Among the laboratory techniques designed to assess the characteristics of red blood cells (erythrocytes - Er), not the least role belongs to the coloring of the smear and its morphological examination. Although, before the drug comes under the microscope lens, a person or machine (automatic hematology analyzer) will count red blood cells and determine the level of red blood pigment - hemoglobin (Hb). Having noticed some discrepancy, namely, a decrease in the level of hemoglobin in the blood with a normal content of red blood cells, the doctor, based on the data obtained, can calculate the color index (CI) and in case of its reduced value (below 0.8), without waiting for viewing the smear, give an unambiguous answer – hypochromia
. Of course, to establish a diagnosis, this answer cannot be final, but it will become an additional guideline for microscopic examination.
Hypochromia in a general blood test (CBC) indicates the development of hypochromic (mainly microcytic) anemia.
However, if the development of anemic syndrome is suspected, not only quantitative, but also qualitative (morphological) changes in the red blood must be taken into account.
Before morphological examination
Typically, various indices, including the color index (CI), characterizing the state of red blood cells, are calculated before the doctor begins a visual assessment of the smear. However, if MCH, MCV, MCHC are calculated by a machine, then the CPU is calculated manually by a laboratory employee using a simple and reliable formula:
CP = (Hb, g/l x 3) / first three digits of the total Er content
You can expect the following results from the calculation:
- Normally, CP = 0.85 - 1.05 (normochromia or normochromasia), that is, a normal level of red blood cells that contain hemoglobin in sufficient quantities (no more and no less);
- If the CP values hardly reach (or do not reach at all) up to 0.8, then we are talking about hypochromia
or hypochromasia. This condition is characteristic of hypochromic anemia - the number of cells is within normal limits, but there is no longer enough hemoglobin to ensure functional tasks; - A color indicator that has crossed the border of normal values (up to 1.1) indicates hyperchromasia or hyperchromasia. A significant increase in CP (up to 1.4) is characteristic of pernicious and B12-folate deficiency anemia.
The color index is a digital expression of the content of red blood pigment in relation to the red blood cell. An insufficient amount of Hb and a decrease in CP (hypochromia) gives reason to assume an iron deficiency state (IDA) of various origins or sideroachrestic anemia, which is formed due to a violation of heme synthesis in young, nucleated cells of the erythroid series - erythroblasts. These anemic conditions are included in the group of hypochromic anemias.
At the same time, it is very important not to doubt the veracity of all calculations and determinations of red blood parameters, because how reliably the CP value will be calculated depends on the accuracy of determining the level of hemoglobin and the number of red blood cells - these are the parameters that belong to the dominant criteria for anemic syndrome.
Why does it occur
The causes of hypochromia can be different, and most often they are caused by the following diseases:
- Iron-deficiency anemia;
- thalassemia;
- hemolytic anemia;
- lead intoxication;
- other congenital anemias caused by impaired globin synthesis.
Anemia in which hypochromic red blood cells are found in the blood is called hypochromic. In addition, an assessment of the color index of the blood is necessary. In this case, the CPU is reduced and is less than 0.85, while its normal value is 0.85-1.05. Hypochromia, as a rule, is combined with microcytosis - a decrease in the volume of red cells, which causes a decrease in hemoglobin content.
Machine gun and doctor's eyes
Red blood cell counting (quantitative analysis performed in a hematology analyzer or Goryaev chamber) still does not provide comprehensive information about the state of red blood cells
. In any case, especially if some pathology is suspected, a machine cannot replace a doctor’s eyes, so in any hematology laboratory, after counting and obtaining “dry numbers”, a more informative morphological (qualitative) analysis will follow. This study allows you to comprehensively examine a smear, determine the size of red blood cells (after they are calculated by an automatic device or, if one is not available, the doctor will do this instead) and see with your own eyes the degree of saturation of red blood cells with the red blood pigment - hemoglobin.
