Causes of trophic ulcers on the leg
A trophic ulcer always accompanies another serious disease. Diseases that contribute to the appearance of trophic ulcers:
- advanced stage of varicose veins
- thrombophlebitis
- atherosclerosis
- diabetes
- hypertonic disease
- burns, frostbite
- arsenic or chromium poisoning
- radiation exposure
- diseases of the spinal cord and peripheral nerves
- complicated tuberculosis and syphilis
- blood diseases
- long-term immobility as a result of injury (bedsores)
- complicated skin diseases, including allergic ones
Pathogenesis of ulcers. What is happening and how to treat it?
Whatever causes a trophic ulcer, in order to get rid of it, or at least reduce its area, you need to treat both the cause and the ulcer itself. Traditionally, we use various ointments, powders, and drops for treatment. These dosage forms can fight microbes that multiply in dead cells, stimulate the formation of new blood vessels, and dry or moisturize the surface of the ulcer. But all of them are applied only externally, minimally affecting the skin and subcutaneous tissues. But in case of chronic inflammation, the edge of the chronic wound defect itself becomes partly the reason for the non-healing of the wound: the composition of a special intercellular substance, which normally provides support for cells, their nutrition and exchange, changes. The ratio of substances that form this framework-matrix is disrupted. The production of dense collagen increases, which is difficult for blood vessels to grow and which is difficult for new epithelial cells to come to. Therefore, the idea of delivering substances that take part in normal metabolism in connective tissue, but whose reserves are depleted due to reasons related to the underlying disease, and are in the patient’s body in insufficient quantities for restoration (regeneration), directly into the thickness of the suffering tissues is very attractive. There are a lot of such substances, but not all of them can be produced in the form of medicines. One of the drugs that are available to correct tissue metabolism in a wound is hyaluronic acid (HA), a natural component of the human body.
Why is hyaluronic acid needed? Treatment .
Our connective tissue consists of fibroblast cells and intercellular substance, one of the main components of which is hyaluronic acid. It has many functions: in addition to the formation of intercellular spaces, it ensures the supply of nutrients to cells and the removal of metabolic products; interacting with cellular receptors, it stimulates the movement and reproduction of cells (fibroblasts and epithelial cells). Hyaluronic acid also absorbs metabolic products, including reactive oxygen species, and blocks lipid peroxidation.
Thanks to everything described, HA activates natural regeneration processes, while acting in a balanced manner, without changing dividing cells and without increasing the formation of scar tissue, and these actions depend on the amount of hyaluronic acid formed, which means it works in both chronic and acute wounds, regardless of the presence or absence of signs of infection.
Trophic ulcer - symptoms
Trophic ulcers do not form spontaneously. Initially, swelling appears, accompanied by severe itching. The skin becomes thinner. Pigmentation or cyanosis appears.
Multiple trophic ulcers on the leg
The appearance of a trophic ulcer is often accompanied by chills and night cramps of the calf muscles. Due to stagnation in the lymphatic vessels, droplets of liquid begin to appear on the glassy surface of the skin. Next, the foci of exfoliated epidermis merge, and an ulcer with ragged, compacted edges is formed, causing severe pain at the slightest touch. As a rule, the ulcer surface is quickly colonized by bacteria, and the bleeding ulcer begins to fester.
Trophic ulcer with varicose veins
More than 70% of cases of trophic ulcers are caused by severe cases of varicose veins. Even minor damage to the integrity of the skin with varicose veins can lead to the formation of ulcers on the ankles and legs.
Large trophic ulcer on the leg
Trophic ulcers located on the lower leg indicate serious changes in larger venous vessels and the spread of an area with impaired innervation and poor blood supply. A trophic ulcer of the leg usually causes severe pain.
Principles (stages) of treatment
Actions when treating a wound depend not only on the conditions and causes of its appearance, but also on the stage at which the wound process has stopped in it.
The first stage of the wound process is acute. During it, vascular changes occur caused by a reaction to damage, and the process of blood clotting is actively underway. If the wound is infected, pus is formed and toxic substances are simultaneously absorbed into the tissue.
At this stage, it is necessary, first of all, to clean the wound - remove dead tissue from it, remove foreign bodies (with the help of a doctor), drain it - remove pus and exudate from the wound. It is also necessary to prevent infection from entering the wound. It is best to wash the affected area with saline solution, as caustic disinfectant liquids can harm surrounding healthy tissue.
