To the reference book Wegener's granulomatosis involves damage to the upper respiratory tract.
Author:
- Oganesyan Tigran Sergeevich
ENT pathology expert
5.00 (Votes: 1)
Wegener's granulomatosis is a granulomatous vasculitis characterized by damage to the upper respiratory tract, first described in the first third of the 20th century by the German physician Friedrich Wegener, for which it received its name.
The disease is predominantly necrotic in nature; with a long course, the lungs and kidneys are involved in the process.
Clinical picture
There are several forms of pathology - acute, subacute and chronic. The development of the disease also describes three main stages:
- initial - changes in the upper respiratory tract are local in nature (the mucous membranes of the nasal cavity, pharynx, larynx, trachea, and sometimes the middle ear are affected);
- generalized - the process of damage involves internal organs, lungs and kidneys in particular;
- terminal - the most severe, aggravated by the addition of renal, pulmonary and heart failure.
In this regard, patients complain about:
- nasal congestion (usually one half);
- purulent nasal discharge mixed with blood;
- brown-brown crusts form on the mucous membrane, after removal of which it has a thinned appearance and is covered with bleeding lesions.
In the case of further progression of the disease, perforation of the cartilaginous and then the bone part of the septum occurs (saddle-shaped perforation of the nose). After which nearby tissues, especially the paranasal sinuses, are destroyed. A distinctive feature of granulomatosis from syphilis is the absence of destruction of the hard palate, which in this case remains unchanged.
The generalized stage of the pathology is usually diagnosed after several months or even after several years. Damage to the lungs will be marked by the appearance of cough, shortness of breath, and characteristic chest pain. The skin also signals changes occurring in the body; ulcerative necrotic rashes appear on it.
Severe, terminal stage granulomatosis is life-threatening. The symptoms of azotemic uremia are accompanied by signs of pulmonary and heart failure, which together are the cause of death.
Wegener's granulomatosis
Clinical picture:
Initial manifestations may have different localizations, but usually they relate to the upper respiratory tract. The patient consults a doctor with symptoms of rhinitis, sinusitis, severe difficulty in nasal breathing, otitis media and blockage of the auditory tube. Ear pain and significant hearing loss are possible. During the examination, granulomatous ulcerative growths are detected in the area of the nasopharynx, nasal septum, mucous membrane of the sinuses, soft and hard palate. Fever, weakness, and loss of appetite are common. A number of patients from the very beginning of the disease have signs of pulmonary involvement in the process - cough, chest pain, shortness of breath, hemoptysis. Life-threatening profuse bleeding is rare. In some cases, lung lesions occur in later stages of the disease. X-ray signs of pulmonary pathology are very diverse: single or multiple nodes, infiltrates, cavities, focal atelectasis, exudative pleurisy, pneumothorax. Enlargement of the mediastinal lymph nodes is uncharacteristic.
The airways (upper or lower sections or combined changes) are affected in all patients with Wegener's syndrome, and the sinuses are involved in the process in 90%. Granulomatous sinusitis itself is often complicated by secondary purulent infection, which requires additional active antibiotic therapy and is often incorrectly assessed as an exacerbation of the underlying disease.
Often the first signs of damage to the nasopharynx are very modest, and only after a few months do symptoms of a systemic disease develop. Individual patients are described in whom generalization of the disease occurs several years after the onset of its first mild manifestations. The progression of nasopharyngeal lesions with the spread of granulomatous tissue can lead to destruction of the nasal septum and retraction of the nasal dorsum (“saddle nose”), compression of the orbit and bulging of the eyeball forward and downward (proptosis) due to retrobulbar granulomatous inflammation, destruction of tissue of the eyeball and orbit. At the same time, perforation of the hard or soft palate is not typical for Wegener's granulomatosis and gives reason to suspect the presence of a so-called midline granuloma (see below).
Kidney damage occurs in 80-90% of patients, and the appearance of corresponding symptoms is often the first sign of generalization of the disease. Changes in urine tests correspond to those in acute glomerulonephritis (hematuria, proteinuria); biopsy in most cases reveals focal glomerulonephritis. Approximately 10% of patients have a picture of rapidly progressing glomerulonephritis with the development of azotemia and the discovery of necrotic changes in the glomeruli on biopsy and the formation of many proliferative “crescents”. In a number of patients, nephrotic syndrome occurs as a consequence of glomerular lesions (in contrast to classic periarteritis nodosa, in which this syndrome is usually the result of renal vein thrombosis).
Typical histological changes in biopsied renal tissue are sometimes found in patients without any clinical and laboratory signs of kidney damage.
