Chronic venous insufficiency (CVI) is a pathology that develops due to a violation of the outflow of blood from the veins of the extremities. Frequent symptoms are changes in skin color, cramps, swelling, pain. The most common is chronic venous insufficiency of the lower extremities. Often, patients ignore the first symptoms of CVI and turn to a phlebologist with deteriorated health and the condition of the lower extremities. At the earliest stages, the disease is treated conservatively; when pronounced signs of impaired venous circulation appear, complex therapy is required, usually including treatment of varicose veins, nutritional correction, physical activity and wearing compression garments (1, English).
From the article you will learn the causes of chronic venous insufficiency and features of the development of the disease. Classic symptoms and method of diagnosis according to the international classification. Diagnostics and therapy are discussed in detail.
CVI – causes of chronic venous insufficiency
CVI is a symptom complex in which there are problems with the lumen of the veins. Usually the vessels have normal lumen. If there are disturbances, the capacity of the veins is significantly reduced. Overload of the venous system leads to impaired blood return, which is manifested by the appearance of symptoms of chronic venous insufficiency.
Impaired venous blood return leads to symptoms of CVI
Is CVI dangerous? Wikipedia states that CVI actively develops and progresses in women 30-50 years old, especially those with a hereditary predisposition. Often, symptoms of CVI appear during pregnancy, when body weight increases significantly.
Among the factors leading to CVI is weak physical activity.
The appearance of CVI is provoked by:
- travel in transport without changing position;
- long static position at the workplace;
- excess weight;
- tendency to constipation;
- staying in the heat for a long time;
- straining when lifting weights.
In addition, CVI can occur with systematic exercise and taking hormonal contraceptives; CVI often occurs during pregnancy.
Chronic LYMPHOVENOUS INSUFFICIENCY of the lower extremities and lymphoscintigraphy
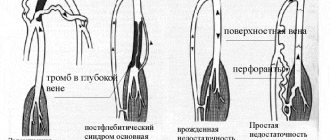
Edema of the lower extremities is observed in postthrombophlebitic syndrome in 80-100% of patients, depending on the form of the disease. According to the classification of V.S. Savelyev, there are edematous, edematous-varicose, varicose-trophic or trophic forms of the disease. When studying edema in patients with postthrombophlebitic syndrome, the main attention was paid to venous hypertension of the lower extremities. From this perspective, valvular insufficiency of the veins [3], diffusion of water and proteins in tissues at the microcirculatory level [1, 8], and venous hypertensive microangiopathy [14] were considered.
Disorders of lymphatic drainage in the lower extremities in thrombophlebitic syndrome have been studied to a lesser extent. The main work was performed using X-ray lymphography. It has been shown that on the lymphogram of a patient with this syndrome there is an expansion or, conversely, narrowing and tortuosity of the main lymphatic vessels, poor contrast or absence of the valve apparatus in the lymphatic vessels, their segmental obliteration, a pronounced network of pathological collaterals, multiple anastomoses between the lymphatic vessels, an expanded network lymphatic vessels of the skin, deposition of a contrast agent with the formation of lacunae, especially in the area of ulcers and blood clots, regurgitation of lymph through the lymphatic vessels, an increase or, conversely, a decrease in the size of the inguinal lymph nodes [2, 4, 9]. A slowdown in evacuation and a change in the nature of resorption of radionuclide drugs on the foot were also revealed.
This paper presents the results of further study of the main forms of edema in postthrombophlebitic syndrome. Along with changes in the veins, disorders of lymphatic drainage from the lower extremities were studied using radionuclide lymphoscintigraphy.
A total of 218 patients (190 women and 28 men) aged 21–75 years were examined.
Persistent lymphostasis of the lower extremities occurred in 50% of patients with postthrombophlebitic syndrome, usually with edematous and edematous-varicose forms of the disease. In the varicose-trophic form of the syndrome, pronounced lymphostasis of the legs and feet was extremely rare. Lymphostasis of the lower extremities was not observed in patients with the trophic form of the syndrome. All patients were operated on. All had a recanalized form of postthrombophlebitic syndrome.
