How does the tricuspid valve work?
The human heart consists of four sections.
The aortic and pulmonary valves communicate with the atrial cavity and the arteries of the same name. The left and right atrioventricular openings are located between the ventricle and the atrium of the heart on the corresponding side. The tricuspid valve (right AV orifice) is a window with three flexible plates - leaflets on a ring of fibrous tissue, communicating with the right parts of the heart. Normally it has three valves: anterior, posterior and septal, due to which it is also called tricuspid. There may be four or six leaves.
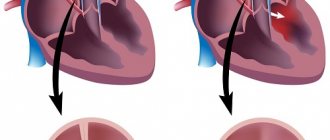
The AV orifice contains papillary muscles and chordae tendineae extending from them, which are attached to the base of each leaflet and ensure proper operation of the valve, tension or relaxation during heart contraction cycles. The right atrioventricular valve is shown in the figure below:
Mechanism of operation
During diastole (relaxation of the heart muscle), the tricuspid valve opens and allows venous blood to flow from the right atrium to the right ventricle. During systole (contraction of the heart), the valves close tightly and do not wrap due to fixation by the chordae and muscles. From the ventricle the blood is ejected into the pulmonary trunk. Next, along the right and left main arteries it is sent to the lungs for gas exchange. In this case, the muscles and functional apparatus of the valve prevent the backflow of blood into the heart cavity from large vessels.
This happens due to:
- Holding the valve leaflets open by the papillary muscles and chordae during the filling phase.
- Tight closure to prevent regurgitation (backflow into the atrium) during the phase of expulsion of blood into the pulmonary trunk.
- The difference between the larger size of the valve leaflets and the smaller diameter of the AV orifice, due to which the valve closes tightly during the contraction phase as the volume of the ventricle changes.
- Anatomically, the valve is shaped like a funnel, which ensures passive blood flow when pressure changes in the cavities of the heart.
Causes of tricuspid insufficiency
The development of congenital tricuspid valve insufficiency can occur for a number of reasons, including:
- infectious diseases in a pregnant woman,
- exposure to ionizing radiation,
- Ebstein's anomaly
- connective tissue dysplasia.
Acquired tricuspid insufficiency can develop due to deformation or wrinkling of the valves, their calcification, as well as due to rupture of the papillary muscles, chordae tendineae, and dysfunction of the annulus fibrosus. This can happen against the background of:
- rheumatism (the most common cause of tricuspid valve insufficiency),
- infective endocarditis,
- carcinoid syndrome,
- other pathologies.
Main functions
Throughout a person’s life, the heart provides a closed path of blood flow, delivery of oxygenated blood to organs and tissues, and venous outflow of carbon dioxide and breakdown products. The cardiovascular system consists of blood circulation circles. The large one originates in the left ventricle and ends in the right atrium, the small one starts in the right ventricle and goes to the left atrium.
The tricuspid valve is actually an element of a small circle that performs the following functions:
- During heart contractions, it prevents reverse regurgitation (blood flow from the lower ventricle into the atrium).
- Directly involved in blood circulation, ensures the delivery of venous blood to the vessels of the lungs.
- Through which the process of gas exchange in the alveoli of the lung tissue and heat transfer takes place.
Pathological changes in damage to the aortic valves
The result of congenital and acquired changes is the formation of insufficient closure of the valves, this is expressed in the return of part of the blood to the cavity of the left ventricle when it relaxes. The cavity expands and lengthens in size.
Forced intensification of contractions causes, over time, a breakdown of compensatory mechanisms and hypertrophy of the muscular layer of the left ventricle. This is followed by dilation of the left venous opening connecting the ventricle to the atrium. Overload from the left sections is transmitted through the pulmonary vessels to the right heart.
The impaired ability of the valve leaflets to close tightly leads to the formation of insufficiency and prolapse under the influence of reverse blood flow. Usually, aortic stenosis occurs simultaneously. In the clinical picture we can talk about the predominance of one type of defect. Both increase the load on the left ventricle of the heart. Features of the course must be taken into account when choosing a treatment method.
What pathologies of the right atrioventricular valve most often occur?
Dysfunction of the right atrioventricular orifice most often takes the form of stenosis or insufficiency. Pathological changes in the valvular apparatus of the heart significantly impair blood circulation, which is manifested by certain clinical symptoms.
Tricuspid valve stenosis
- It is associated with certain diseases of an infectious nature, infection with streptococcal, enterococcal or treponemal infections.
- It is more often detected in patients with rheumatism or syphilis.
- Represents a narrowing and reduction in the diameter of the AV opening (stenosis), which significantly impedes the flow of blood through the valve.
- In 60% it is combined with damage to other valves, mitral or aortic.
- Circulating in the bloodstream, the infection settles in all parts of the heart, affecting the elements of the valve apparatus.
- Due to the progressive inflammatory process, the tricuspid valve becomes sclerotic. The valves, annulus fibrosus, muscular elements and chords fuse, reducing the lumen of the AV foramen.
- Normally, the size of the valve is 3-4 centimeters; with stenosis, the diameter decreases from 3-1.5 cm.
- As a result of changes in hemodynamics, not the entire volume of blood flows from the atrium to the ventricle, and therefore stagnation develops in the pulmonary circulation.
- The examination is characterized by pathological reflux - swelling of the neck veins when pressing on the abdominal area where the liver is located.
- Auscultation of the heart reveals diffuse pulsation and enlargement of the cardiac boundaries, loud pathological murmur in the diastole phase.
- It manifests itself as portal hypertension (increased pressure in large hepatic vessels) with subsequent stagnation of blood in the spleen, intestinal vessels, and stomach.