Hypochromic anemia (due to iron deficiency), as a rule, is indicated by the following morphological signs:
- Hypochromia or absence of any color at all (anulocytes);
- Often hypochromia and microcytosis;
- The appearance of fragments of red blood cells, which are called schizocytes, and young cells (precursors of reticulocytes) - normoblasts;
- Polychromatophilia - the presence in a smear of red blood cells stained with both acidic and alkaline (due to the presence of a basophilic substance) dyes;
- No reaction or slight fluctuations in white blood.
Important indicators of CBC are cell size and...
When studying the main characteristics of erythrocytes using an automatic analyzer that calculates the RDW indicator - anisocytosis of erythrocytes and other indices, the doctor still pays attention to cell sizes:
- He classifies normal red blood cells (with a diameter of 7–8 microns) as normocytes
and does not make any marks in their direction if other indicators also correspond to the norm. But it should be borne in mind that for certain types of anemia, cells such as normocytes are quite common; - Red blood cells with a diameter of more than 8 microns are classified as macrocytes
and this is noted in the analysis form (anisocytosis with a predominance of macrocytes); - In the presence of a large number of tiny cells with a diameter much less than 7 microns, often losing the appearance of red blood cells, it is written “microcytosis” and suggests microcytic anemia.
In the absence of automated hematology systems, if an abnormal phenomenon is detected, the laboratory employee will continue to study using the Price-Jones curve.
Changes in childhood
A pathological increase in the number of red blood cells in children is associated with various factors:
- with a low level of oxygen in maternal blood - the anomaly manifests itself in newborns;
- regular exposure of the baby to tobacco smoke (passive smoking);
- living in high mountain areas;
- regular sports activities.
A list of probable sources of deviation in children is presented:
- congenital heart defects;
- bone marrow dysfunction;
- hypertension in the pulmonary circulation;
- blood pathologies;
- obstructive pulmonary lesions with a chronic course;
- acute bronchitis, rhinitis or allergies;
- obesity of the last two degrees;
- dehydration caused by vomiting or diarrhea;
- disruption of the adrenal cortex.
Serious diagnoses associated with changes in the number of red blood cells include cancer of the kidneys and liver. Erythrocytosis is not an independent disease; it indicates latent pathologies or the presence of external influence factors.
...their coloring
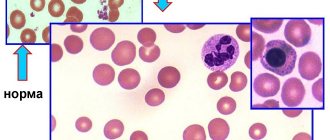
Meanwhile, in addition to the size of red blood cells, there is another, no less important criterion that gives a visual assessment - the intensity of staining of red blood cells:
- Red blood cells, fully (but not excessively!) saturated with hemoglobin, are visible under a microscope as normocytes with a small clearing in the middle of the cell - this is normochromia or normochromasia
, corresponding to a color index in the range of 0.85 - 1.0. And again, normochromia does not mean the absence of pathology; a proportional decrease in red cells and blood pigment is also designated as normochromia, but in fact normochromic anemia occurs; - Excessive saturation of erythrocytes with red blood pigment gives an excessively intense color, erasing the median clearing (CP - more than 1.1) - hyperchromia or hyperchromasia
; - A large median clearing and a narrow rim (ring) outlining the cell indicate hypochromia of erythrocytes or hypochromasia
(the greater the clearing, the greater the degree of anemia). This means that red blood cells (they are called anulocytes) are poorly saturated with red blood pigment, therefore, they will perform their main functional duties (delivering oxygen to tissues and organs) poorly.
A laboratory diagnostic doctor, having conducted a morphological study of red blood cells and seen changes in red blood cells (and this will certainly happen if most of the cells for some reason have changed their characteristics - size and color), will suspect the development of an anemic condition, which will be reflected in his conclusion. However, the topic of this work is hypochromia, so let’s return to it...
Red blood cell staining intensity
An important criterion for assessing red blood cells is the intensity of their staining:
- Normochromia (normochromasia), when red blood cells saturated with Hb look like normal cells with a small bright spot in the middle of the cell, the CP is in the range of 0.85-1.0. This condition does not always correspond to the norm; it can be observed with normochromic anemia.