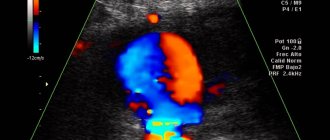
We studied the state of the lumen of the veins and the consistency of the valve apparatus of the superficial and deep veins of the lower extremities using ultrasound, using color Doppler mapping of blood flow and analysis of the Doppler frequency shift spectrum.
Lymphatic drainage from the lower extremities was studied using functional radionuclide lymphoscintigraphy. Most authors [15, 16] used this method to examine patients with lymphedema of the lower extremities. Lymphostasis in diseases of the veins of the lower extremities has not been studied enough.
The method of functional radionuclide lymphoscintigraphy is based on the ability of labeled colloidal particles, after their subcutaneous injection into tissues, to enter the lymphatic vessels and nodes that are regional to the injection zones of the radiopharmacological drug. For the study, the drug Lymphocys, labeled with 99m Tc (Sorin, France) was used in the amount of 185 MBq in a volume of 0.2-0.5 ml. The studies were carried out in a gamma chamber. With the patient lying on his back, the radiopharmacological drug was injected subcutaneously into the first interdigital spaces of the feet. Within 5 minutes after administration of the drug, the patient was in a state of muscle rest. At this time, the passage of the drug through the lymphatic system of the legs was observed. After 5 minutes, a three-minute load was performed (flexion-extension of the feet). After physical exercise, some patients noted a change in the nature of the advancement of the radiopharmacological drug at the level of the knee joints and hips. After the drug reached the level of the inguinal folds, the patient was asked to walk for 40 minutes, after which static photographs of the area of the legs, thighs, pelvis, and liver were taken.
The data obtained indicate that in edematous forms of postthrombophlebitis syndrome, edema in not all patients can be explained by regurgitation of blood through the main veins, as previously thought [4].
When analyzing the results of functional radionuclide scintigraphy, the following indicators were used.
1. Type of movement of the radiopharmacological drug on the scintigram. In this case, they distinguished: main movement through lymphatic collectors (in 25% of patients); diffuse movement of the drug through the interstitium of soft tissues (15%); mixed filling, in which the movement of the drug through the main lymphatic vessels and its diffuse evacuation were noted (60%).
Diffuse movement of a radiopharmaceutical on a functional radionuclide lymphoscintigram is a significant symptom for determining soft tissue edema. It can be used, in particular, for the diagnosis of hidden edema (latent stage of lymphostasis), when clinical data are in doubt.
2. Speed of movement of the radiopharmacological drug (visualization of the lymphatic tract of the legs along the entire length lasts on average 10 - 15 minutes).
3. The nature of contrast in functional radionuclide lymphoscintigraphy of the inguinal and iliac lymph nodes.
Enlargement of lymph nodes, reduction or absence of their image provided information about morphological changes in the lymphatic system both on the predominantly affected and relatively healthy limbs.
Studies have shown that the pathogenesis of edema with severe lymphostasis in patients with edematous forms of postthrombophlebitis syndrome cannot be fully explained by blood reflux through the main veins of the lower extremities. Thus, in 70 out of 81 patients with an edematous form of the disease with unilateral lesions, deep vein valve insufficiency was expressed to the same extent on both the diseased and relatively healthy limbs. In the edematous-varicose form of the syndrome, the insufficiency of the deep vein valves was the same on the sick and healthy limbs in 38 out of 77 patients, and in the varicose-trophic form in 40 out of 60. Consequently, in the edematous forms of postthrombophlebitic syndrome, blood reflux through the main veins is far from normal. In all cases, it plays a leading role in persistent lymphedema. This was confirmed in other studies [11]. Using retrograde popliteal venography among patients suffering from ordinary varicose veins, the authors identified reflux in the popliteal vein system in 71.1%, of which it was pronounced in 12%, and lymphostasis was absent in these patients. A similar pattern is also observed in many patients with the varicose-trophic form of postthrombophlebitis syndrome, in whom, despite gross anatomical changes in the valve apparatus of the main veins, there is no pronounced lymphostasis of the lower extremities.
The main significance in the pathogenesis of lymphostasis belongs to the disturbance of lymphatic drainage, which in postthrombophlebitic syndrome complicates diseases of the peripheral veins [10].
