, **Stavropol Regional Clinical Diagnostic Center.
Why, doctors, even in modern medical institutions, cannot part with the tradition of determining ESR , despite numerous scientific data that cast doubt on the accuracy and diagnostic value of this test?
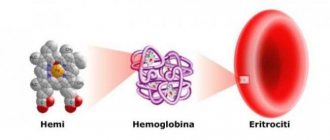
Erythrocyte sedimentation rate (ESR, previously erythrocyte sedimentation reaction - (ROE) is a nonspecific laboratory blood indicator; a change in ESR can serve as an indirect sign of a current inflammatory or other pathological process. For more than a hundred years, this test, despite the fact that it is nonspecific, has been used for quantitative characteristics of the severity of inflammatory processes caused by infections, various inflammations, and the development of neoplasms. However, although inflammation is the most common cause of accelerated erythrocyte sedimentation, an increase in ESR can also be caused by other, including not always pathological, conditions. Thus, the results ESR determinations can be considered reliable only when no parameters other than those expected influence the indicator being studied. In fact, too many factors influence the results of this test and therefore its clinical significance should be reconsidered. The main effect is on the erythrocyte sedimentation rate, suspended in plasma, affects the degree of their aggregation. This process is quite complicated. It depends on many factors and the leading role in it belongs to three main ones - those influencing the aggregation of erythrocytes, these are: 1) surface energy of the cells, 2) cell charge and 3) dielectric constant. The latter indicator is a characteristic of plasma associated with the concentration of asymmetric molecules. An increase in the content of such molecules (proteins) leads to an increase in the strength of the bonds between red blood cells, which, in turn, leads to agglutination and clumping (formation of columns) of red blood cells and, thus, to a higher rate of their sedimentation. However, these main factors, in turn, depend on many physicochemical changes occurring in the body (Table 1).
Table 1 The influence of some physicochemical factors on the ESR value (according to G.E. Roitberg and A.V. Strutynsky, 1999)
| Basic physical and chemical factors | The most common pathological changes | Change in ESR |
| Fibrinogen | Increase | Increase |
| α-globulins | Increase | Increase |
| γ-globulins | Increase | Increase |
| Paraproteins | Increase | Increase |
| Albumen | Increase | Increase |
| Bile pigments | Increase | Decrease |
| Bile acids | Increase | Decrease |
| Changes in blood pH | Decrease (acidosis) Increase (alkalosis) | Decrease Increase |
| Blood viscosity | Increase Decrease | Decrease Decrease |
| Red blood cell count | Increase (erythrocytosis) Decrease (anemia) | Decrease Increase |
In addition to these factors, laboratory-methodological, biological and iatrogenic influences can change the ESR indicator (see Table 2).
Table 2 Factors causing an increase in ESR (L.I. Dvoretsky, 1998)
| Laboratory and methodological | Biological | Iatrogenic |
| Inaccurate amount of citrate | Macrocytosis | Dextrans |
| Standing the sample with citrate for more than 4 hours | Anemia | Phenothiazine |
| Standing the sample in the light | Anti-erythrocyte antibodies | a-Methyldopa |
| Keeping the sample warm | Hyperproteinemia | Vitamin A |
| Wet capillary | Dysproteinemia | Contraceptives |
| Standing the sample at an angle | Hyperfibrinogenemia | g-globulin |
| Hyperlipidemia | Deseril | |
| Alkalosis | ||
| Pregnancy | ||
| Elderly age |
What causes false results when measuring ESR?
False increase in ESR - summing up the most common factors and common clinical situations affecting ESR, we can conclude that the clinician most often encounters a false increase in ESR when:
- anemia with normal erythrocyte morphology
- an increase in plasma concentrations of all proteins except fibrinogen, M-protein, macroglobulins and erythrocyte agglutinins
- renal failure
- use of heparin when drawing blood
- hypercholesterolemia
- extreme obesity
- pregnancy (by the way, the determination of ESR was originally used to establish pregnancy)
- female
- elderly age
- technical errors during testing (deviation of the test tube from the vertical position increases the ESR, while an angle of 3° from the vertical line can lead to an increase in ESR by up to 30 units).