- Characteristic symptoms are severe weakness, shortness of breath, swelling, cyanosis of the hands and face, irregular heartbeat, increased blood pressure, hemoptysis, swelling of the abdomen and fatty tissue, swelling of the veins around the navel.
- Without treatment, it leads to fatal heart failure and death.
- Drug treatment is ineffective; surgical intervention is indicated to replace the affected valve and save the patient’s life.
Right atrioventricular valve insufficiency
Most often occurs due to rheumatic infection, inflammation of the endocardium of the heart or rupture of elements of the valve apparatus, part of the chords or muscle fibers.- Extremely rare - this is a congenital defect.
- In addition to infection, dysfunction can be caused by changes in the right ventricle, its hypertrophy or dilatation, which leads to a compensatory increase in the diameter of the fibrous ring of the valve and disrupts its closure.
- May occur as a result of dilatation of the heart ventricle due to inflammatory diseases, myocarditis or cardiomyopathy.
- It is associated with opium addiction and its main complication – endocarditis (inflammation of the inner layer of the cardiac membrane).
- It is characterized by incomplete slamming or prolapse (protrusion) of the valve leaflets, due to which blood is constantly thrown back into the right atrium.
- During an ultrasound examination, the doctor sees changes in hemodynamics, the degree of blood reflux and the size of the narrowing of the AV opening.
- Auscultation (listening to the valves during heartbeat) reveals a pathological popping noise.
- Since the atrium does not have great compensatory capabilities, signs of dilatation (expansion) immediately appear.
- As with stenosis, it manifests itself as congestion in the liver, an increase in venous pressure and venous pulse (swelling of the neck veins when the heart contracts).
Congenital changes in the aortic valve
The exact causes of congenital disorders are still unknown. More often it occurs simultaneously with another congenital heart disease - the mitral valve.
The most common developmental defects:
- formation of two leaflets rather than three (bicuspid aortic valve);
- one of the sashes is larger than the others, stretches and sags;
- one valve is smaller than the others, underdeveloped;
- holes inside the doors.
Aortic valve insufficiency ranks second in frequency after mitral valve defects. Usually combined with stenosis of the aortic lumen. More often found in boys.
Consequences of tricuspid valve dysfunction
The prognosis for progressive stenosis or insufficiency of the right atrioventricular valve is extremely unfavorable. According to statistics, most patients develop complications of cardiac pathology within 5-10 years. The most dangerous of them: thromboembolism of the pulmonary vessels with a thrombus from the AV valve or fatal atrial fibrillation (arrhythmia). Cardiac arrest can be triggered by complete blockade or secondary infection in the presence of a defect.
Progressive pathology of the tricuspid valve is complicated by congestive heart failure with damage to the liver and blood vessels of the internal organs. This increases the risk of developing gastrointestinal bleeding from portal hypertension from the esophageal veins.
Treatment of tricuspid insufficiency
If first degree tricuspid valve insufficiency is detected, no treatment is prescribed. At this stage, the heart itself copes with the defect that has arisen and does not fail due to compensation mechanisms.
In later stages, when symptoms appear, drug treatment is prescribed to reduce signs of heart failure. The following may be prescribed: beta-blockers, cardiac glycosides, anticoagulants, diuretics and other drugs that the cardiologist selects individually, taking into account the condition.
In later stages, surgical treatment is recommended, which includes several types of surgery: reconstruction of the tricuspid valve or replacement of a poorly functioning valve with an artificial or biological prosthesis.
conclusions
The basis of prevention for tricuspid valve pathology is timely examination and treatment. Drug therapy can be effective only in the early stages. If valvular dysfunction is detected late, surgical intervention is indicated. As a rule, the life expectancy of a patient with tricuspid stenosis is no more than 20 years, with insufficiency - 25-30. Currently, successful implantation, plastic surgery, correction or prosthetic valve replacement is carried out surgically, which makes it possible to prevent dangerous complications, death and prolong the patient’s life.
Place of the bicuspid valve among aortic defects
The incidence of bicuspid aortic valve detection among children reaches 20 cases per thousand newborns. In adults it is 2%. For most people, two valves are enough to ensure normal blood circulation throughout a person’s life and do not require treatment.
On the other hand, when examining children with congenital heart disease in the form of aortic stenosis, up to 85% of cases reveal a variant of the bicuspid aortic valve. In adults, similar changes are found in half of the cases.
The “throughput” area of the aortic opening depends on the options for valve fusion.
Usually one of the two valves is larger than the other, the opening has an asymmetrical appearance like a “fish mouth”
If the congenital pathology of heart disease is “layered” with causes of an infectious nature, atherosclerosis of the aorta, then the valves fail faster than usual and undergo fibrosis and calcification.
How does valvular insufficiency manifest?
Symptoms of incomplete closure of the aortic valve begin to appear if the reverse flow of ejected blood reaches 15–30% of the volume of the ventricular cavity. Before this, people feel good, even play sports. Patients complain about:
- heartbeat;
- headaches with dizziness;
- moderate shortness of breath;
- feeling of pulsation of blood vessels in the body;
- angina pain in the heart area;
- tendency to faint.
With decompensation of the cardiac adaptation mechanisms, the following appears:
- dyspnea;
- swelling in the limbs;
- heaviness in the hypochondrium on the right (due to stagnation of blood in the liver).
During the examination, the doctor notes:
- pale skin (reflex spasm of peripheral small capillaries);
- pronounced pulsation of the cervical arteries and tongue;
- change in pupil diameter in accordance with the pulse;
- In children and adolescents, the chest protrudes due to strong heartbeats into the non-ossified sternum and ribs.
Intensified beats are felt by the doctor when palpating the heart area. Auscultation reveals a typical systolic murmur.
Blood pressure measurement shows an increase in the upper number and a decrease in the lower one, for example, 160/50 mmHg. Art.