Indications and contraindications for the use of Rosuvastatin
There are two main indications for taking this drug:
- Hypercholesterolemia.
- Hypertriglyceridemia.
It should be noted that, together with treatment with Rosuvastatin, strict adherence to the diet prescribed by the doctor is mandatory. Otherwise, the effectiveness of the drug is sharply reduced.
The use of the drug is limited if patients have the following conditions:
- The presence of individual hypersensitivity to the main or additional ingredients of the drug.
- Acute and chronic liver diseases.
- Myopathy.
- Chronic kidney disease.
- Pregnancy and breastfeeding period.
- Sepsis.
- Severe injuries.
If there are serious indications, Rosuvastatin can be prescribed with extreme caution to patients with endocrine pathology, as well as to patients under the age of 18 and over 60 years of age.
Description of the drug ROSUVASTATIN
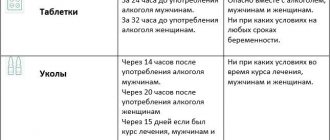
Use with caution in the presence of risk factors for the development of rhabdomyolysis (including renal failure, hypothyroidism, personal or family history of hereditary muscle diseases and a previous history of muscle toxicity when using other HMG-CoA reductase inhibitors or fibrates), in chronic alcoholism, in older patients 65 years old, with a history of liver disease, sepsis, arterial hypotension, during major surgery, trauma, severe metabolic endocrine or electrolyte disturbances, with uncontrolled epilepsy, in people of Asian origin (Chinese, Japanese).
Therapy should be discontinued if CPK levels are significantly increased (more than 5 times the ULN) or if muscle symptoms are severe and cause daily discomfort (even if the CPK level is 5 times less than the ULN).
When using rosuvastatin at a dose of 40 mg, it is recommended to monitor renal function indicators.
In most cases, proteinuria decreases or disappears during therapy and does not indicate the onset of acute or progression of existing kidney disease.
An increased incidence of myositis and myopathy has been reported in patients taking other HMG-CoA reductase inhibitors in combination with fibric acid derivatives (including gemfibrozil), cyclosporine, niacin, azole antifungals, protease inhibitors and macrolide antibiotics. Gemfibrozil increases the risk of myopathy when combined with certain HMG-CoA reductase inhibitors. Therefore, co-administration of rosuvastatin and gemfibrozil is not recommended. The balance of risk and possible benefit should be carefully weighed when using rosuvastatin and fibrates or niacin together.
It is recommended to determine liver function indicators before starting therapy and 3 months after starting therapy. The use of rosuvastatin should be discontinued or the dose reduced if the level of transaminase activity in the serum is 3 times higher than the ULN.
In patients with hypercholesterolemia due to hypothyroidism or nephrotic syndrome, treatment of underlying diseases should be carried out before starting treatment with rosuvastatin.
Impact on the ability to drive vehicles and operate machinery
When engaging in potentially hazardous activities, patients should be aware that dizziness may occur during therapy.
Adverse reactions and symptoms of overdose
Taking the drug may be accompanied by a large number of side effects. Most often, patients develop the following conditions:
- From the musculoskeletal system: arthritis, myositis, myopathies.
- CNS: headaches, dizziness, sleep disturbances, anxiety, depressive thoughts.
- From the respiratory system: cough, bronchial asthma, rhinitis, pharyngitis, tracheitis, bronchitis and pneumonia.
- Urinary tract infections.
- Gastrointestinal tract: dyspeptic syndrome, bloating, gastritis.
- From the cardiovascular system: tachycardia or angina.
- Allergic reactions.
An overdose of the drug is currently not described.
Ro-statin
From the urinary system
In patients receiving high doses of rosuvastatin (mainly 40 mg), tubular proteinuria was observed, which in most cases was transient. This proteinuria did not indicate acute kidney disease or progression of kidney disease. In patients taking the drug at a dose of 40 mg, it is recommended to monitor renal function parameters during treatment.
From the musculoskeletal system
The following effects on the musculoskeletal system have been reported with the use of rosuvastatin at all dosages and, in particular, when taking doses of the drug exceeding 20 mg: myalgia, myopathy, and in rare cases, rhabdomyolysis.