A false decrease in ESR can occur when:
- increase in red blood cell count
- significant increase in white blood cell count
- DIC syndrome (due to hypofibrinogenemia)
- dysfibrinogenemia
- afibrinogenemia
- significant increase in the level of bile salts in the blood plasma
- congestive heart failure
- valproic acid
- low molecular weight dextran
- cachexia,
- lactation.
A false decrease in ESR can occur due to morphological changes in red blood cells: red blood cells of an abnormal, unusual shape prevent the formation of columns and lead to a decrease in ESR. This is exactly how they affect erythrocyte aggregation, reducing ESR: 1) spherocytosis, 2) anisocytosis, 3) poikilocytosis. I wonder how to objectively assess what happens in iron deficiency anemia, when a decrease in the number of red blood cells accelerates the ESR, and aniso- and poikilocytosis slow it down, and how to correctly calculate the relative importance of these factors?
The most common technical errors in determining ESR ESR decreases as the temperature in the laboratory decreases; to determine ESR, blood obtained more than 2 hours before the test cannot be used: during storage, red blood cells take on a spherical shape and ESR decreases. It is also believed that the three most common factors that underestimate ESR in patients are: 1) blood thickening, 2) acidosis, 3) hyperbilirubinemia. Based on the above, it should be especially emphasized that for any diseases that are, in principle, characterized by an increase in ESR, this indicator at certain stages of the development of the pathological process may in fact not be increased and lead to erroneous conclusions if at least one of the following factors: 1) blood thickening, 2) a state of acidosis or hyperbilirubinemia (jaundice), 3) cardiac decompensation, 4) a state of ketoacidosis in diabetes mellitus and 4) many other changes in the patient’s body. Thus, it is obvious that doctors who require the determination of ESR rely more on the traditions of medicine than on the actual reliability of this method.
But the doctor urgently needs to assess the severity of the inflammatory reaction. The best method for this assessment is to measure the concentration of C-reactive protein, the main acute phase protein (APP) of inflammation. BOP levels during the inflammatory process change to varying degrees and depending on the stage of inflammation (Fig. 1). Assessing this group of indicators based on the dynamics of BEF levels, the degree of increase in these levels, their specificity, and, finally, the reliability of their laboratory determination, we can clearly name the most “worthy candidate for filling the position” ESR - SRB. Like all BOPs, CRP is synthesized in the liver under the influence of interleukins, oncostatin M, with the modulating effects of other interleukins and tumor necrosis factor. CRP is considered one of the “main” BFs of inflammation in humans, as it increases very quickly (in the first 6-8 hours) and very significantly (20-100 times, sometimes 1,000 times). But is measuring CRP levels really better than measuring ESR? Table 3 compares the results of ESR and CRP measurements, from which it follows that CRP is the most specific and most sensitive qualitative and quantitative laboratory indicator of inflammation and necrosis. CRP concentrations change rapidly in response to increasing or decreasing severity of inflammation. That is why measurement of CRP levels is widely used to monitor and control the effectiveness of therapy for bacterial and viral infections, chronic inflammatory diseases, cancer, complications in surgery and gynecology, etc.
Rice. 1 . Changes in the concentration of BOP during moderate inflammation (Shevchenko O.P., 2005)
CRP levels in various inflammatory processes
Up to 10-30 mg/l – CRP increases with viral infections, tumor metastasis, sluggish chronic and some systemic rheumatic diseases.
to 40-100 mg/l (and sometimes up to 200 mg/l) with: 1) bacterial infections, 2) exacerbation of some chronic inflammatory diseases and 3) tissue damage (surgery, acute myocardial infarction). With effective treatment of bacterial infections, the level of CRP decreases the next day; if not, more effective antibacterial treatment is necessary.
Up to 300 mg/l or more - CRP increases with: 1) severe generalized infections, 2) burns, 3) sepsis, which increase CRP almost prohibitively.