The second stage of the wound process is granulation. At this stage, a thin layer of connective tissue begins to form on top of the wound. The edges of the wound begin to tighten, and it closes itself. The thinnest capillaries are formed in the connective tissue layer, providing nutrition to regenerating tissues. Often chronic wounds stop at this phase, and the healing process does not proceed further; This is most often what happens with trophic ulcers.
At the granulation stage, it is important, firstly, to protect the newly formed tissue from mechanical damage, secondly, to stimulate further regeneration, and thirdly, to prevent the development of the inflammatory process - despite the fact that the wound is closed, the risk of infection and inflammation remains. To stimulate tissue regeneration, methyluracil ointment is used (you can use a ready-made Voskopran dressing with methyluracil ointment); to protect the surface of the wound, atraumatic dressings should be used that do not stick to the wound surface and do not injure it.
We should not forget about maintaining a maintenance diet and sleep schedule - this will help speed up the healing process.
Trophic ulcer, stages or course options
The size of the trophic ulcer directly depends on the lack of blood supply and the duration of the pathological process. Usually the ulcerative surface occupies no more than 35 cm2. If left untreated, it can cover the entire lower leg and reach 100 cm2. Treatment methods for trophic ulcers must be correct, competent and qualified: no poultices or tinctures!
Stages of appearance of a trophic ulcer
The initial stage (small bleeding ulcer) is complicated by the addition of a bacterial and fungal infection. Purulent contents with an unpleasant odor begin to separate from the ulcer. The longer the process, the deeper the layers are subject to inflammation and rotting. The ulcerative lesion spreads to the calf muscles, involving the ankle joint in the inflammatory process. In advanced cases, the development of pyoderma, phlegmon and sepsis is possible.
It is worth distinguishing between venous and arterial trophic ulcers. The former occur in patients of any age, while arterial ulcers are a disease that occurs exclusively in old age, caused by atherosclerosis of the artery walls.
What bad could happen?
The administration of the drug is generally not painful, but in case of increased sensitivity it can be unpleasant. However, this can be resolved by using additional analgesia [[2]].
The drug has not been tested in pregnant and lactating women and children under 18 years of age, therefore the administration of hyaluronic acid cannot be recommended for these groups of patients.
When mixing hyaluronic acid with anesthetic solutions, before preparing and administering the mixture, it is necessary to specifically ask the patient about drug allergies in general and allergies to the anesthetic planned for administration in particular.
Trophic ulcer, diagnosis
When diagnosing a trophic ulcer and identifying the causes of its occurrence, the following laboratory tests are used:
- determination of blood sugar levels
- Wasserman reaction
- cytological analysis
- bacteriological examination
The doctor also prescribes a number of necessary studies:
- Ultrasound examination of the vessels of the lower extremities
- angiography (x-ray examination of blood vessels with a contrast agent)
- rheovasography
- infrared thermography
- spiral computed tomography
Diagnosis of a trophic ulcer is a key stage in proper treatment
To select an effective treatment, consultation with a phlebologist surgeon specializing in vascular diseases of the lower extremities is necessary.
Why is a trophic ulcer dangerous? - Wikipedia warns!
The main point in the treatment of trophic ulcers is to identify the underlying disease that caused the ulcerative skin defect. This approach will ensure effective treatment of ulcers and prevention of relapses. The danger of trophic ulcers lies in the fact that, in the absence of proper treatment, damaged cells are capable of malignant degeneration and the appearance of squamous cell carcinoma, and in rare cases, skin sarcoma. Therefore, even if the trophic ulcer has gone away, treatment after surgery should continue.
Surgery
For life-threatening complications of varicose veins, the presence of a large area of skin ulceration, or a deep wound, surgical treatment is used. The ulcer is cleaned mechanically using curettes (wound curettage), vacuuming or VAK therapy. In severe cases, the affected area is excised and the defect is covered with a skin graft from the patient's thigh. Sometimes additional blood vessels are inserted to not only remove the defect, but also restore blood supply. After the operation, the patient undergoes a course of rehabilitation, after which he returns to his normal life.
Trophic ulcer - treatment in Moscow
Do you have a trophic ulcer? Treatment in Moscow or in any other city is quite lengthy and involves a whole range of measures to ensure that the trophic ulcer disappears. Conservative treatment, the same as drug treatment, is aimed at reducing the symptoms of the underlying disease that caused a violation of tissue trophism, treating the ulcerative lesion itself and fighting secondary infection.