Determination of creatine phosphokinase activity
Determination of CPK activity should not be carried out after intense physical exercise or in the presence of other possible reasons for increased CPK activity, which
may lead to incorrect interpretation of the results obtained. If the initial CPK activity is significantly increased (5 times higher than the upper limit of normal), a repeat measurement should be taken after 5-7 days. Therapy should not be started if a repeat test confirms the initial CPK activity (more than 5 times the upper limit of normal).
Before starting therapy
When prescribing the drug Ro-statin, as well as when prescribing other HMG-CoA reductase inhibitors, caution should be exercised in patients with existing risk factors for myopathy/rhabdomyolysis; it is necessary to consider the balance of risk and possible benefit of therapy and conduct clinical observation.
During therapy
The patient should be informed to immediately report to the doctor the unexpected onset of muscle pain, muscle weakness or cramps, especially in combination with malaise and fever. In such patients, CPK activity should be determined. Therapy should be discontinued if CPK activity is significantly increased (more than 5 times the upper limit of normal) or if muscle symptoms are severe and cause daily discomfort (even if CPK activity is less than 5 times the upper limit norms). If symptoms disappear and CPK activity returns to normal, re-prescribing Rostatin or other HMG-CoA reductase inhibitors in lower doses should be considered with careful monitoring of the patient. Routine monitoring of CPK activity in the absence of symptoms is impractical. Very rare cases of immune-mediated necrotizing myopathy have been reported with clinical manifestations in the form of persistent weakness of the proximal muscles and increased CPK activity in the serum during treatment or upon discontinuation of statins, incl. rosuvastatin. Additional studies of the muscular system and nervous system, serological studies, and therapy with immunosuppressive drugs may be required.
There were no signs of increased effects on skeletal muscles when taking the drug Rostatin and concomitant therapy. However, an increase in the number of cases of myositis and myopathy has been reported in patients taking other HMG-CoA reductase inhibitors in combination with fibric acid derivatives, including gemfibrozil, cyclosporine, nicotinic acid in lipid-lowering doses (more than 1 g / day), azole antifungals, inhibitors HIV proteases and macrolide antibiotics. Gemfibrozil increases the risk of myopathy when used together with certain HMG-CoA reductase inhibitors. Thus, the simultaneous use of Rostatin and gemfibrozil is not recommended. The balance of risk and possible benefit should be carefully weighed when using the drug Rostatin together with fibrates or lipid-lowering doses of nicotinic acid (more than 1 g/day). Taking the drug Rostatin at a dose of 40 mg together with fibrates is contraindicated. 2-4 weeks after the start of treatment and/or when increasing the dose of the drug Ro-statin, monitoring of lipid metabolism parameters is necessary (if necessary, dose adjustment is required). Effect on liver function
It is recommended to determine liver function indicators before starting therapy and 3 months after starting therapy. Taking Rostatin should be stopped or the dose reduced if the activity of hepatic transaminases in the blood serum is 3 times higher than the upper limit of normal.
In patients with hypercholesterolemia due to hypothyroidism or nephrotic syndrome, treatment for underlying diseases should be carried out before starting treatment with Rostatin. Special populations. Ethnic groups
During pharmacokinetic studies among Chinese and Japanese patients, an increase in systemic concentrations of rosuvastatin was noted compared with values obtained among European patients.
HIV protease inhibitors
Concomitant use of the drug with HIV protease inhibitors is not recommended. Lactose
The drug should not be used in patients with lactase deficiency, galactose intolerance and glucose-galactose malabsorption.
Interstitial lung disease
Isolated cases of interstitial lung disease have been reported with some statins, especially over long periods of use. Manifestations of the disease may include shortness of breath, non-productive cough and deterioration in general health (weakness, weight loss and fever). If interstitial lung disease is suspected, statin therapy should be discontinued.
Diabetes mellitus type 2
In patients with glucose concentrations between 5.6 and 6.9 mmol/L, rosuvastatin therapy was associated with an increased risk of developing type 2 diabetes mellitus.