Table 3 What determines changes in ESR and CRP levels (T. Husain, et al. 2001)
| The measurement result depends on: | ESR | SRB |
| Paula | Yes | No |
| Age | Yes | No |
| Pregnancy | Yes | No |
| Temperatures | Yes | No |
| Medicines (steroids, salicylates) | Yes | No |
| Smoking | Yes | No |
| Plasma protein levels | Yes | No |
| Erythrocytes – number (Ht) Morphology Aggregation | Yes Yes Yes | No no no |
| Laboratory characteristics of indicators | ||
| Rate of increase in response to disease | Moderate | High |
| Normal values | Wide | Narrow |
| Specificity | Moderate | High |
| Sensitivity | Moderate | High |
| Reproducibility | Low/moderate | High |
| Identifying errors while performing analysis | Complex | Lung |
| Duration | > 60 min | < 20 min |
| Relative price | x 1 | x 2-3 |
If neonatal sepsis is suspected, a CRP level of more than 12 mg/l is an indication for the immediate initiation of antimicrobial therapy (in some newborns, a bacterial infection may not increase CRP). Neutropenia: In an adult patient, a CRP level greater than 10 mg/L may be the only objective indication of a bacterial infection. Postoperative complications: if CRP continues to remain high (or increases) within 4-5 days after surgery, this is an indication of the development of complications (pneumonia, thrombophlebitis, wound abscess). After surgery, the higher the level of CRP, the more severe the operation and the more traumatic it is. Concomitant bacterial infections: in any disease, the addition of a bacterial infection increases CRP to more than 100 mg/l. Tissue necrosis causes OF, similar to that caused by a bacterial infection. Such OF is possible with: 1) myocardial infarction, 2) tumor necrosis - tissues of the kidneys, lungs, and large intestine.
Monitoring CRP when monitoring the effectiveness of treatment for various diseases Systemic rheumatic diseases sharply increase the level of CRP: a decrease in CRP in rheumatoid arthritis indicates the effectiveness of therapy. In systemic vasculitis, CRP monitoring allows minimizing steroid doses. In inflammatory diseases of the gastrointestinal tract: 1) a strong increase in CRP causes Crohn's disease, 2) a slight increase in CRP is observed in ulcerative colitis and 3) in functional disorders of the gastrointestinal tract, CRP is usually not elevated. In secondary amyloidosis, increased CRP correlates with the development of renal complications. In cardiac transplant rejection, high CRP is associated with infectious complications but does not indicate rejection per se. In kidney transplant rejection, severe OF is one of the early indicators of rejection.
Increasing CRP levels in oncological diseases If, with a high level of CRP, there are no obvious signs of inflammation or necrosis, the patient should be examined for the presence of oncological diseases!
With malignant tumors, various changes in the level of CRP are possible, which depends on: 1) the addition of infection, 2) tissue necrosis, 3) dysfunction of organs due to obstruction of the respiratory tract or gastrointestinal tract, 4) the influence of immunosuppression and chemotherapy. Strong OF and increased CRP are observed in necrosis of solid tumors. Lymphomas are rarely accompanied by tissue necrosis and changes in the spectrum of plasma proteins. In myeloma, a very strong acute phase is a poor prognostic sign.
Highly sensitive measurement of CRP and assessment of cardiovascular risks A new technological solution - highly sensitive immunoturbidimetric determination of CRP or hs-CRP (hs - high sensitivity) with latex enhancement made it possible to increase the sensitivity of the analysis by 10 times and bring the lower limit of determination to 0.03-0.05 mg/l. The basic level of CRP is its level in the plasma of practically healthy people: 1) without an acute inflammatory process, 2) without exacerbation of a chronic disease, 3) without previous operations, 4) without injuries, 5) in the absence of tissue necrosis and 6) without oncology . When measuring hs-CRP, it was changes in its basic concentrations that made it possible to assess low-grade inflammatory processes, in particular in the vascular endothelium, which are associated with the development of atherosclerosis and its complications. The importance of determining hs-CRP in atherosclerosis became clear after numerous prospective studies indicating that CRP in atherosclerosis is not just a marker of inflammation, but an active participant in the development of this disease at all stages of pathogenesis.
So, what do changes in baseline CRP concentrations indicate? As a result of numerous studies it has been established that measurements of basic levels of CRP have prognostic value, which allows one to assess the degree of risk of developing: 1) acute myocardial infarction, 2) cerebral stroke, 3) sudden cardiac death in individuals who do not suffer from cardiovascular diseases (Table 4 ).
Table 4 Risk of developing vascular complications depending on the level of hs-CRP (O.P. Shevchenko, 2005)
| hs-CRP level, mg/l | Risk of developing vascular complications |
| < 1 | minimum |
| 1,1-1,9 | short |
| 2,0-2,9 | moderate |
| > 3 | high |
- It should be taken into account that CRP levels below 10 mg/l are significant for stratifying the risk of vascular complications.