- Hyperchromia (hyperchromasia), when the median clearing does not differ from the rest of the erythrocyte due to excessive saturation with pigments. The CPU is more than 1.1.
- Hypochromia (hypochromasia), when the median clearing is excessively large, and the rim of the cell is very narrow due to poor saturation with red pigment. The condition is characterized by poor performance of erythrocytes’ functions.
The doctor, having assessed the characteristics of red blood cells during a morphological study, will identify anemia and reflect the diagnosis by drawing up a conclusion.
Degree of hypochromia. Relation to microcytosis
Thus, it is clear that hypochromia of erythrocytes means weak staining of the cells (a sign of hypochromia is the median clearing increasing in diameter) as a result of their insufficient saturation with red blood pigment.
hypochromia with microcytosis in the blood
Hypochromia, being a decisive sign of the development of hypochromic anemia, has different degrees of severity:
- 1st degree - the cell is well colored on the periphery, but the clearing zone in the center shows slight hypochromia;
- 2nd degree - the clearing in the center expands, tending closer to the membrane, but the area filled with paint is clearly visible, which indicates moderate hypochromia;
- 3rd degree - the color is located only at the membrane itself, it is actually not visible, so it seems that this is not an erythrocyte at all, but... some kind of pale ring. A similar situation occurs with advanced forms of anemia and indicates its severe course.
Hypochromia of erythrocytes is evidence of the development of hypochromic anemia, but for some reason at the beginning of our work we talked about another characteristic of red blood cells - their size? So, in the vast majority of cases, hypochromia and microcytosis are inseparable; they are the main symptom of hypochromic microcytic anemia. In addition, the importance of these two indicators increases if there is a need to differentiate hypochromic microcytic anemia from other conditions or among themselves.
Primary sources of increasing values
Changes of physiological nature are provoked by:
- severe emotional stress;
- severe dehydration;
- long-term sports activities;
- living in high mountain areas.
The pathological form of erythrocytosis is associated with:
- with erythremia - tumor damage to the hematopoietic organs;
- heart defects - when arterial and venous blood is mixed, there is an insufficient supply of oxygen to the tissues; to compensate for the deviation, the bone marrow begins to produce a larger number of red blood cells;
- neoplasms in the kidneys, pituitary gland, adrenal glands or liver - the organs are responsible for the disposal of old elements in the blood, the formation of the disease leads to the cessation of this function, the tests indicate a predominance of mature forms;
- diseases of the respiratory tract and heart, infectious pathologies - a large number of young or reticular types of elements are observed;
- primary pulmonary hypertension;
- Pickwick's syndrome caused by obesity, pulmonary insufficiency, high blood pressure.
Less dangerous sources of development of an increased number of red blood cells include:
- lack of digestive enzymes;
- dehydration due to heat or prolonged physical activity;
- low-quality water: with chlorine, contaminated, highly carbonated;
- vitamin deficiency or deficiency due to liver dysfunction;
- smoking.
Against the backdrop of a large number of reasons causing changes in tests, only a doctor can correctly determine the original source of the deviation.
A reliable sign of hypochromic anemia
So, hypochromia is a reliable sign of hypochromic anemia, which, differing from each other in other laboratory indicators and their origin, also have their own forms. Thus, the group of hypochromic anemias consists of the following anemic conditions:
Iron deficiency anemia (IDA)
IDA is a typical representative of hypochromic microcytic anemia, and also the most common. Diagnostic criteria:
- Hypochromia and microcytosis;
- Decreased CP and serum iron (Fe) levels;
- Drugs intended to treat such conditions have a positive effect.
Iron-saturated anemia (sideroachrestic)
This form is characterized by a normal iron content in the serum, but due to poor absorption it cannot reach the site where heme synthesis occurs (erythroblasts), therefore, the hemoglobin level drops. This form is most often the result of prolonged intoxication with aggressive chemicals or industrial poisons. In addition, the body is pushed towards the development of chronic hypochromic anemia by long-term use of drugs of various pharmacological groups (affecting the components of red blood).