HMG-CoA reductase inhibitors, incl. Ro-statin may increase blood glucose concentrations.
Instructions for use of Rosuvastatin
The dosage is selected by the attending physician depending on the severity of the lipid profile disorder and the presence of cardiovascular risk.
The starting dose is 10 mg per day. If necessary, it is possible to increase the amount of the drug taken to 20 or 40 milligrams, but not earlier than after the start of treatment.
Increasing the daily dosage is possible only under the strict supervision of a specialist.
The drug should be taken whole, without chewing and with a sufficient amount of water. It is advisable to take the medication before meals.
Rosuvastatin Ro-statin caps 10 mg x30
Clinical and pharmacological group: Lipid-lowering drug Pharmaco-therapeutic group: Lipid-lowering drug - HMG-CoA reductase inhibitor
pharmachologic effect
A lipid-lowering drug from the statin group, an inhibitor of HMG-CoA reductase. According to the principle of competitive antagonism, the statin molecule binds to the part of the coenzyme A receptor where this enzyme is attached. Another part of the statin molecule inhibits the conversion of hydroxymethyl glutarate to mevalonate, an intermediate in the synthesis of the cholesterol molecule. Inhibition of the activity of HMG-CoA reductase leads to a series of sequential reactions, as a result of which the intracellular cholesterol content decreases and a compensatory increase in the activity of LDL receptors occurs and, accordingly, accelerates the catabolism of LDL cholesterol (Xc).
The lipid-lowering effect of statins is associated with a decrease in the level of total cholesterol due to LDL cholesterol. The decrease in LDL levels is dose-dependent and is not linear, but exponential.
Statins do not affect the activity of lipoprotein and hepatic lipases, do not have a significant effect on the synthesis and catabolism of free fatty acids, therefore their effect on TG levels is secondary and indirect through their main effects on reducing LDL-C levels. The moderate decrease in TG levels during statin treatment appears to be associated with the expression of remnant (apo E) receptors on the surface of hepatocytes involved in the catabolism of DILI, which contain approximately 30% TG.
In addition to the lipid-lowering effect, statins have a positive effect on endothelial dysfunction (a preclinical sign of early atherosclerosis), on the vascular wall, the condition of atheroma, improve the rheological properties of blood, and have antioxidant and antiproliferative properties.
The therapeutic effect appears within 1 week. after the start of therapy and after 2 weeks of treatment is 90% of the maximum possible effect, which is usually achieved by week 4 and remains constant thereafter.
Pharmacokinetics
After oral administration, Cmax of rosuvastatin in blood plasma is achieved in approximately 5 hours. Bioavailability is approximately 20%.
Rosuvastatin accumulates in the liver. Vd - approximately 134 liters. Plasma protein binding (mainly albumin) is approximately 90%.
It is biotransformed to a small extent (about 10%), being a non-core substrate for isoenzymes of the cytochrome P450 system. The main isoenzyme involved in the metabolism of rosuvastatin is CYP2C9. Isoenzymes CYP2C19, CYP3A4 and CYP2D6 are involved in metabolism to a lesser extent.
The main identified metabolites of rosuvastatin are N-dismethyl and lactone metabolites. N-dismethyl is approximately 50% less active than rosuvastatin; lactone metabolites are pharmacologically inactive.
About 90% of the rosuvastatin dose is excreted unchanged in the feces. The remainder is excreted in the urine. Plasma T1/2 - approximately 19 hours. T1/2 does not change with increasing dose. The average plasma clearance is approximately 50 l/h (coefficient of variation 21.7%).
As in the case of other HMG-CoA reducase inhibitors, the membrane transporter Xc is involved in the process of hepatic uptake of rosuvastatin, which plays an important role in the hepatic elimination of rosuvastatin.
Systemic exposure of rosuvastatin increases in proportion to the dose.
In patients with severe renal failure (creatinine clearance <.30 ml/min), the concentration of rosuvastatin in the blood plasma is 3 times higher, and the concentration of N-dismethyl is 9 times higher than in healthy volunteers. Plasma concentrations of rosuvastatin in hemodialysis patients were approximately 50% higher than in healthy volunteers.
