What does immunoglobulin g mean? Igg immunoglobulins make up about 75% of serum immunoglobulins and 10-20% of total serum protein. They are produced by mature B lymphocytes. Immunoglobulins g are the main antibodies that are produced upon secondary contact with an antigen. Laboratory assistants do a blood test for immunoglobulin G using the immunoturbidimetric method.
Therapists at the Yusupov Hospital prescribe a blood test for immunoglobulin g to diagnose many diseases. The results of the study are interpreted by professors and doctors of the highest category. All complex cases of disease are discussed at a meeting of the expert council. Immunologists prescribe modern drugs registered in the Russian Federation, which allow normalizing the concentration of immunoglobulin G.
Detailed description of the study
The main function of the immune system is to protect the human body from infections and various cancers and autoimmune diseases. Normally, it is carried out with the help of cells (leukocytes, macrophages, etc.) and special proteins - immunoglobulins (antibodies): IgA, IgM, IgD, IgE and IgG. This test is aimed at identifying the amount of IgG in the blood.
Immunoglobulin class G (IgG) is a protein from the gamma globulin fraction, which is formed by mature B lymphocytes - plasma cells. IgG is the main representative of immunoglobulins in serum: its level in it is about 75-80% of all antibodies and 10-20% of the total amount of protein in the blood. IgG consists of 4 subclasses: IgG1, IgG2, IgG3 and IgG4.
The functions of class G immunoglobulins are diverse. IgG promotes the death of foreign microorganisms by enhancing phagocytosis of macrophages and activating a special complex of proteins (complement system). A feature of IgG antibodies is that they are predominantly produced during a secondary immune response, when a foreign molecule enters the body again. This means that IgG contributes to long-term immune protection against various pathogens and their toxins.
IgG immunoglobulins are the only class of antibodies that can pass through the placental barrier (the filter between the mother and fetus during pregnancy). This unique property provides the newborn child with “passive” (maternal) immunity, which in the first months of life cannot yet produce antibodies. By 3-6 months of a child’s life, the level of maternal IgG gradually decreases: his body gains the ability to produce its own immunoglobulins in sufficient quantities.
The main pathologies associated with IgG appear against the background of its excess or insufficient quantity.
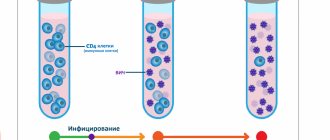
IgG deficiency is accompanied by a more frequent development of infectious diseases, usually purulent bacterial infections. The deficiency of these antibodies can be primary, for example, in general variable immunodeficiency, which is accompanied by a reduced amount of all classes of immunoglobulins (hypogammaglobulinemia) or only IgG. Also, a deficiency of IgG in the blood can be caused by acquired immunodeficiency, for example, due to HIV infection.
Excessive levels of IgG in the blood serum can be observed against the background of chronic and recurrent infectious diseases (usually the ENT organs and respiratory system), autoimmune diseases and clonal gammopathies. The latter are a pathology in which B-lymphocytes degenerate into tumor cells and begin to uncontrollably produce immunoglobulins of one (monoclonal gammopathy) or several (polyclonal) classes. The most common (≈75-80%) monoclonal IgG type of multiple myeloma.
In the Gemotest laboratory, the quantitative determination of IgG is carried out using the immunoturbidimetry method, which is based on determining the concentration of IgG proteins using modern automatic analyzers. You can also undergo a comprehensive study of humoral immunity and immune status. When diagnosing multiple myeloma, this test is recommended to be taken together with a test of abnormal proteins - immunofixation or paraprotein typing in the blood serum.
Preparing for a blood test
Blood is drawn from a vein in the morning on an empty stomach. If the procedure is performed at another time, the interval after eating should be at least 3-4 hours. On the eve of the study, it is recommended to refrain from drinking alcohol and excessive stress on the body. A few days before blood sampling, the doctor recommends that you stop taking medications that may affect the test results.