Diagnostic criteria:
- Hypochromia of erythrocytes;
- Decreased hemoglobin levels;
- Iron concentrations are usually normal;
- There is no effect when treated with ferrum-containing drugs.
Iron redistribution anemia
The cause of the development of this form is excessive destruction of red cells (hemolysis), as well as purulent infections or pathological processes localized in the heart (endocarditis) or lungs (tuberculosis). However, all types of hemolytic anemia (HA) are not suitable as an example of chronic hypochromic anemia, although the destruction of red blood cells (and, accordingly, hemolysis) underlies this pathology. Many forms of HA are normochromic, but quantitative thalassemia corresponds to the definition of hypochromic microcytic anemia.
Indicators used for diagnosis:
- Hypochromia of erythrocytes;
- Decreased hemoglobin levels;
- The serum iron content does not leave the normal range;
- Ferrotherapy does not produce a positive effect.
In other cases (in the presence of signs that can be attributed to different types), the form of hypochromic anemia is classified as mixed
.
Meanwhile, each of the forms has its own origin, that is, the reasons for their formation are different.
Causes
Obviously, the cause of hypochromia of erythrocytes is a certain form of hypochromic anemia. Meanwhile, the reasons for the development of each of the options are different (they are described in detail in the relevant sections devoted to a specific type of anemia), but if they are put together, we can identify the main factors that contribute to the formation of an anemic state of the body and the appearance of hypochromia in a general blood test:
- Blood loss that continues for a long time or chronically, for example, gastrointestinal or uterine bleeding, gives rise to the development of chronic hypochromic anemia;
- Impaired absorption of iron in the gastrointestinal tract due to chronic inflammatory processes (enteritis, extensive resection) which also form chronic hypochromic anemia;
- Malignant neoplasms, especially those localized in the gastrointestinal tract (most often stomach cancer);
- Increased need for macro- and microelements, including such a chemical element as iron (pregnancy, breastfeeding, childhood and adolescence);
- Insufficient content of iron and vitamins that facilitate its absorption in food products entering the body (vegetarianism and other diets).
Clinical signs are in correlation with the level of hemoglobin and the severity of hypochromic anemia:
- The first degree of severity of anemia (mild) is noted when the hemoglobin level drops below the physiological norm, but does not cross the limit of 90 g/l;
- Anemia of the second degree of severity (moderate) is established based on the level of hemoglobin in the blood in the range of 70 - 90 g/l, the color index below 0.8 and moderate hypochromia during visual assessment of the smear;
- The third degree (severe) is indicated by hemoglobin levels (below 70 g/l), a noticeably reduced color index and pronounced hypochromia in the smear.
Based on this, it can be noted that the severity of symptoms weakens with a mild degree and manifests itself in full force in the case of severe hypochromic anemia.
Iron deficiency anemia in children
Why are iron supplements necessary for IDA? What are the advantages of the latest generation drugs? Why should iron supplements be taken for a long time?
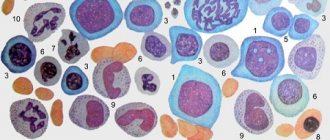
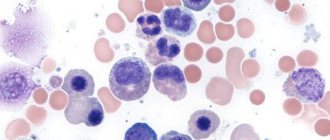
| Blood picture in chronic iron deficiency anemia. Severe hypochromia of erythrocytes, anisocytosis, poikilositosis, schizocils, the presence of polychromatophils |
Anemia is a pathological condition characterized by a decrease in red blood cell mass, often in combination with a decrease in the number of red blood cells per unit volume of blood.
There are many causes of anemia; For children, iron deficiency anemia (IDA) is most typical. IDA is characterized by the presence of small hypochromic red blood cells and depletion of iron stores in the body. The prevalence of iron deficiency in children at an early age, according to WHO, ranges from 17.5 to 30%.