In patients with liver failure, the degree of which was 8 and 9 on the Child-Pugh scale, an increase in T1/2 by at least 2 times was noted.
Indications of the active substances of the drug RO-Statin
Hypercholesterolemia (type IIa, including familial heterozygous hypercholesterolemia) or mixed hypercholesterolemia (type IIb) as an adjunct to diet when diet and other non-drug treatments (eg, exercise, weight loss) are insufficient.
Familial homozygous hypercholesterolemia as an adjunct to diet and other cholesterol-lowering therapy or in cases where such therapy is not suitable for the patient.
Open list of ICD-10 codes
Dosage regimen The method of administration and dosage regimen of a particular drug depend on its release form and other factors. The optimal dosage regimen is determined by the doctor. The compliance of the dosage form of a particular drug with the indications for use and dosage regimen should be strictly observed. Taken orally. The recommended starting dose is 10 mg 1 time/day. If necessary, the dose can be increased to 20 mg after 4 weeks. Increasing the dose to 40 mg is possible only in patients with severe hypercholesterolemia and a high risk of cardiovascular complications (especially in patients with familial hypercholesterolemia) with insufficient effectiveness at a dose of 20 mg and subject to physician supervision.
Side effect
From the side of the central nervous system: often - headache, dizziness, asthenic syndrome, possibly - anxiety, depression, insomnia, neuralgia, paresthesia.
From the digestive system: often - constipation, nausea, abdominal pain, possible - reversible transient dose-dependent increase in the activity of liver transaminases, dyspepsia (including diarrhea, flatulence, vomiting), gastritis, gastroenteritis.
From the respiratory system: often - pharyngitis, possibly - rhinitis, sinusitis, bronchial asthma, bronchitis, cough, dyspnea, pneumonia.
From the cardiovascular system: possible - angina, increased blood pressure, palpitations, vasodilation.
From the musculoskeletal system: often - myalgia, possible - arthralgia, arthritis, muscle hypertonicity, back pain, pathological pearl of the limb (without damage), rarely - myopathy, rhabdomyolysis (simultaneously with impaired renal function, while taking the drug at a dose 40 mg).
From the urinary system: tubular proteinuria (in less than 1% of cases - for doses of 10 and 20 mg, 3% of cases - for a dose of 40 mg), possibly - peripheral edema (arms, legs, ankles, legs), pain in the lower abdomen, infections urinary system.
Allergic reactions: possible - skin rash, itching, rarely - angioedema.
From the laboratory parameters: transient dose-dependent increase in CPK activity (if CPK activity increases by more than 5 times compared to ULN, therapy should be temporarily suspended).
Other: often - asthenic syndrome, possibly - accidental injury, anemia, chest pain, diabetes mellitus, ecchymosis, influenza-like syndrome, periodontal abscess.
Contraindications for use Liver disease in the active phase (including a persistent increase in the activity of hepatic transaminases or any increase in the activity of transaminases by more than 3 times compared with ULN), severe renal dysfunction (creatinine clearance <30 ml/min), myopathy, concomitant use of cyclosporine , pregnancy, lactation (breastfeeding), women of reproductive age who do not use adequate methods of contraception, children and adolescents under 18 years of age (since the effectiveness and safety have not been established), increased sensitivity to rosuvastatin.
Use during pregnancy and breastfeeding
Contraindicated during pregnancy and lactation.
Do not use in women of reproductive age who do not use reliable methods of contraception.
Use for liver dysfunction Contraindicated for liver diseases in the active phase (including a persistent increase in liver transaminase activity or any increase in transaminase activity more than 3 times compared to ULN).
Use for impaired renal function Contraindicated in cases of severe impaired renal function (CC<.30 ml/min).