It is recommended not to smoke in the last 3 hours before donating blood. Blood is drawn from the ulnar vein. Biological material is stored and transported in sealed tubes at an air temperature of +2 to +4° C. Research results can be obtained within 24 hours. They are interpreted by doctors at the Yusupov Hospital.
IgG antibodies
The main role of IgG antibodies is the long-term protection of the body from most bacteria and viruses - although their production occurs more slowly, the response to an antigenic stimulus remains more stable than that of IgM class antibodies.
Levels of IgG antibodies rise more slowly (15-20 days after the onset of illness) than IgM antibodies, but remain elevated longer, so they may indicate a long-standing infection in the absence of IgM antibodies. IgG may remain at low levels for many years, but upon repeated exposure to the same antigen, IgG antibody levels rise rapidly.
For a complete diagnostic picture, it is necessary to determine IgA and IgG antibodies simultaneously. If the IgA result is unclear, confirmation is carried out by determining IgM. In case of a positive result and for an accurate diagnosis, a second test, done 8-14 days after the first, should be checked in parallel to determine the increase in IgG concentration. The results of the analysis must be interpreted in conjunction with information obtained in other diagnostic procedures.
IgG antibodies, in particular, are used to diagnose Helicobacter pylori, one of the causes of ulcers and gastritis.
Types of diseases
This syndrome can be either primary (genetically determined) or secondary (appears due to external factors or diseases).
Primary immunodeficiency in children - what is it and where does it come from?
Congenital immunodeficiency (ID) in a child is something that develops due to genetic factors; these are primary disorders of the immune system. As a result, severe infections develop that quickly become chronic, and organs and tissues are affected by inflammatory processes. Without treatment, primary immunodeficiency leads to death in children from complications of various infectious diseases.
Symptoms of primary immunodeficiency may not be detected in children because the disease does not have unique features. This may be a simple but often recurring infection, for example of the lungs or ENT organs, or problems with the gastrointestinal tract, inflammation of the joints. Often neither parents nor doctors realize that all these problems are the result of a defect in the child’s immune system. Infectious diseases become chronic, complications appear, and there is no response to a course of antibiotics. Typically, severe forms of immunodeficiency are visible immediately after the birth of the baby or after some time. Source: Doan Thi Mai Recurrent infections in children - the risk of immunodeficiency // Pediatrician, 2021, vol. 8, special issue, pp. 109-110
It is important to distinguish primary immunodeficiency from AIDS. The second is a viral, acquired disease, and the primary form is already “implanted” into the body due to genetic defects.
Why does a child develop secondary immunodeficiency, and what is it?
Such a disease is also a disorder in the functioning of the immune system; it appears in children and adults and is not the result of defects in genes. Secondary immunodeficiency can be caused by a number of factors - external and internal. Any external unfavorable factors that disrupt the metabolic process in the body can lead to the development of such a pathology. The most common of them:
- poor environment, dirty air;
- ionizing radiation, microwave exposure;
- acute poisoning in chronic form;
- long course of certain medications;
- chronic fatigue, stress. Source: M.V. Kudin, S.A. Sergeeva, A.V. Skripkin, Yu.N. Fedorov Prevention of morbidity in children with secondary immunodeficiency in disadvantaged environmental regions // Bulletin of VolSMU, 2009, No. 1(29), pp. 87-95
All these factors have a complex effect on the body and all its systems, including the immune system. And such as ionizing radiation, selectively inhibit the hematopoietic system. People living in conditions of environmental pollution have reduced immunity, they are more likely to suffer infections, and the risk of developing cancer increases. .
Prevention methods
ID is easier to prevent than to treat. It is important to remember that the condition of the child directly depends on how correctly the pregnancy was planned. If one of the parents has problems with immunity, he must undergo special procedures to exclude a similar pathology in the child.
In the first six months of life, only breastfeeding is recommended, because breast milk contains all the necessary elements that contribute to the development of full immunity. If there is no lactation, you need high-quality artificial mixtures, but always supplemented with multivitamins.
Sources:
- Doan Thi Mai. Recurrent infections in children - the risk of immunodeficiency // Pediatrician, 2021, v. 8, special issue, pp. 109-110.