The following reasons for the development of iron deficiency in children can be identified.
- Insufficient iron stores at birth. Premature babies, as well as children from mothers who suffered from anemia during pregnancy, are at risk for developing IDA. The condition of the placenta is also of great importance, since the positive balance of iron in the fetus is due to the perfect transport mechanisms of the placenta.
- Insufficient intake of iron from food and impaired absorption in the gastrointestinal tract. What matters is not so much the iron content in the product, but the efficiency of its absorption and assimilation. Iron is absorbed in the duodenum and jejunum, therefore, with various diseases of the digestive tract (chronic enteritis, malabsorption syndrome), iron deficiency can also develop due to impaired absorption.
- Increased need for iron due to growth, intensive processes of tissue differentiation, maturation of various organs and systems, and an increase in circulating blood volume. The need for iron is especially high during traction, puberty and during the formation of menstrual function in teenage girls.
- Excessive loss of iron by the body. This is primarily blood loss: bleeding of various locations (for diseases of the digestive tract - ulcerative processes, polyps, vascular anomalies, nasal), helminthic infestation, menstruation in teenage girls. Excessive loss of iron can occur with severe allergic manifestations on the skin due to the loss of a microelement with exfoliating epithelium, with frequent acute respiratory viral infections in children, since viruses and bacteria use the child’s iron for their metabolic processes.
It is important to note that in young children the causes of iron deficiency are, as a rule, insufficient iron stores and poor nutrition, and in older children - blood loss and sudden traction.
Pathophysiological aspects
Since iron absorption is limited, most people's dietary intake barely meets the body's current needs; iron deficiency can easily develop as a result of illness or poor nutrition. This process consists of several stages.
Stage 1. Iron loss exceeds iron intake. Against the background of a negative iron balance, its reserves in the bone marrow are gradually depleted. Although serum iron and hemoglobin levels remain normal, serum ferritin levels decrease (below 20 ng/mL). As iron stores are depleted, a compensatory increase in transferrin concentration occurs (as evidenced by an increase in iron-binding capacity).
Stage 2: Depleted iron stores no longer provide erythropoietic function to the bone marrow. While plasma transferrin levels rise, serum iron levels decrease, resulting in an increasing deficiency in red blood cell production. Erythropoiesis is impaired when iron levels are below 50 mcg% and transferrin saturation is below 16%. The concentration of ferritin receptors in the serum increases (more than 8.5 mg/l).
Stage 3. Anemia with apparently normal red blood cells and red blood cell indices.
Stage 4. Development of microcytosis and then hypochromia.
Stage 5: Iron deficiency is accompanied by symptoms of tissue disorders.
Clinical manifestations
The idea of the clinical status of a patient with anemia depends on the underlying disease and the form of anemia (acute or chronic). IDA is a chronic condition. The manifestation of anemia per se is explained using pathophysiological mechanisms. Most symptoms of IDA are a reflection of cardiovascular and gas exchange changes that compensate for the decrease in red blood cell mass. The severity of symptoms depends on the speed of development of anemia (with the slow development of anemia, characteristic of iron deficiency conditions, there is enough time for the full development of compensatory mechanisms) and its duration. Even moderate anemia is often asymptomatic. The child may complain of fatigue, shortness of breath and palpitations, especially after physical activity. In severe anemia, symptoms persist even at rest, and the patient cannot tolerate physical activity. If the hemoglobin level is less than 75 g/L, resting cardiac output increases markedly as both heart rate and stroke volume increase. Symptoms of heart failure develop when myocardial reserve is depleted. Consequently, the severity of the patient’s condition is determined primarily by the severity of cardiovascular disorders.