Excellent results in laser treatment of trophic ulcers
Depending on the stage, the trophic ulcer is removed in different ways. Treatment (Moscow offers many methods) depends on the stage of development of the trophic ulcer and is carried out in the following areas:
- local treatment;
- elastic compression;
- drug treatment;
- hemosorption - removal of toxic tissue breakdown products from the blood;
- physiotherapy;
- autoirradiation of blood with laser or ultraviolet rays;
- surgical intervention if indicated;
- visiting sanatoriums.
What to do if you have deep trophic ulcers of the lower extremities? What to do if a large trophic ulcer, treatment (photo, results you have already assessed) which you have not carried out, increases?
Dressings for the treatment of non-healing wounds
When treating wounds of any nature, including chronic ones, the correct selection of dressing material plays an important role.
Dressing material for non-healing wounds should be:
•hygroscopic;
•"breathable";
•elastic and flexible – the bandage will have to be worn for a long time, so it should not interfere with movements.
Biotekfarm company offers a wide selection of dressings for the management of wounds of any complexity and at any stage. So, for wounds in which there are fragments of necrotic tissue or hemorrhage, a Parapran dressing with chymotrypsin is suitable - the drug included in the dressing helps to break down necrotic tissue, helping to cleanse the wound.
To moisturize “dry” chronic wounds (bedsores, trophic ulcers) and accelerate their healing, it is recommended to use the “GelePran” dressing with miramistin or colloidal silver. This soft transparent dressing, consisting of 70% water, moisturizes the surface of the wound, and the medicine it contains (miramistin or silver) disinfects and promotes regeneration.
For the treatment of infected wounds, bactericidal dressings Voskopran with Povidone-iodine ointment, antimicrobial dressings Voskopran with Dioxidin ointment, and anti-inflammatory dressings Voskopran with Levomekol ointment are suitable. Polipran dressings with Dioxidin are excellent for preventing infection of wounds at the granulation stage.
The Chitopran dressing based on chitosan nanofibers will help stimulate regeneration. It provides optimal conditions for healing - sufficient humidity, breathability and protection from damage, and promotes the rapid growth of its own cells. It is worth paying attention to the fact that this bandage does not need to be removed - it resorbs on its own as the wound heals.
Trophic ulcer - treatment at home
The attending physician decides about the possibility of treating the disease at home. With the prescribed set of medications, the patient can do dressings at home, while regularly visiting the doctor. It is desirable, of course, that this doctor be a good specialist in the treatment of trophic ulcers. There are few such doctors in Moscow.
Leading specialist of our center for the treatment of trophic ulcers Malakhov A.M.
Our leading surgeon-phlebologist Alexey Mikhailovich Malakhov deals with this problem.
Trophic ulcer - treatment without surgery
If the cause of the ulcer is not venous pathology, then conservative measures are sufficient. A portable laser device is a great help in home treatment of the initial stages of ulcerative skin lesions up to 50 cm2 in size. A laser injected into a vein helps reduce blood viscosity, significantly reduces the risk of blood clots, and increases blood flow in problem areas. In addition, the laser beam effectively reduces pain and trophic ulcers. Laser treatment (reviews below) in combination with conservative treatment allows you to avoid surgical intervention.
Laser therapy is carried out in courses of 10-15 procedures. With the correct individual selection of treatment parameters, this treatment method does not cause complications, patients note good tolerability of the procedures, and the trophic ulcer is quickly eliminated. Laser treatment, the price of which is not too high, is very popular.
Trophic ulcer - laser treatment (EVLO, EVLK)
A more radical method of treating trophic ulcers is surgery using laser coagulation (Endovasal laser coagulation). We have been using the EVLT technique for many years. This treatment method consists of “burning out” the vein, which is located in the area of the trophic ulcer. The results are very good: the ulcers heal almost before our eyes. Scarring occurs over several weeks. At the same time, patients do not fall out of their normal routine of life.
Treatment of trophic ulcers with laser in
Laser treatment of trophic ulcers in Moscow has a number of advantages:
- low morbidity - the phlebologist does not make additional incisions in the ulcerated area;
- the ability to avoid long-term conservative treatment before surgery;
- high efficiency - scarring of the ulcer goes away quite quickly;
- positive cosmetic effect - low tissue trauma eliminates the formation of rough scars when the trophic ulcer disappears. Laser treatment, the cost of which can be discussed upon admission, will help you.