Of the 218 patients, only 44 retained the purely magistral type of movement of the radiopharmacological drug, which is natural for humans, and in all cases, contrasting of the lymphatic vessels and regional lymph nodes was enhanced due to chronic dynamic stagnation of the lymph. In 121 patients, along with the movement of the drug through the main lymphatic pathways, its diffuse movement through the interstitium was noted. It is assumed that diffuse filling occurs due to the spread of the radiopharmaceutical drug through an extended network of minute lymphatic vessels. It is also possible that the radiopharmacological drug may directly diffuse through the interstitium from the drug depot on the foot during edema (the effect of an ink stain spreading over blotting paper).
Along with the nature of the advancement of the radiopharmacological drug on the legs, the speed of its spread in the proximal direction was also important. It turned out that this parameter had a certain prognostic value. In 62 patients with accelerated movement of the drug (3-6 min) after surgery on the veins with lymphatic drainage intervention, a consistent good result was noted. There were no relapses of edema in these patients throughout the entire observation period (3-4 years). On the contrary, with a slow speed of drug movement (20 minutes or more), a good effect was observed in the immediate postoperative period and recurrence of edema in the long term.
In patients with an average speed of movement of the radiopharmacological drug along the lower leg (10-15 min), the immediate results after surgery were not as clear as in patients with accelerated movement of the drug. In 56% of patients, relapses of edema of varying intensity were noted. There was a preliminary opinion that the speed of movement of the drug is determined by the state of the pumping function of the lymphatic capillaries of the diseased limb.
The most important indicator of anatomical patency of the lymphatic drainage pathways was the image of the iliac lymph nodes. In all patients, contrast enhancement of the iliac lymph nodes, predominantly on the diseased limb, was reduced to varying degrees compared to the relatively healthy limb. In 50 patients, contrast enhancement of the iliac lymph nodes on the side of the diseased limb was absent, but on the side of the healthy limb it was satisfactory. Functional radionuclide lymphoscintigraphy of the inguinal lymph nodes turned out to be less indicative. Of the 218 patients, in 143, the incorporation of the radiopharmacological drug into the inguinal lymph nodes on the affected side was reduced compared to the healthy side. In 26 patients, the accumulation of the drug in the inguinal lymph nodes on the side of the diseased limb was more intense than on the healthy one. In 49 patients, the inguinal lymph nodes were contrasted symmetrically on the diseased and healthy sides.
Edema was classified clinically as resolving, partially resolving, or not resolving. With passing edema, the excess circumference at the level of the ankles compared to a relatively healthy limb did not exceed 1.5–2.5 cm. In this form, edema occurred by the end of the working day and disappeared overnight. The edematous fluid in such patients contained relatively little protein, according to our data, no more than 15-20 g/l, which corresponds to the normal protein content in the lymph of the lower extremities [12].
Transient swelling responded well to treatment with regular elastic compression (bandages, stockings, tights) and decreased after vein surgery, disappearing completely in most patients. Passing edema was observed mainly in the varicose-trophic form of postthrombophlebitis syndrome. Patients with transient, that is, predominantly phlebogenic, edema were not included in this study. Partially resolving swelling is characteristic of edematous and edematous-varicose forms of the disease. In the varicose-trophic form, edema of this type was rare. In such patients, the excess circumference of the lower leg in the distal parts reached 4-5 cm or more. Sufficiently long bed rest (up to three days or more) led to a partial reduction of edema: only the so-called “mobile” watery part of the edema resolved. At the same time, the perimeter of the lower leg in relatively mild cases decreased by 50-60%, in more severe cases only by 10-15%. The main, “persistent” part of the edema remained, despite the patients’ compliance with bed rest, compression therapy and external drainage. The protein content in the tissue fluid after resorption of the passing part of the edema was 32-35 g/l, which corresponds to literature data [12, 13].
The results obtained confirmed that in postthrombophlebitic syndrome, partially resolving edema is formed not only due to venous hypertension, but also as a result of difficulty in lymphatic drainage caused by impaired patency of the main lymphatic vessels and regional lymph nodes. Lymphostasis increasingly complicates venous insufficiency in postthrombophlebitic syndrome of the lower extremities. The more protein is contained in the tissue fluid, the more swelling increases due to water retention in the soft tissues. As edema increases, the pumping function of the lymphatic capillaries weakens, and at the same time the resorption capacity of the blood capillaries decreases [17]. The swelling gradually becomes persistent. Decompensation of the outflow of tissue fluid develops over a number of years, sometimes decades.