- M.V. Kudin, S.A. Sergeeva, A.V. Skripkin, Yu.N. Fedorov. Prevention of morbidity in children with secondary immunodeficiency in disadvantaged ecological regions // Bulletin of VolSMU, 2009, No. 1(29), pp. 87-95.
- G.A. Samsygina, G.S. Koval. Problems of diagnosis and treatment of frequently ill children at the present stage // Pediatrics, 2010, v. 89, no. 2, pp. 137-145.
The information in this article is provided for reference purposes and does not replace advice from a qualified professional. Don't self-medicate! At the first signs of illness, you should consult a doctor.
Normal value for immunoglobulin G
The following reference values have been established for IgG:
| Age | Floor | IgG, g/l |
| 0 – 1 month | Male | 3,97 – 17,65 |
| Female | 3,91 – 17,37 | |
| 1 – 12 months | Male | 2,05 – 9,48 |
| Female | 2,03 – 9,34 | |
| 1 – 2 years | Male | 4,75 – 12,1 |
| Female | 4,83 – 12,26 | |
| 2 – 80 years | Male | 5,4 – 18,22 |
| Female | 5,52 – 16,31 |
Note: It should be noted that each laboratory has the right to establish its own range of normal values. It is advisable to take tests and undergo treatment at the same medical institution.
Factors of influence
There are factors that can distort test results:
- intense sports activities;
- excessive stress and worry;
- taking alcohol or drugs, smoking;
- long-term use of drugs to enhance immunity;
- taking certain medications: carbamazepine;
- phenytoin;
- methylprednisolone;
- hormonal drugs (estrogen, oral contraceptives);
- valproic acid;
- gold preparations;
- cytostatics;
- immunosuppressants (drugs for artificial suppression of immunity);
It is advisable to assess the state of general immunity and diagnose pathologies after a comprehensive study of immunoglobulins of all classes.
Treatment of the disease
The primary form of the disease involves:
- avoiding contact with possible sources of infection.
- during periods of remission, the child can and should lead a normal life, maintain hygiene, and attend an educational institution.
- if there is a threat of infection, broad-spectrum antibiotics are prescribed.
- If there is an effect, the child should be treated for about 3-4 weeks while taking antiviral and antifungal agents. Sometimes antimicrobial treatment lasts for years.
Immunodeficiency can be corrected using immunoreconstruction, replacement treatment, and immunomodulators. In the primary form of the pathology, immunoglobulins are used; in the secondary form, immunotropics, replacement therapy, and immunization are used.
In case of primary pathology, it is extremely important to isolate the child from all sources of infection. When there are no exacerbations of infections, the child can lead a normal life. In case of primary immunodeficiency against the background of a general deficiency of antibodies, children cannot be vaccinated against:
- measles;
- mumps;
- polio;
- rubella;
- chicken pox;
- tuberculosis.
Those living with the child can only be vaccinated with inactivated vaccines.
Antimicrobial treatment consists of taking broad-spectrum antibiotics. If there is no rapid response to therapy, the drug is changed. If there is an effect, then the child should take the antibiotic for at least 3-4 weeks. Medicines are administered intravenously or parenterally. At the same time, antifungal drugs are prescribed and, if indicated, antiviral, antiprotozoal, and antimycobacterial drugs. Antimicrobial therapy can even be lifelong.
For influenza against the background of ID, oseltamivir, remantadine, zanamivir, amantadine, and neuraminidase inhibitors are usually prescribed. If a child gets chickenpox or herpes, acyclovir is prescribed; parainfluenza requires taking ribavirin. Before dental treatment or surgery, the child must take a course of antibiotics to prevent infection.
In cases of severe secondary or primary T-cell ID, Pneumocystis pneumonia should be prevented, depending on blood test results. For this, doctors usually prescribe trimethoprimsulfomethaxozole.
Important! Any medications should only be prescribed by a doctor; self-medication is deadly for a child!