- If the level of CRP is above 10 mg/l , then obviously this is associated with acute inflammation, chronic disease, etc.
- The baseline level of CRP is measured no earlier than 2 weeks after the disappearance of symptoms of any acute disease or exacerbation of a chronic disease.
When determining the risk of atherogenesis, hs-CRP measurements are performed in duplicate at a desired interval of 2 weeks. The greatest prognostic significance for assessing the risk of developing cardiovascular diseases is the joint determination of hs-CRP and lipid metabolism parameters. In acute coronary syndrome, destabilization of atheroma and thrombus formation are associated with inflammatory processes. With unstable angina, elevated levels of CRP occur much more often (in 70% of patients) than with exertional angina (in 20% of patients). In addition, in patients with unstable angina who developed acute myocardial infarction, CRP was elevated (>3 mg/l) in almost all (98%) patients. When stratifying the risk of early (up to 14 days) mortality in patients with unstable angina and acute myocardial infarction, the most informative is the combined determination of hsCRP and troponin T. An increase in both of these risk markers (hsCRP > 1.55 mg/l, troponin T > 0.1 mg /l) indicates a high risk of death. hsCRP levels <1.55 mg/l and troponin T <0.1 mg/l indicate minimal risk. By quitting smoking, regular physical activity, moderate alcohol consumption, and treating obesity, the baseline hsCRP level and, at the same time, coronary risk decrease. Taking aspirin to prevent vascular complications is effective only in individuals with initially elevated baseline hsCRP levels.
hsCRP and cardiac surgery risk assessment In patients undergoing coronary artery bypass grafting, elevated hsCRP is associated with a risk of early delayed complications. In angioplasty with coronary artery stenting in patients with coronary artery disease, high hsCRP is associated with a higher risk of subsequent restenosis. The association of hsCRP with the risk of complications after invasive treatment of coronary artery disease is evidenced by the following: only 12% of patients with coronary artery restenosis that developed after angioplasty with stenting had hsCRP <5 mg/l (in combination with a normal ceruloplasmin level, >2 g/l) . All patients with hsCRP > 9 mg/l (in combination with a reduced level of ceruloplasmin <0.2 g/l) developed restenosis of the coronary arteries.
hsCRP and risk assessment of pregnancy pathologies Measuring hsCRP makes it possible to assess the risk of spontaneous abortions in pregnant women, which may be associated with low-grade inflammatory processes. In full-term pregnancy, the CRP level is usually 2.4 mg/L. Women with elevated CRP levels during weeks 5–19 of pregnancy (3.2 mg/L) are at high risk of preterm birth. And with - with CRP - 8 mg/l and higher, the risk of premature birth increases by 2.5 times, regardless of other risk factors.
ESR and/or CRP? Unfortunately, at present, it is most likely impossible to completely abandon the definition of ESR and switch to measuring CRP everywhere. The determination of ESR cannot be replaced in local hospitals and outpatient clinics. But in larger and more modern medical institutions, the measurement of ESR should gradually give way to the determination of CRP. It is urgently necessary to carry out a gradual planned transition to the quantitative determination of CRP and use its indicator: firstly, to assess the severity of inflammatory processes (the range of measured concentrations is from 10 mg/l and above) and, secondly, to assess the risks associated with low-grade inflammatory processes (range of measured concentrations – less than 10 mg/l).
CRP in the inflammatory range should be measured for
- determining the severity of inflammatory processes caused by bacterial and viral infections
- monitoring changes in the severity of such processes in order to correct their therapy
- monitoring the patient's condition after surgery,
- monitoring the process of rejection of a transplanted kidney
- monitoring the patient's condition after a heart attack or ischemic stroke.
Highly sensitive CRP measurement should be used to assess risks:
- occurrence and progression of atherosclerosis
- acute coronary events
- risks of ischemic strokes
- assessing the risks of pregnancy pathologies.