Examples of patients with diabetic ulcers treated in our clinic
Patient Lukyanov V.N., 75 years old.
Diagnosis: Diabetes mellitus type II. Diabetic foot syndrome, mixed form. Upon admission: Phlegmon of the right foot, in bone tissue cultures - abundant growth of Pseudomonas aeruginosa, St. aureus, Enterococcus faecalis. This patient literally ran to us from the purulent surgery department of one of the clinics in our city, where his foot was going to be amputated. His troubles began with inflammation and then phlegmon of the fourth toe of his right foot. He was hospitalized at this purulent surgery department, where he underwent amputation of the fourth finger. Then, during a month of hospitalization, due to the progression of purulent inflammation, his third and second fingers were amputated. Despite this, the infectious process spread to the foot and the patient developed phlegmon of the foot. They began to prepare him for amputation.
Upon admission to our clinic, the patient had severe pain, severe hyperemia and tenderness of the sole, exposed bones were visible in the wound, and there was a purulent discharge with a disgusting odor. We immediately performed bone culture. It contains abundant growth of Pseudomonas aeruginosa (Pseudomonas aeruginosa), St. aureus (Staphylococcus aureus), Enterococcus faecalis (fecal enterococcus).
For treatment in this case, we used a portable vacuum-flushing system that we developed. In it, the beneficial effect of negative pressure on wounds is enhanced by the effect of antiseptics used for washing. In addition, in the case of ischemic ulcers, overdrying of the wound surface is avoided. These systems have proven themselves well for the treatment of severe purulent wounds. In this case, the patient, as you can see in the picture, is mobile - treatment is carried out on an outpatient basis:
After the first dressings, the pain in the wound and the unpleasant odor almost completely disappeared, the pain decreased and the hyperemia on the sole was limited. Soon the ulcer significantly decreased in size, was filled with granulation tissue, and the culture results were negative. The patient underwent branded autodermoplasty:
All treatment took place on an outpatient basis. In the pictures below you can see the right foot of this patient at the time of admission to our Center and at discharge:
The following photographs show the foot of a 66-year-old patient before and after treatment in our clinic. She has an ischemic form of diabetic foot syndrome. The exposed bones of the left foot are visible.
Patient M., 66 years old. Diagnosis: Diabetes mellitus type II. Diabetic foot, ischemic form. Obliterating atherosclerosis. Occlusion of the arteries of the left leg
It all started with an ulcer of the first finger, after which, despite inpatient treatment in one of the leading clinics in St. Petersburg, several amputations followed, as a result of which necrosis spread to the foot. And at the time of admission to our clinic, the ulcer looked as shown in the first picture.
We were able to restore the skin through systemic antibacterial therapy and local treatment. Perforations were made in the bones, and the growth of granulations from these holes was stimulated through cell therapy. Then autodermoplasty was performed. Again, due to cell therapy, it was possible to achieve engraftment of the transplanted skin flap.
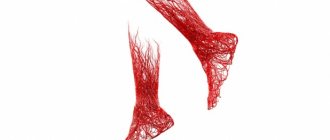
Obliterating endarteritis, also known as Buerger's disease, also known as Winivarter-Buerger disease, is characterized by inflammation that primarily affects the peripheral arteries in young smokers. The photo shows the leg of a patient with obliterating endarteritis, treated in our clinic.
With this disease, there is a very strong dependence on smoking: this disease does not occur in non-smokers, and if you quit smoking, the prognosis is favorable. Initially, the arteries of the distal parts of the feet become inflamed and close, then the disease spreads proximally. When the popliteal arteries are involved, intermittent claudication will occur. Therefore, the Fontaine-Pokrovsky classification does not apply here: ulceration and gangrene may precede intermittent claudication. Diagnostic criteria for the disease are presented below.
Trophic ulcer - radiofrequency treatment (RFA, RFO)
The radiofrequency treatment method is considered the most modern and safe if you have a trophic ulcer. RFA treatment in Moscow involves heating the walls of the vein with microwaves, it “closes”, and the trophic ulcer gradually shrinks. RFO treatment - and after a few months the problem vein is a connective tissue cord, and the entire load is transferred to neighboring, healthy vessels. This is how the trophic ulcer gradually heals.