Methods for correcting immune deficiency:
- replacement treatment;
- reconstruction of immunity;
- immunomodulation.
Immunoreconstruction involves transplanting bone marrow or stem cells obtained from umbilical cord blood. In case of primary ID, replacement therapy most often involves taking allogeneic immunoglobulin, which in recent years has been commonly administered intravenously.
Treatment of children with primary ID with common defects in antibody production
In this case, replacement therapy with immunoglobulins, which are administered intravenously, and antibiotics is carried out. Immunoglobulins are administered once every three to four weeks for life. Continuous antibiotic therapy is needed to prevent bacterial infections.
When a bacterial infection worsens, broad-spectrum antibiotics administered parenterally are prescribed. In case of hyper IgM syndrome and common variable immune deficiency (CVID), you need to constantly take antifungal and antiviral drugs. They can be assigned in courses. This is determined by the doctor individually. If a child has X-linked hyper IgM syndrome, then a bone marrow transplant from an HLA-identical donor is indicated.
Immunoglobulin test price
| Service | Price according to Price |
| Immunoglobulin G (IgG) | 400 rub. |
| Immunoglobulin M (IgM) | 400 rub. |
| Immunoglobulin A (IgA) | 400 rub. |
| Immunoglobulin e (Ige) | 500 rub. |
| Immunoelectrophoresis-screening (differentiation of gammopathy: lambda chains, kapa chains of immunoglobulins) | 2200 rub. |
| Immunoelectrophoresis (complex study) with quantitative determination: includes differentiation of gammopathy: lambda chains, kappa chains of immunoglobulins electrophoretically (immunofixation) + quantitative determination Immunoglobulins IgG, IgM, IgA | 46800 rub. |
Why is an elevated level of immunoglobulin dangerous?
Immunoglobulin IgE is a structural part of the body's natural immune defense. Its initial role is to neutralize pathogenic organisms (bacteria, viruses and helminths) on mucosal surfaces. They attract immunoglobulins G, eosinophils, neutrophils and other biologically active substances to the area where pathogens invade, getting rid of the threat. Therefore, it would be incorrect to talk about the harm of IgE during the normal functioning of the immune system.
A completely different picture unfolds with an atypical increase in IgE in response to their reaction with allergens. In this case, the immunoglobulin “raises troops” against a non-existent enemy, and the cells called upon to protect the body attack its own tissues. However, even with its increase, we cannot say that it is IgE that threatens human health. First of all, it is a marker indicating existing disorders that can be corrected under the guidance of a competent doctor.
Treatment methods for secondary ID
Immunotropic therapy is mainly used, which can be of different directions:
- active immunization;
- replacement therapy;
- taking immunotropics.
The choice of immunotropic therapy depends on how acute the inflammatory-infectious process is and what immunological defect is identified. When the symptoms of the disease subside, vaccine therapy can be used for prevention.
Immunoglobulins administered intravenously are used as replacement therapy. Their main active ingredient is special antibodies obtained from donors. Immunoglobulins containing only IgG are often prescribed.
Immunotropic treatment of secondary ID
Using immunomodulators, the effectiveness of antimicrobial therapy can be increased. Immunomodulators should be part of complex therapy together with etiotropic treatment of infection. The doctor calculates the regimen and dosage individually.
Immunological monitoring should be carried out while taking immunomodulators. If the infection is in an acute stage, immunomodulators are used with caution. Otherwise, you can cause a severe general inflammatory response and septic shock as a result. Source: G.A. Samsygina, G.S. Koval Problems of diagnosis and treatment of frequently ill children at the present stage // Pediatrics, 2010, v. 89, no. 2, pp. 137-145
Indications for the study
Indications for a blood test for immunoglobulin E are diseases and conditions associated with this substance. These include:
- dermatographism - a specific skin reaction in the form of urticaria or redness in places that came into contact with hard, blunt objects (literally drawings on the skin), disappearing spontaneously 30-40 minutes after occurrence;
- repeatedly exacerbating dermatitis, widespread throughout the body;
- increased skin sensitivity to household chemicals, cosmetics, food products;
- increased sensitivity to food, expressed by intestinal symptoms or dermatitis;
- long-term exacerbation of sinusitis, rhinitis, bronchitis and attacks of bronchial asthma of unknown origin.