If not treated in a timely manner, swelling becomes permanent. Clinically, edema takes on the features of lymphedema (elephantiasis). In such patients, during operations on the extremities, hypertrophy of the subcutaneous fat layer was noted (its thickness is up to 6-7 cm). Excess fat was located circularly, mainly in the distal segments of the lower leg. Fat lobules pathologically increased to 3-3.5 cm in diameter.
In particularly severe cases, progressive fibrosis of the interstitial septa was observed in the ankle segment; in such patients, the adipose tissue acquired a finely lobed structure and crumbled when touched. In the absence of timely treatment, by the age of 50-60, patients experienced severe disabling complications: the appearance of the lower leg and foot was grossly disturbed, some patients developed percutaneous lymphorrhea, chronic dermatosis, outbreaks of erysipelas, and extensive deep trophic ulcers appeared on the lower leg.
During the surgical treatment of edematous forms of postthrombophlebitis syndrome, venous operations and lymphatic drainage interventions were simultaneously performed: the formation of lymphovenous anastomoses, fenestration of the fascia of the leg, external drainage and liposuction.
So, with postthrombophlebitic syndrome, there are three forms of edema of the lower extremities: passing, partially passing and not passing. Transient swelling occurs as a result of phlebostasis. They disappear after vein surgery and subsequent conservative therapy. The cause of partially resolving and persistent edema is venous insufficiency, complicated by increasing lymphostasis as a result of impaired patency of the main lymphatic tracts, inguinal and, especially, iliac lymph nodes, and inhibition of the pumping function of the lymphatic capillaries.
The data obtained using lymphoscintigraphy helps to clarify the diagnosis of lymphostasis, establish the level and extent of the block of the lymphatic system, the degree of disruption of its function, determine the indications for lymphatic drainage interventions during operations on the veins, choose the most appropriate method of lymph drainage and predict the results of surgical treatment.
Literature 1. Vasyutkov V. Ya., Chikalin V. I. Triggering mechanisms in the genesis of varicose and postthrombophlebitic ulcers of the leg // Bulletin of surgery. 1978. No. 2. P. 73 – 78. 2. Vakhidov V.V., Kadyrov R.Yu. Changes in superficial lymphatic vessels with lesions of the veins of the lower extremities // Surgery. 1977. No. 12. P. 41 – 45. 3. Vedensky A. N. Postthrombotic disease. L.: Medicine. 1986. 4. Zhukov B.N., Borisov V.K. On disorders and correction of lymphatic drainage in chronic venous insufficiency of the lower extremities // Bulletin of surgery. 1976. No. 2. P. 89 – 92. 5. Zhukov B.N., Myshentsev P.N., Musienko S.N. et al. Indirect functional dynamic lymphography of the lower extremities in phlebological practice // Bulletin of surgery. 1983. No. 8. P. 45 – 47. 6. Zolotorevsky V. Ya., Aliev M. M., Zelentsova M. V. et al. // Angiology and vascular surgery. 1996. No. 2. P. 44 – 51. 7. Konstantinova G.D., Buyanova N.N., Kostenko I.G. et al. Mechanisms of microcirculatory changes in varicose veins of the lower extremities // Surgery. 1977. No. 5. P. 56 – 61. 8. Kuzin M.I., Anichkov M.I., Zolotorevsky V.Ya. et al. Pathogenesis and treatment of non-healing ulcers in diseases of the vessels of the extremities // Surgery. 1979. No. 3. P. 24 – 31. 9. Pokrovsky A.V., Klioner L.I., Tarapon Yu.G., et al. Pathogenesis and surgical treatment of postthrombophlebitic and varicose ulcers of the legs // Surgery. 1974. No. 11. P. 73 – 77. 10. Savelyev V.S., Yablokov V.G. Postthrombotic disease. In the book: Diseases of the heart and blood vessels // Ed. E. I. Chazova. M.: Medicine. 1992. T. 3. P. 417 – 442. 11. Sukovatykh B. S., Nazarenko P. M., Belikov L. N. Mechanisms of formation of vertical blood reflux through deep veins in varicose veins // Vestn. surgery. 1992. No. 11-12. P. 330 – 335. 12. Yarema I.V., Urtaev B.M. Transfusion of lymph and its components. M., 1995. 