Treatment of trophic ulcers with radiofrequency (RFA, RFO) in our center
RFO treatment in Moscow is carried out quite quickly; the patient goes home 10 minutes after the intervention. The radio frequency method provides the following advantages:
- short duration of the procedure - 30-40 minutes;
- exposure parameters are selected automatically and without the participation of a doctor;
- cosmetic effect - the absence of additional trauma promotes the formation of a less rough scar where there was a trophic ulcer. RFA treatment is very positive in this regard.
- the procedure is completely painless and easily tolerated;
- Hospitalization is not required, the patient can lead a normal life, limiting activity only after the procedure.
Is a diet necessary when treating a trophic ulcer?
What should be avoided if there is a trophic ulcer? Photos of complications will help you control yourself when dieting. Diet for trophic ulcers excludes salty foods and spices. It is necessary to saturate the body with nutrients, vitamins and Omega-3 acids. Vegetables (carrots, tomatoes, cabbage), fruits, nuts, milk, cheeses, vegetable and butter, and fish are especially useful. You should eat small portions to avoid a sharp increase in blood sugar. A radical change in diet is not required; a small adjustment will have a beneficial effect on the healing process.
Trophic ulcer - prevention
To prevent the trophic ulcer from returning and the treatment not to be in vain (the cost of which can only be found out after consultation), take care of prevention. Measures to prevent the occurrence of trophic ulcers and relapses:
- early detection and treatment of diseases that provoke the appearance of trophic ulcers;
- moderate physical activity (daily walking 2-3 km);
- use of compression hosiery;
- ignoring baths and saunas, hardening procedures for the legs;
- refusal of flour and sweets, predominance of fruits and vegetables in the diet;
- medical examination 2 times a year.
Frequently asked questions from our patients on the Internet about trophic ulcers
How to treat non-healing wounds on the legs?
To effectively treat non-healing leg wounds, it is necessary to understand how such wounds appeared. Long-term non-healing wounds on the legs can form as a result of a number of completely different pathologies, and each requires its own specific treatment.
How to treat non-healing wounds at home?
Before you begin to treat long-term non-healing wounds at home, you need to find out the cause of such wounds. Most often this is:
- Diabetes.
- Obliterating atherosclerosis.
- Chronic venous insufficiency.
If you want to cure long-term non-healing wounds, then in addition to the local use of ointments, it is necessary to deal with the underlying pathology that caused the problem.
How to treat a deep wound?
How to treat a deep wound should be asked to the doctor during an in-person consultation. Treating such wounds on your own, using the Internet, can be fraught with progression of the process and the development of a life-threatening condition.
My father developed sores on his legs six months ago, how can I get rid of them?
If “sores” on your legs appear and do not go away for a long time, as a rule, only a doctor will help you get rid of them. Long-term non-healing wounds are often a sign of a serious pathology that requires specific treatment.
Symptoms of non-healing wounds
•constant pain;
•converging edges of the wound;
•constant bleeding;
• “stuck” wound at one of the stages of healing for more than three weeks;
•often – unpleasant odor;
•conventional treatments do not help or help little.
These signs indicate that the regeneration processes in tissues are disrupted for one reason or another. For the treatment of chronic wounds, local treatment is not enough; comprehensive measures are required.
To achieve progress in healing, it is necessary to provide conditions for restoring the normal rate of regeneration. They largely depend on the cause of the chronic wound, but there are recommendations that are common to all situations.
The body needs to provide:
•balanced nutrition - in particular, the diet should be enriched with vitamins A and B, which stimulate tissue regeneration, and vitamin C, which promotes the production of collagen - a substance involved in the formation of connective tissue that closes the wound in the first stages;
•normal sleep mode – during sleep the regeneration process occurs more actively;
•protecting the wound and the area around it from external influences, such as rubbing, squeezing, etc.;
•wound ventilation – without air circulation, the wound will quickly fester.
More specific recommendations depend on the origin and nature of the wound.
Trophic ulcer - treatment. Reviews from our patients.
Patient's review of laser treatment for trophic ulcers in our center.
Victor Petrovich, 65 years old.
I am a pensioner with a whole cartload of all sorts of ailments. My legs had been hurting and swollen for a long time, but I, like many, put off going to the doctor until later. I took some pills on the advice of a neighbor nurse, although I didn’t notice any particular improvement. In general, I lived to the point where I had a huge ulcer on my leg. God bless your doctors, I already thought that I would be left without a leg. They gave me laser treatment. I didn’t particularly delve into the nuances of this case; the doctors guaranteed a good result. Everything went without pain, literally after a few days my trophic ulcer began to disappear before my eyes, and after two weeks only a small scar remained. Of course, various medications were prescribed, then I went to a sanatorium and forgot about this terrible disease. Thanks to all the doctors of the Medical Center for Phlebology, especially Dr. Malakhov Alexey Mikhailovich.