Eye damage (iritis, conjunctivitis, dacryocystitis, granulomatous episcleritis, sclerouveitis, perforating scleromalacia, cavernous sinus thrombosis, proptosis) occurs in almost 50% of patients, i.e. much more often than with polyarteritis. In rare cases, retrobulbar granulomatous proliferation and retinal artery thrombosis have resulted in blindness.
Almost as often, skin changes are observed - mainly petechial hemorrhages, localized mainly on the extremities. Nodular eruptions, vesicles, or necrotic ulcerations are rarely observed.
Arthralgia and short-term, completely reversible (even without treatment) arthritis of predominantly large joints are observed in 50-60% of patients, more often in the early stages of the disease. Occasionally, longer lasting arthritis of small joints mimicking RA is observed.
Heart pathology (arrhythmias, clinical and electrocardiographic symptoms of coronary insufficiency, rarely pericarditis) is recorded in no more than 1/3 of patients.
In 20% of patients, changes in the nervous system . Peripheral neuropathies do not differ from those with polyarteritis nodosa. Intracranial spread of granulomatous tissue from the nasopharynx and sinuses can lead to pathological symptoms in some structures of the base of the brain, in particular the pituitary gland (diabetes insipidus syndrome) and cranial nerves.
Much less frequently, vasculitis and granulomatosis are localized in other organs (intestines, liver) with corresponding clinical symptoms. The correct interpretation of these changes is facilitated by the accompanying typical signs of the disease.
Causes and course of the disease
Currently, the causes of this disease are not fully understood, but most researchers are of the opinion that it is an autoimmune disease, in the occurrence of which viruses such as cytomegalovirus and herpes virus play an important role.
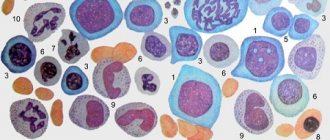
An equally important factor is the genetic peculiarity of the immune system, especially since with this disease in the blood of patients there is an increased content of the HLA-A8 antigen, which is responsible for the genetic predisposition to the development of autoimmune diseases. In the pathogenesis of Wegener's granulomatosis, immunological disorders such as deposition of immune complexes in the walls of blood vessels and impaired cellular immunity are of great importance. Patients experience necrotizing vasculitis, which affects medium- and small-caliber arteries and is accompanied by the formation of polymorphic cell granulomas that contain giant cells.
Medicines
When treating the disease use:
- "Cyclophosphamide", "Methotrexate" and "Azathioprine", which are part of the group of cytostatics.
- "Dexamethasone" and "Prednisolone" are part of the group of glucocorticoids.
- Anticytokine therapy.
- Hemodialysis, cascade plasma filtration, extracorporeal pharmacotherapy, plasmapheresis.
- Antibiotics, which are prescribed to prevent the occurrence of infectious complications.
- Immunoglobulins. May be prescribed if there is a relapsing course of the disease.
Treatment
If you seek help from specialists in a timely manner, surgical intervention is usually not required. Combination therapy with hormones is carried out, the main ones of which are cytostatics and glucocorticosteroids. For a complete cure, long-term and constant use is required. In case of complications of the disease, Wegener's granulomatosis, treatment involves surgery. Otherwise, under such circumstances, the disease may progress and spread to other organs.
Forms of the disease
Depending on the extent of the spread of pathological changes, two forms of Wegener's granulomatosis are distinguished:
- localized. The upper part of the respiratory system is predominantly affected, which is manifested by hoarseness of voice, frequent nosebleeds, the formation of bloody crusts in the nasal cavity, and persistent rhinitis;
- generalized. Characterized by extensive systemic manifestations (fever, abscess pneumonia, joint and muscle pain, increasing signs of renal, cardiovascular and respiratory failure).
The prognosis for Wegener's granulomatosis in the absence of adequate and timely treatment is extremely unfavorable. More than 90% of patients die in the first two years from the moment of diagnosis.
Differential diagnosis
For the purpose of correct diagnosis, diseases that also occur with pulmonary-renal syndrome should be excluded: microscopic polyangiitis, Churg-Strauss syndrome, periarteritis nodosa, Goodpasture syndrome, hemorrhagic vasculitis, systemic lupus erythematosus; rarely - streptococcal pneumonia with glomerulonephritis. A differential diagnosis is also carried out with other diseases: lymphoid granulomatosis, angiocentric malignant lymphoma, malignant tumors, median granuloma of the nose, sarcoidosis, tuberculosis, berylliosis, systemic mycoses, syphilis, leprosy, AIDS, etc. With a predominantly renal course, differential diagnosis is carried out with idiopathic rapidly progressive glomerulonephritis .
Diagnostics
In patients with a developed clinical picture, the diagnosis is usually simple, but due to the variety of forms and course options, difficulties arise in the early stages of the disease. Approximately 25% of patients in the initial stage have no signs of lung or kidney damage.