13. Bates DO, Levick JR, Mortimer PS Cyange in macromolecular composition of instrstitial fluid from swollen arms after breast cancer treatmtnt fnd its implication // Clin. Sci. Cjlch. 1993, Dec. 85(6). P. 737 – 746. 14. Belgaro G., Christopoulos D., Nicolaides AN Skin flow and swelling in post-pyltitis limbs // Vasa. 1989. 18 (2). P. 136 – 139. 15. Mandell GA, Alexander MA, Harcke YT. Amultiscintigrahyic approach to imagining lymphedema and other causes of the congenially large extremity // Clin. Nucr. Vtd. 1993, Aug. 18(8). P. 646 – 654. 16. Ter SE, Alavi A., Rim CK, Merli G. Lymphosscintigrahye. A reliable test for the diagnosis of lymphedema // Clin. Nuck. Med. 1993, Aug. 18 (8). P. 646 – 654. 17. Zaugg VB, Dorffer MJ, Spiecel M. et al. Lymphatic capi llary pressure in patients with primary lymphedema // Microvaasc. Res. 1993, Sep. 46(2). P. 128 – 134.
CVI - symptoms
CVI may not manifest itself for a long time, but the symptoms that appear significantly affect the patient’s quality of life. The first symptoms are a feeling of heaviness in the legs, very often swelling of the legs and feet appears. Next comes bursting pain. The calf muscles may cramp at night, and the patient experiences a feeling of heat in the lower extremities.
Advanced forms of venous insufficiency - trophic eczema and ulcers
Spider veins and veins begin to appear through the skin, which with varicose veins become noticeable in the form of plexuses, similar to a bunch of grapes. The skin becomes drier and becomes covered with brown “islands” that grow as the disease progresses. Eventually, a trophic ulcer forms in their center.
The mechanism of the onset and development of the disease
Under the influence of gravity, the blood in the vessels descends to the lower extremities, the body has to make efforts to lift it. Venous valves prevent blood from flowing downwards, which are actively helped in this by physical activity, muscle contraction and bending of the knees. The combination of these factors ensures normal blood flow.
Maintaining a constant resistance to gravity is possible due to physiological changes in the lumen of blood vessels when changing body position, the operation of the valve apparatus and the tone (elasticity) of the venous wall. If one of these component mechanisms is disrupted, pathological processes begin to affect the entire system as a whole. Loss of elasticity of the section of the vein below the valve, and its expansion leads to valvular incompetence, the inability to maintain blood flow for subsequent rise. Stagnation of fluid leads to increased pressure to move blood upward. But, over time, increased pressure increases the volume of the part of the vein that has lost its elasticity.
Venous reflux (reverse flow of blood from top to bottom) can join the pathological process. The liquid begins to stagnate and put pressure on the walls of the vessel. As a result, blood plasma leaks into the surrounding tissue, causing swelling. The situation develops similarly with initial valvular insufficiency.
Simultaneously with circulatory failure, the lymphatic system is also overloaded. Trophic disorders contribute to the formation of trophic ulcers. Trophic ulcers are long-term non-healing wounds (6 months or more) affecting the skin and tissues. They form on the lower leg, are surrounded by an area of inflammation, and have a high risk of infection.
CVI - stages of chronic venous insufficiency
The disease has several stages:
- first the venous wall changes;
- valves stop functioning;
- perverted blood flow occurs, leading to venous hypertension;
- varicose veins appear;
- skin pigmentation changes;
- Varicose eczema may appear;
- at this stage, thrombosis often develops, affecting the deep veins;
- complications include thrombophlebitis, pulmonary embolism.
The walls of the veins become more permeable, lymph enters the blood, trophism is disrupted and inflammation occurs (10-15% of cases). The last stage of CVI is a venous trophic ulcer (4% of cases)
What happens to the vessels?