A patient's review of the treatment of trophic ulcers using the EVLO method in our center.
Komissarova L.I.
Our patient with surgeon-phlebologist A.M. Malakhov. after treatment
My leg ached constantly, there was a buzzing sensation in it at the end of the day, and then a trophic ulcer formed, which became larger and larger. I didn’t dare to have surgery using the classical method, because I was afraid after reading reviews online and all sorts of complications. Well, my daughter is in the know, she found me an experienced doctor in Moscow, Alexey Mikhailovich Malakhov. Before the operation, and this is endovasal laser coagulation, at the medical center in Moscow, where I decided to have it, they did an ultrasound, donated blood and that’s it. After the operation, I was forced to get up from the table and walk for about an hour. After 3 weeks I saw my doctor. I didn’t worry about scars, the main thing was that the ulcer healed faster. It's been 3 months since the laser procedure on my leg. Everything is fine, the ulcer has become very small, but I hope it will heal completely soon.
I'm very glad that everything went well. Thanks for all. Komissarova Lyudmila Ivanovna, December 7, 2021
Examples of patients with venous ulcers treated in our Center
Patient N., 24 years old Diagnosis: Varicose veins of the left lower limb. After complete healing of the trophic ulcer (this took 1 month), the patient underwent outpatient surgery - he underwent removal of the varicose great saphenous vein. In the second photograph, taken three weeks after the operation, traces of punctures are still visible, through which this vein destroyed by varicose disease was removed. The patient is observed for 9 years after the operation - there is no recurrence of the ulcer.
Patient Alexandrova L.B., 66 years old, before and after outpatient treatment in our Center. Diagnosis: Postthrombotic disease of the left lower limb. Circular trophic ulcer of the left leg. The photo shows a galosh that filled with lymph every half hour of walking. The clinic website has
.
The story of this patient was described by a journalist who interviewed her for an article about Andreev D.Yu. "Healing Man":
“The professional life of an obstetrician-gynecologist is a struggle for the health of patients. This is what Lyudmila Borisovna Alexandrova did. At the age of sixty, she herself became a patient. Now I can’t even remember all the offices of vascular surgeons, phlebologists, lymphologists, where they tried to fight her trophic ulcer. Everywhere - to no avail. She walked with a huge man's galosh on her foot. The ulcer that consumed her body released lymph that flowed down her leg. Every half hour it was necessary to pour one and a half glasses of this liquid out of the galoshes. I was constantly in pain... After six years of such a life, Alexandrova, in a fit of despair, wrote a letter to the Minister of Health (T. Golikova).
The administrative-bureaucratic machine began to move and got the head doctor of the local clinic when the writer was at the dacha. There she was found by an ambulance sent by the chief. They were admitted to the hospital (“St. George”). A council was quickly assembled, headed by a professor, one of the city’s leading lymphologists. Conclusion of venerable specialists: amputation, urgently.
“As a surgeon,” Lyudmila Borisovna recalls now, “I myself understood that with a circular ulcer there are only two outcomes: amputation or death. But how hard it is to give up hope!…
The night passed without sleep. In the morning, no longer remembering why, she went downstairs. There's a newsstand in the lobby. On the counter lay the magazine “Prevention, Health, Beauty.” I took it...
I started calling. I contacted vascular surgeon Andreev. Friendly voice, clear, specific questions. And then confident: “I will cure you”...
On the same day, Lyudmila Borisovna left St. George. The next day I met with Andreev. It was the end of November. In May, she parted ways with her six-year curse, an aggressive circular ulcer.
“I have no words to express my gratitude,” says the healed woman. “I think as many people as possible should know about this doctor.”
She herself spoke about it in a letter to Elena Malysheva, Doctor of Medical Sciences, professor, one of the creators of the “Calling” project, who hosts the “Health” program on Channel 1 TV. But either the letter did not arrive, or the respected professor and TV presenter, like some of Andreev’s colleagues in St. Petersburg, also sometimes use the formula: “This cannot happen, because it never happens” ... "
We examine all patients with venous ulcers for concomitant arterial pathology. And if it is present, we determine the ankle-brachial index. This is important for prescribing adequate compression therapy. Here is an example of such a patient:
Patient Sh., 65 years old. Diagnosis: Postthrombotic disease of the left lower limb. Obliterating atherosclerosis. Occlusion of the superficial femoral, popliteal and anterior tibial arteries. Ischemia stage III ABI 0.5.