Classification criteria for the diagnosis of Wegener's granulomatosis
| Criterion | Definition |
| 1. Inflammation of the nose and mouth | Ulcers in the mouth. Purulent or bloody discharge from the nasal cavity |
| 2. Changes in X-ray examination of the lungs | Nodules, infiltrates or cavities |
| 3. Changes in urine | Microhematuria (>5 red blood cells per field of view) or accumulations of red blood cells in urine sediment |
| 4. Biopsy | Granulomatous inflammation in the arterial wall or in the perivascular and extravascular spaces |
If two or more criteria are present, the sensitivity of diagnosis is 88% and the specificity is 92%. To confirm the diagnosis, the presence of classical antineutrophil cytoplasmic antibodies (cANCA) in the blood is determined.
Material and methods
The pathomorphological features of vascular lesions were studied in 11 people who died from GPA aged 16 to 74 years. Among the patients, men predominated (8 cases). The professional composition was as follows: workers - 2, students - 2, livestock specialist - 1, machinist - 1, pharmacist - 1, employee - 1, housewife - 1, pensioner - 1, student - 1. The duration of the disease ranged from 1 month to 4 years , the course of the disease was acute in four cases, subacute in two and chronic (with periods of exacerbation and remission) in five observations.
Forecast for the development of the disease
The transition of granulomatosis from the initial stage to the terminal stage occurs over a short period.
Moreover, in almost all cases, the infected organism is prone to complications. Among the large number of patients at a late stage there are:
- destruction of facial cartilage and bones;
deafness and blindness;- hemoptysis;
- formation of granulomas;
- gangrene of the foot;
- additional infections;
- renal failure.
Lack of therapy in 97% of cases has an unfavorable prognosis: patients die within a period of six months to two years.
The course of the local form of the disease is benign. Immunosuppressive therapy helps improve the overall state of remission in 80% of patients. In half of the patients, a new exacerbation occurs after a long period.
conclusions
Thus, therapy for Wegener's disease (granulomatosis) is complex and takes a long time until stable remission is achieved. If the case is severe, then immunosuppressive treatment should be combined with combined pulse therapy in the presence of glucocorticoids. Severe complications of drug therapy can be avoided by extracorporeal hemocorrection. Cryomodification of autoplasma is currently popular among rheumatologists and hematologists. This procedure allows you to avoid further progression of the disease, and also allows you to reduce the dose of cytostatics taken by the patient.
Such methods of therapy, together with traditional treatment, can quickly improve the condition of patients and achieve remission.
Causes and risk factors of Wegener's disease
The cause of the disease is unknown.
Wegener's granulomatosis is thought to result from an abnormal response of the immune system to certain triggers. This reaction leads to inflammation, the formation of granulomas, and narrowing of the lumen of blood vessels. Scientists believe that infections may be such triggers, but a specific infection has not yet been identified. Wegener's disease can occur at any age, but most often develops after 40 years of age. Whites are more likely to develop Wegener's granulomatosis than blacks and other races.
Stages of the disease
In the clinical picture of Wegener's granulomatosis, several stages are distinguished:
- Rhinogenic granulomatosis (granulomatous-necrotizing vasculitis). Ulcerative-necrotic or purulent-necrotic rhinosinusitis, nasopharyngitis, laryngitis, destructive changes in the orbit and nasal septum develop.
- Pulmonary granulomatosis. The pathological process affects the lung tissue.
- Generalized granulomatosis. The lower parts of the respiratory system, cardiovascular system, digestive tract and kidneys are affected.
- Terminal granulomatosis. Renal and (or) pulmonary failure develops. Death occurs within a year from the moment the disease enters the terminal stage.
Description of the pathology
In the walls of blood vessels, Wegener's disease (photo in the article) is characterized by giant cell granulomatous-necrotizing inflammation. First of all, the formation of granulomas occurs in the vessels and tissues that surround the respiratory tract and eyes, after which they begin to develop in the kidneys, skin, heart and nervous system.
Granulomatosis received its name thanks to its discoverer, who identified this systemic vasculitis as a separate nosology. This happened in the thirties of the last century.
There are several forms of Wegener's disease (we'll look at the symptoms later).
Local form
In the local form, an inflammatory process is observed in the nasal mucosa, in the paranasal sinuses, in the pharynx and larynx, in the trachea, in various parts of the visual and auditory analyzers. Patients suffer from constant rhinorrhea and periodic nosebleeds. In addition, nasal breathing is impaired, bloody crusts form in the nose, and the voice becomes hoarse. Many scientists consider the local form of granulomatosis as an independent disease, which is characterized by dominant lesions of the skin and respiratory organs.