From the veins, blood flows towards the heart, that is, from bottom to top. Overcoming gravity is achieved, among other things, by venous valves - these valves close and prevent blood from flowing in the opposite direction. During physical activity or compression of the veins (during a massage, when wearing compression stockings), the muscles of the lower extremities contract, improving the outflow of fluid. The pathology is accompanied by a violation of the outflow of blood from the vessels of the legs. This occurs when physiological mechanisms are disrupted, in particular, pathology of the valve apparatus of the superficial or deep vessels of the leg veins and dysfunction of the vascular wall. As a result, the pressure in these veins increases, that is, venous hypertension develops (2, English). This, in turn, leads to symptoms characteristic of the disease.
On the left is normal operation of the valve apparatus, on the right is operation with disturbances. Against the background of the pathology, fatigue appears in the legs and pain in the evening. The disease can also develop in normal internal and superficial vessels of the lower extremities: the cause of the pathology is increased pressure in the inferior vena cava system, where blood flows from the vessels of the legs. Varicose veins are not equated to the concept of chronic venous insufficiency (3, English). When the deep venous network is affected, there are no visible nodular changes in the legs, but other manifestations of pathology are observed. The pathology is characterized by progressive venous hypertension, anatomical and pathophysiological dysfunction of the veins (valve and venous wall), pathological reflux of blood in the superficial and deep veins and secondary skin changes, both with and without the presence of varicose veins (4, English).
CVI - Diagnostics
Typically, patients turn to a phlebologist when obvious signs of CVI are visible to the naked eye, and the diagnosis is easy to make. Specialized clinics use ultrasound methods to diagnose CVI:
- the condition of blood vessels is studied;
- assesses how blood flows through them;
- Disturbances in the functioning of venous valves are considered.
Ultrasound scanning gives a complete picture of the causes of CVI
With an ultrasound examination, the doctor receives a three-dimensional image of the vessel, reliable information about its functioning, and can make an objective diagnosis.
People at risk
- Women are more susceptible to developing CVI than men - due to hormonal fluctuations, pregnancy, and childbirth.
- With varicose veins of the lower extremities, especially if there have been complications in the past.
- With diseases of the cardiovascular system - hypertension, atherosclerosis, heart rhythm disturbances.
- With metabolic disorders - diabetes, obesity, gout.
- Anyone whose ability to move freely or change body position is limited due to the nature of their profession, disability, diseases of muscles, joints, etc.
- Patients with a hereditary history of venous diseases.
CVI – complications of chronic venous insufficiency
Many patients have a common belief that CVI is not too dangerous, that it is just cosmetic. In fact, disturbances in the venous blood flow of the legs provoke the formation of blood clots. Therefore, CVI has two main complications: thrombosis and thrombophlebitis. In the first disease, the deep veins suffer:
- the affected area acquires a bluish tint,
- tissues swell
- movements are accompanied by pain.
With thrombophlebitis, blood clots form in the superficial veins. Wherein
- the skin turns red;
- Painful lumps form under the skin
- When walking, the patient experiences sharp pain in the legs.
A detached blood clot can clog a large vessel and cause death. Acute manifestations of these diseases are treated only in a surgical hospital. You can see the danger of CVI - photos, the results are on websites on the Internet.
Classification of the disease
Acute venous insufficiency has no classification by stages. Let's consider the degrees and stages of the chronic form of the disease. To fully describe the patient’s diagnosis, doctors use the CEAP classification, that is, assigning a kind of “code”, for example: C4a, S, Eс, Ad, Pr, 8, 10, 11, 17. It is deciphered based on the following classification characteristics.
C – pathology class:
- C0 – no visible symptoms;
- C1 – spider veins;
- C2 – dilated veins from 3 mm;
- C3 – swelling in the areas of the legs and ankles;
- C4a – dermatitis, pigmentation and other skin lesions;
- C4b – increased pigmentation, thickening of the skin;
- C5 – self-healing skin wounds;
- C6 – non-healing trophic ulcers.
The following index indicates whether the patient has complaints: A – without symptoms or complaints, S – there are complaints.
E – cause of disease:
- EC – congenital;
- Er – etiology unknown;
- Es – the reason is known.
A – localization:
- As – saphenous veins;
- Ar - vessels that connect the deep veins and subcutaneous veins;
- Ad – deep veins;
- Аn – there are no pathologies of the venous system.