Symptoms of moderate to severe anemia extend to other organ systems. The patient often complains of dizziness and headaches, tinnitus, and even fainting is possible. The person becomes irritable, sleep is disturbed, and concentration decreases. Because blood flow to the skin is reduced, hypersensitivity to cold may develop. Symptoms also arise from the gastrointestinal tract - a sharp decrease in appetite, dyspeptic disorders (nausea, changes in the nature and frequency of stool), primarily due to the shunting of blood bypassing the vascular bed of the internal organs. In teenage girls, the menstrual cycle is disrupted, which manifests itself in the form of amenorrhea or heavy bleeding.
The main sign of anemia is pale skin. However, its information content is limited by other factors that determine skin color.
Therefore, the most informative sign of anemia is the pallor of visible mucous membranes - the mucous membrane of the oral cavity, the nail bed and the conjunctiva of the eyelids. The color of the skin on the folds of the palmar surface is also considered informative - if they do not differ in color from the surrounding skin, then the patient’s hemoglobin level is usually less than 80 g/l.
The development of pallor of the skin during anemia is explained by two factors: the first is, undoubtedly, a decrease in the level of hemoglobin in the blood, the second is the shunting of blood bypassing the vessels of the skin and other peripheral tissues, which promotes increased blood supply to vital organs. Redistribution of blood flow is one of the important mechanisms for compensating for anemia.
Other clinical symptoms of anemia include the already mentioned tachycardia, significant fluctuations in pulse pressure, systolic ejection murmur over the atria, decreased mental and physical activity, children become irritable, quickly get tired, their sleep is restless, and their appetite is reduced.
With IDA, the usual symptoms of anemia are accompanied by signs specific to iron deficiency. With prolonged iron deficiency, perverted appetite (eating chalk, dirt, paints) and sense of smell appear (like the strong smells of gasoline, paints, varnishes, eating ice (pagophagia), glossitis, cheilitis, koilonychia (thinned, striated, brittle nails) develop. With deficiency iron, the activity of the immune system decreases due to a decrease in the synthesis of IL-2 and T-killers; children are more likely to get ARVI, which, in turn, aggravates the existing iron deficiency.
The diagnosis is confirmed by laboratory data. The criterion for diagnosing IDA is microcytic, hypochromic, normoregenerative anemia. IDA is characterized by anisocytosis, thrombocytosis, decreased serum iron levels (less than 13 mmol/l), total iron-binding capacity of serum is unchanged or increased, serum ferritin level is less than 15 ng/ml, transferrin saturation is less than 16%, erythrocyte protoporphyrin level is increased, Hb level A2 is reduced, irritation of the red line is noted in the bone marrow (erythrocytes: granulocytes = 1:1 - 1:2), a typical lack of iron reserves and ring-shaped sideroblasts in the bone marrow.
The differential diagnostic search includes thalassemia, lead poisoning, anemia in chronic diseases, congenital disorders of iron metabolism (transferrin deficiency, impaired iron utilization, impaired iron reutilization), hemosiderosis, including Goodpasture's syndrome, copper deficiency.
Principles of treatment of IDA in children
- Elimination of the causes underlying the development of iron deficiency.
- Therapy for IDA should be carried out with iron supplements, since it is impossible to compensate for iron deficiency in this condition with diet therapy alone; true iron deficiency is not accompanied by a deficiency of vitamins B12, B6, and folic acid.
- The goal of therapy with iron supplements is to eliminate iron deficiency in the body, and not just to normalize hemoglobin levels, so the treatment period is long (at least 3 months).
- IDA therapy is carried out mainly with oral iron supplements.
- Blood transfusions for IDA are carried out only for health reasons.
Diet therapy for IDA in children
It is now generally accepted that it is impossible to eliminate iron deficiency in the body through diet therapy alone. This is due to the fact that the absorption of iron from food is limited - 1.8-2 mg (no more than 2.5 mg) of iron per day - even with a balanced diet appropriate for age and consumption of sufficient amounts of foods high in iron. (For comparison: a healthy child, depending on age, loses from 0.15 to 0.6 mg of iron per day, a girl during menstruation - 15-50 mg) When taking modern iron supplements, it is absorbed 20 times better. Diet therapy should be one of the components of IDA therapy in children.