Use in children Contraindicated in children and adolescents under 18 years of age (since efficacy and safety have not been established).
special instructions
Use with caution in the presence of risk factors for the development of rhabdomyolysis (including renal failure, hypothyroidism, personal or family history of hereditary muscle diseases and a previous history of muscle toxicity when using other HMG-CoA reductase inhibitors or fibrates), in chronic alcoholism, in older patients 65 years old, with a history of liver disease, sepsis, arterial hypotension, during major surgery, trauma, severe metabolic endocrine or electrolyte disturbances, with uncontrolled epilepsy, in people of Asian origin (Chinese, Japanese).
Therapy should be discontinued if CPK levels are significantly increased (more than 5 times the ULN) or if muscle symptoms are severe and cause daily discomfort (even if the CPK level is 5 times less than the ULN).
When using rosuvastatin at a dose of 40 mg, it is recommended to monitor renal function indicators.
In most cases, proteinuria decreases or disappears during therapy and does not indicate the onset of acute or progression of existing kidney disease.
An increased incidence of myositis and myopathy has been reported in patients taking other HMG-CoA reductase inhibitors in combination with fibric acid derivatives (including gemfibrozil), cyclosporine, niacin, azole antifungals, protease inhibitors and macrolide antibiotics. Gemfibrozil increases the risk of myopathy when combined with certain HMG-CoA reductase inhibitors. Therefore, co-administration of rosuvastatin and gemfibrozil is not recommended. The balance of risk and possible benefit should be carefully weighed when using rosuvastatin and fibrates or niacin together.
It is recommended to determine liver function indicators before starting therapy and 3 months after starting therapy. The use of rosuvastatin should be discontinued or the dose reduced if the level of transaminase activity in the serum is 3 times higher than the ULN.
In patients with hypercholesterolemia due to hypothyroidism or nephrotic syndrome, treatment of underlying diseases should be carried out before starting treatment with rosuvastatin.
Impact on the ability to drive vehicles and operate machinery
When engaging in potentially hazardous activities, patients should be aware that dizziness may occur during therapy.
Drug interactions
With the simultaneous use of rosuvastatin and cyclosporine, the AUC of rosuvastatin was on average 7 times higher than the value observed in healthy volunteers, while the plasma concentration of cyclosporine did not change.
Initiating rosuvastatin therapy or increasing the dose of the drug in patients receiving concomitant vitamin K antagonists (eg, warfarin) may lead to an increase in prothrombin time and INR, and discontinuation of rosuvastatin or dose reduction may lead to a decrease in the INR (INR monitoring is recommended in such cases).
The combined use of rosuvastatin and gemfibrozil leads to a 2-fold increase in Cmax in blood plasma and AUC of rosuvastatin.
The simultaneous use of rosuvastatin and antacids containing aluminum and magnesium hydroxide leads to a decrease in the plasma concentration of rosuvastatin by approximately 50%. This effect is less pronounced if antacids are used 2 hours after taking rosuvastatin (clinical significance unknown).
The simultaneous use of rosuvastatin and erythromycin leads to a decrease in rosuvastatin AUC by 20% and rosuvastatin Cmax by 30% (probably as a result of increased intestinal motility caused by erythromycin).
Concomitant use of rosuvastatin and oral contraceptives increases the AUC of ethinyl estradiol and AUC of norgestrel by 26% and 34%, respectively. Such an interaction cannot be excluded with the simultaneous use of rosuvastatin and hormone replacement therapy.
Gemfibrozil, other fibrates and lipid-lowering doses of nicotinic acid (≥1 g/day) increased the risk of myopathy when used concomitantly with other HMG-CoA reductase inhibitors, possibly due to the fact that they can cause myopathy when used as monotherapy.
Co-administration of rosuvastatin and itraconazole (CYP3A4 inhibitor) increases the AUC of rosuvastatin by 28% (clinically insignificant).
,
Analogues of the drug
The drug has a fairly large number of analogues. Their cost can be both higher and lower and varies from 100 to 1000 rubles.
The most well-known analogues of Rosuvastatin include: Pravastatin, Lipitor, Simvastol, Lovastatin, Rozulip, Simvastatin, Atoris, Roxera, Crestor and a number of other drugs.
It is not recommended to change one medicine to another without the consent of a specialist. If necessary, the doctor himself will adjust the treatment, change the dosage and prescribe another drug.