Literature: 1. Amelyushkina V.A. ESR - methods of determination and clinical significance. // In the book. Laboratory diagnostics / ed. V.V. Dolgov, O.P. Shevchenko. – M.: Publishing house. "Reafarm". – 2005.– P. 107-109. 2. Shevchenko O.P. Characteristics and clinical significance of proteins in the acute phase of inflammation.// In the book. Laboratory diagnostics / ed. V.V. Dolgov, O.P. Shevchenko. – M.: Publishing house “Reapharm”. – 2005. – P.137-143 3. Dvoretsky L.I., Features of laboratory diagnostics in geriatrics.// Clinical laboratory diagnostics, 1998, No. 1, P. 25-32. 4. Karpov Yu.A., Sorokin E.V. Primary prevention of cardiovascular diseases: new guidelines? RMJ, Volume 10 No. 19, 2002 5. Roitberg G. E., Strutynsky A. V. Laboratory and instrumental diagnosis of diseases of internal organs. 1999. Ed. "Binomial". – 622 p. 6. Sumarokov A.B., Naumov V.G., Masepko V.P., C-reactive protein and cardiovascular pathology. 2006, Triad. 7. Albert C, Rifai N, et al; Prospective Study of C-Reactive Protein, Homocysteine, and Plasma Lipid Levels as Predictors of Sudden Cardiac Death; Circulation 2002;105(22):2595-2599 8. Jurado RL Why Shouldn't We Determine the Erythrocyte Sedimentation Rate? // Clinical Infectious Diseases, 2001; 33: 54854-9 9. Ridker P, Rifai N, et al; Comparison of C-Reactive Protein and Low-Density Lipoprotein Cholesterol Levels in the Prediction of First Cardiovascular Events N Engl J Med 2002, 14;347(20):1557-1565 10. Pitiphat W, et al. Plasma C-reactive protein in early pregnancy and preterm delivery. Am J Epidemiol. 2005;162(11):1108-1113.
How to calculate the individual ESR norm in elderly patients?
The easiest way is to use Miller's formula:
For example, the permissible ESR limit for a 60-year-old woman is: (60 years + 10): 2 = 35 mm/hour
When changes are detected in a clinical blood test, the first thing the patient does is go to a general practitioner. A useful point is that ESR is included in the Clinical Blood Test, which means that the doctor simultaneously sees the level of leukocytes, platelets, and hemoglobin. When making a diagnosis, the doctor first chooses between three groups: infections, immune diseases and conditions, and malignant diseases. The doctor interviews and examines the patient, after which, based on symptoms, examination and diagnostic data, he determines further tactics.
If the reason for the increase in ESR has not been identified, the analysis should be repeated after 1-3 months. Normalization of the indicator is observed in almost 80% of cases.
ESR and oncology
In the absence of an inflammatory and infectious disease, a significant increase in ESR should raise suspicion regarding the presence of a malignant tumor. At the first suspicion of its presence, a consultation with an oncologist and a thorough additional examination using high-tech equipment and competent specialists are necessary.
Oncology is a multifactorial disease, accompanied by both inflammatory processes and anemia, metabolic disorders, and therefore causing the body to release a large amount of active substances and proteins. Therefore, most patients with various forms of malignant tumors have an elevated ESR.
For example, ESR in lung cancer may increase in the presence of pneumonia near the tumor. With colon or stomach cancer, severe anemia occurs, which leads to an increase in ESR.
There is no specific level for each tumor; most often, the increase is due to a combination of many factors.
The highest level of ESR (80-90 mm/h or more) associated with oncology is usually determined in diseases grouped as “paraproteinemias” (myeloma, Waldenström's macroglobulinemia). With these diseases, structurally abnormal and functionally defective proteins appear in the blood, which leads to changes in the blood.
When elevated ESR is not dangerous
ESR depends on the characteristics of the erythrocyte membrane and the concentration of certain proteins in the blood. Sometimes their number changes, but this is not associated with the disease, but is the norm. For example, the following people may have elevated values:
- In pregnant women Pregnancy and the erythrocyte sedimentation rate. The longer the period, the higher the ESR. In the first half, the indicator can increase to 18–48 mm/h, and in the later period - up to 30–70 mm/h. If a woman suffers from anemia, the results will be even higher - up to 95 mm/h.
- In the elderly Erythrocyte sedimentation rate and disease in the elderly. ESR increases with age. Even in healthy people after 60 years of age, the erythrocyte sedimentation rate can be 35–40 mm/h.
- For those who like fatty foods. Clinical assessment of laboratory test results. Because of this diet, there are more lipids in the blood, and the ESR also increases.
This does not mean that you do not need to pay attention to an increased ESR. In some cases, this is a sign of illness, so it is better to entrust the interpretation of the analysis to a therapist.