On the other hand, it is very important to focus not on the iron content in food, but on its form. It is the form of iron that determines the percentage of its absorption and assimilation and, consequently, the effectiveness of therapy. Of the various forms of iron, the easiest to absorb is heme iron, a complex organic compound in which iron is found in hemoglobin; inorganic compounds - iron salts - are absorbed by the body much worse. Iron in heme is actively captured by the cells of the intestinal mucosa and absorbed unchanged. The processes of heme absorption in the intestine do not depend on the acidity of the environment and the activity of food enzymes. Iron from cereals, vegetables, and fruits is absorbed much less well due to the presence of ferroabsorption inhibitors in them, such as oxalates, phosphates, tannin and others. Compare: the absorption coefficient of iron from beef (heme iron) is 17-22%, from fruit - no more than 3%. The degree of absorption of iron from animal products also depends on the form of iron-containing compounds. Thus, from the liver, where iron compounds are presented in the form of ferritin and transferrin, iron is absorbed in significantly smaller quantities than from meat products, although the total iron content in the liver is 3 times higher than in meat. Therefore, including liver in the diet to eliminate iron deficiency or for preventive purposes does not make any sense. Thus, the diet should be as rich as possible in foods that contain iron in the form of heme (beef tongue, rabbit meat, beef).
It should also be noted that meat, liver and fish improve the absorption of iron from fruits and vegetables when consumed simultaneously.
The absorption of iron from cereals, legumes, tubers, vegetables, and fruits is much lower, since they contain iron in non-heme form, and largely depends on the content in the diet of substances that inhibit or potentiate the absorption of iron. Ascorbic acid, meat, poultry, fish products, as well as substances that reduce the acidity of food (for example, lactic acid) enhance the absorption of non-heme iron. Soy protein and polyphenols found in tea, coffee, nuts and legumes reduce the absorption of non-heme iron. Despite the high iron content in some products of plant origin, they cannot meet the high iron requirement characteristic of a growing organism, since iron from them is absorbed much less well than from animal products. Recommendations to consume large quantities of fruit juices, apples, pomegranates, buckwheat and other products in order to replenish iron depots in IDA also cannot be considered justified. A diet balanced in terms of the main ingredients allows you to “cover” only the physiological need of the child’s body for iron, but does not eliminate iron deficiency in any way and should be used in combination with iron supplements in the treatment of IDA. However, a complete and balanced diet plays an important role in preventing the development of iron deficiency in a child’s body during all periods of childhood.
Drug therapy for IDA
The main goal of IDA therapy is to eliminate iron deficiency in the child’s body. This is achieved by taking iron-containing medications. The main requirements for iron preparations are a sufficient content of elemental iron and the absence of side effects and complications. Currently, there is a sufficient selection of iron preparations on the Russian pharmaceutical market, which expands the physician’s capabilities and allows taking into account the individual characteristics of patients when prescribing treatment (Table 1). In particular, convenient forms for young children have appeared - drops and syrup (ferrum lek, maltofer, actiferrin, hemofer).
All drugs are registered and approved for use in the Russian Federation.
Modern iron supplements are divided into two groups:
- ionic iron-containing preparations (salts, polysaccharide iron compounds);
- non-ionic compounds, i.e. preparations represented by the hydroxide-polymaltose complex of ferric iron (ferrum lek, maltofer).
The absorption of iron from a medicinal product depends on the content of elemental (active) iron in it. The largest amount of elemental iron is contained in preparations in which iron is presented in the form of fumarate (ferretab, ferronate) or ferrous sulfate (actiferrin, ferro-foil, hemofer prolangatum, ferro-gradumet). Currently, a new generation of iron preparations has appeared, which include drugs represented by the hydroxide-polymaltose complex of ferric iron (maltofer, ferrum lek). The peculiarity of these drugs is that the entry of iron from the intestine into the blood occurs through active absorption, in contrast to iron salt compounds, the absorption of which occurs along a concentration gradient. This is important because it eliminates the possibility of an overdose of iron preparations containing ferric iron hydroxide-polymaltose complex.