Indications for the study also include:
- an allergic reaction, the source of which cannot be determined from anamnesis, including by keeping a daily diary of an allergy sufferer;
- unclear or questionable results of skin tests that did not give a clear picture of the degree of sensitization to a specific allergen, or giving reason to assume a false negative result;
- impossibility of performing skin tests - history of increased sensitivity to reagents, high risk of anaphylactic shock, taking antihistamines with the impossibility of stopping them even for a short time;
- patient's reluctance to do skin tests.
Also, an analysis for immunoglobulin E is carried out to clarify the diagnosis, when it is necessary to establish the specificity of the allergen and the degree of sensitivity of the body to it. This data is necessary to create an effective treatment plan.
Good to know: The examination is not carried out when skin tests are sufficient to make an accurate diagnosis.
Various classes of antibodies IgG, IgM, IgA
Enzyme immunoassay determines infectious antibodies belonging to various Ig classes (G, A, M). Antibodies to the virus, in the presence of infection, are detected at a very early stage, which ensures effective diagnosis and control of the disease. The most common methods for diagnosing infections are tests for IgM class antibodies (acute phase of infection) and IgG class antibodies (sustained immunity to infection). These antibodies are detected for most infections.
However, one of the most common tests - hospital screening (tests for HIV, syphilis and hepatitis B and C) does not differentiate the type of antibodies, since the presence of antibodies to the viruses of these infections automatically assumes a chronic course of the disease and is a contraindication, for example, for serious surgical interventions. Therefore, it is important to refute or confirm the diagnosis.
A detailed diagnosis of the type and amount of antibodies for a diagnosed disease can be done by taking an analysis for each specific infection and type of antibodies. Primary infection is detected when a diagnostically significant level of IgM antibodies is detected in a blood sample or a significant increase in the number of IgA or IgG antibodies in paired sera taken at an interval of 1-4 weeks.
Reinfection, or repeated infection, is detected by a rapid rise in the level of IgA or IgG antibodies. IgA antibodies have higher concentrations in older patients and are more accurate in diagnosing ongoing infection in adults.
A past infection in the blood is defined as elevated IgG antibodies without an increase in their concentration in paired samples taken at an interval of 2 weeks. In this case, there are no antibodies of classes IgM and A.
Diagnostics of ID
A family history and complaints of the child (if he is not a newborn), an examination, as well as a number of laboratory tests are collected: molecular genetics, clinical blood test, etc.
Important! If the family already has a child with primary immune deficiency, then prenatal diagnosis is extremely important when carrying a second one.
Signs and symptoms of primary immunodeficiency are detected in children already in the first weeks of life. When a doctor collects anamnesis, he pays special attention to the frequent incidence of viruses and bacterial infections, to heredity aggravated by disorders of the immune system, to congenital malformations.
Often such pathology is detected much later and by chance, when other tests are performed.
The main methods for diagnosing both congenital and acquired disorders of the immune system:
- examination of the child, during which special attention is paid to the condition of the skin, as there may be fungal infections, erosions, dystrophy, ulcers, swelling of different parts of the body;
- blood tests - pathology is indicated by a violation of the leukocyte formula;
- special immunological studies;
- molecular genetic analysis.
IgM antibodies
Their concentration increases soon after the disease. IgM antibodies are detected as early as 5 days after onset and reach a peak between one and four weeks, then decline to diagnostically insignificant levels over several months, even without treatment. However, for a complete diagnosis, determining only class M antibodies is not enough: the absence of this class of antibodies does not indicate the absence of the disease. There is no acute form of the disease, but it may be chronic.
IgM antibodies are of great importance in the diagnosis of hepatitis A and childhood infections (rubella, whooping cough, chickenpox), easily transmitted by airborne droplets, since it is important to identify the disease as early as possible and isolate the sick person.