Thus, this patient has a combined lesion of the veins and arteries of the left lower limb. Stage 3 ischemia means that due to a sharp decrease in arterial blood flow, the patient cannot remain in a horizontal position for a long time - severe pain occurs; at night he is forced to sleep with his leg off the bed or sitting. In one of the clinics in St. Petersburg there was an attempt - unsuccessful - to restore arterial blood flow. By using the technologies we developed, we - without vascular surgery - managed to improve blood supply and significantly cleanse the ulcer. Then we performed skin grafting:
Complete healing of ulcers – after 8 months of treatment:
All treatment, including skin graft surgery, was carried out on an outpatient basis; hospitalization in our clinic was not required.
Usually located in the distal parts of the limb; surrounded by pale or cyanotic skin. Typical localization is the toes, forefoot and heel area (especially in bedridden patients). They are less common on the dorsum of the foot, on the anterior surface of the lower leg and in the area of the lateral and medial ankles. In the last two cases, they can mimic venous ulcers. Provoking factors are minor skin injuries (for example, when wearing tight shoes). The bottom of the ulcer is usually necrotic tissue; There are few granulations, they are pale. As a rule, there is no swelling of the lower limb. Unlike venous ulcers, which almost never penetrate deeper than the proper fascia of the leg, with these ulcers there are frequent cases of exposure of tendons and bones. Other distinctive features are a small amount of wound discharge and the lack of severity of the inflammatory reaction in the tissues surrounding the ulcer, even at the first stage of the wound process. Another difference from ulcers of venous etiology is that raising the affected limb above the level of the heart increases the pain, and does not alleviate it, as with venous ulcers.
The main contingent of patients are elderly men. Since in obliterating atherosclerosis ulcers are a manifestation of stage IV of arterial ischemia (according to the Leriche-Fontaine-Pokrovsky classification), their occurrence is preceded (and accompanied) by the appearance of a symptom of intermittent claudication (stage II) and pain in the distal parts of the limb at rest (primarily - in a horizontal position) – stage III of ischemia.
When examining the patient, the absence of pulsation of the popliteal artery and arteries of the foot is revealed - the main criterion for distinguishing these ulcers from ulcers of venous etiology.
Ultrasound duplex scanning of the arteries of the lower extremities allows confirmation and clarification of clinical findings.
The photographs below demonstrate modern treatment options for these ulcers.
Patient R., 70 years old.
Diagnosis: Obliterating atherosclerosis. Occlusion of the right superficial femoral, popliteal and anterior tibial arteries. Trophic ulcer of the right leg. Purulent arthritis and fistula of the right ankle joint. Ischemia stage IV Concomitant diagnosis: type II diabetes. ABI 0.2. Systolic pressure at a. tibialis post. 30 mmHg This patient came to our clinic with very severe pain. There is a terrible ulcer on my only right leg. You can see the exposed ankle joint. Note that the ulcer is in a typical location for venous ulcers, although the patient's veins are normal.
To cure this patient, it was necessary to perform an autovenous femoral-tibial bypass with an autovenous vein, after which it became possible to heal the ulcer through local treatment:
The patient has been observed for 11 years - there is no recurrence of the ulcer.
Trophic ulcers in diabetes mellitus are manifestations of diabetic foot syndrome and/or diabetic necrobiosis lipoidica.
According to the international classification (Netherlands 1991), neuropathic, ischemic and mixed (neuroischemic) forms of this syndrome are distinguished. Differential diagnosis of neuropathic and ischemic forms of diabetic foot syndrome is given in the table.
Diabetic ischemic foot syndrome (and ulcers associated with this syndrome) are caused by atherosclerotic damage to the arteries of the lower extremities of diabetic patients. It is well known that diabetes mellitus is one of the leading risk factors for obliterating atherosclerosis. Thus, despite the differences in atherosclerotic damage to the arteries of the lower extremities in patients with and without diabetes mellitus (see table below), ulcers in ischemic diabetic foot syndrome are more correctly classified as atherosclerotic trophic ulcers, considering diabetes mellitus as a concomitant disease.