Iron salt preparations in the intestinal lumen interact with food components and other medications, which complicates the absorption of iron. Therefore, this group of iron supplements is prescribed one hour before meals. However, against the background of pronounced free radical stress that occurs when iron interacts with the intestinal mucosa during its diffusion, the damaging effect of iron compounds on the intestinal mucosa increases, which is manifested by dyspeptic disorders, including necrosis of the mucosa. If iron salt preparations are poorly tolerated, they can be taken with food, which will reduce side effects, but iron absorption, in turn, will worsen. Iron salt preparations should not be taken with tea, milk or combined with certain medications (tetracyclines, chloramphenicol, calcium supplements, antacids, penicillamine), since this reduces the absorption of iron.
Nonionic iron preparations, as studies have shown, do not interact with food components and medications, which allows the use of these preparations without disturbing the diet of children (the preparations can be added to food, juices) and treatment regimens for concomitant pathologies (if there is a need for such treatment ).
The daily therapeutic dose of iron preparations should be sufficient to normalize hemoglobin levels and replenish iron reserves in the bone marrow, which for iron salt preparations is 3-6 mg/kg/day of elemental iron in two or three doses. Iron hydroxide-polymaltose complex (ferrum lek) is prescribed at a dose of 3-6 mg/kg/day in one or more (at the patient’s request) doses.
Adverse reactions when taking iron supplements
The most common side effects observed during treatment with ferrodrugs (Table 2): metallic taste in the mouth, darkening of tooth enamel, allergic skin rashes, dyspeptic disorders as a result of irritation to the mucous membrane of the digestive tract, especially the intestines (loose stools, nausea, vomiting ). Therefore, the initial doses of drugs should be 1/2-1/3 of the therapeutic dose, followed by increasing them to the full dose over several days in order to avoid the occurrence of severe side effects. If you are intolerant to the salt preparation, it can be replaced with an iron hydroxide-polymaltose complex, the use of which does not result in the above-described effects. Iron hydroxide-polymaltose complex can be used immediately in full dose. Non-ionic iron preparations do not cause the side effects listed above, and a feeling of stomach fullness is also rare.
Parenteral administration of iron supplements
Parenteral administration of iron supplements is carried out only under strict indications due to the development of pronounced local and systemic side effects. Indications are as follows: pathology of the digestive tract (impaired intestinal absorption syndrome, ulcerative colitis, chronic enterocolitis, gastrointestinal bleeding) and intolerance to iron-containing drugs when taken orally.
Contraindications to the prescription of iron supplements are anemia not caused by iron deficiency (hemolytic, aplastic), hemosiderosis, hemochromatosis.
Duration of treatment
The clinical and therapeutic effects of oral ferrotherapy develop gradually. After some time, clinical improvement appears: weakness decreases, dizziness disappears, the child becomes more active, appetite increases, and the skin and visible mucous membranes gradually turn pink. On the 8-10th day of therapy, a reticulocyte crisis is observed - up to 5%, which confirms the effectiveness of treatment. Later, an increase in hemoglobin levels is observed; most often, normalization of hemoglobin occurs in the 3-6th week from the start of therapy and depends on the severity of anemia. On average, Hb levels increase by 10 g/l in 10 days. However, normalization of hemoglobin levels is not a sign of elimination of iron deficiency. To completely replenish the iron depot in the body, the course of ferrotherapy should be at least 3 months.
Reasons for the ineffectiveness of ferrotherapy
The ineffectiveness of therapy while taking iron supplements, if they are well tolerated, may be due to the following factors:
- wrong diagnosis,
- ongoing blood loss
- intercurrent diseases (ARVI, exacerbation of chronic foci of infection).
IDA is a disease that, with proper treatment, can lead to complete recovery!