P – type of pathology:
- Po – cessation of blood movement through the veins;
- Pr – valve insufficiency;
- Pr,o – both;
- Рn – no disturbances in the movement of blood through the veins were detected.
The number is the area of the venous system where the pathology is detected: from 1 to 18.
CVI. How to treat the disease with creams?
Treatment with all kinds of ointments is very common at the household level. Many patients stop treatment at this point. Most ointments only temporarily relieve swelling and pain. CVI – how to treat it? This question is asked by all patients. Such popular remedies as heparin ointment, venoruton, venitan, hepatrombin cope well with the external manifestations of CVI at an early stage, but cannot eliminate its cause. For effective treatment that will give long-term results, a visit to a phlebologist or vascular surgeon is mandatory.
CVI - how to cure without consequences?
This can be done even in difficult cases; treatment of CVI in Moscow can be carried out at a high level. True, then surgery will be needed to restore blood flow in the veins. But in the early stages, conservative treatment of CVI without surgery is sufficient. In particular, elastic compression is used. For this purpose, special medical knitwear is used in the form of stockings, golf, tights (conservative treatment).
When treating CVI, it is very important not to waste time using various ointments that give a local and short-term effect, but to seek help from a qualified specialist.
Treatment
Features of treatment
Treatment of chronic venous insufficiency involves conservative therapy and minimally invasive interventions (7, English):
- Therapy is always individual and depends on the stage of venous insufficiency and concomitant diseases, taking into account anatomical and pathophysiological changes in the vessels.
- Compression underwear eliminates many symptoms of pathology and allows you to quickly get a positive result from treatment.
- Treatment tactics are determined only after ultrasound scanning of the vessels of the lower extremities.
- If the pathology has developed due to changes in the deep veins, then conservative therapy is carried out.
- For pathologies of superficial vessels, minimally invasive intervention is performed followed by wearing compression stockings.
Minimally invasive treatment
- Laser vein removal (EVLO). Closing the affected veins with a laser beam is a painless procedure and does not leave scars. Treatment of veins of any diameter. In recent years, EVLO has undergone significant changes and has become the main method for eliminating the pathology of superficial veins.
- Radiofrequency obliteration (RFO). According to the mechanism of action, the technique is similar to that described above, but the treatment process uses radiofrequency rather than laser waves. The procedure is also painless and does not require a recovery period.
- Sclerotherapy/Cryosclerotherapy. Gluing of superficial veins with sclerosant with further transformation into a fibrous cord and resorption. Suitable for veins of small diameters.
- Phlebectomy. Surgical removal of varicose veins. Used for severe insufficiency of the superficial veins and only as a last resort. More modern methods of treating the disease are now available - laser, sclerotherapy. Today, laser obliteration completely replaces surgical treatment.
Conservative treatment
Conservative therapy slows down the course of the disease and relieves symptoms at an early stage.(8, English)
- Phlebotropic drugs. Used to reduce chronic swelling. They are used in tablets, parenterally and topically on the affected limb. Therapy may include several drugs that potentiate each other's effects.
- Therapeutic gymnastics, massage, pressotherapy, myostimulation. They improve blood movement in the deep veins and reduce the clinical manifestations of chronic venous insufficiency.
Conservative treatment of venous insufficiency is carried out with regular follow-up examinations by a phlebologist.
Compression treatment
A conservative method of treating pathology is used in addition to surgical and minimally invasive manipulations in the postoperative period. Compression is effective for the treatment and prevention of chronic venous insufficiency and postphlebitic syndrome (9, German). Indicated for all patients; the compression class and type of compression hosiery are determined by a phlebologist during an in-person consultation. Typically, a distal pressure of 20-30 mm is required at the initial stage. Hg Art. and 30-40 mm. Hg Art. with moderate chronic insufficiency, small varicose veins. Compression hosiery is worn immediately after waking up before swelling appears. The effect of compression treatment of CVI:
- enhances capillary blood flow, prevents the formation of trophic disorders;
- reduces the permeability of the vascular membrane, reduces interstitial edema;
- reduces the severity of symptoms;
- reduces the symptoms of restless legs syndrome;
- reduces reflux.
Treatment for restless legs syndrome
The greatest effectiveness in the treatment of restless legs syndrome and chronic venous insufficiency is provided by sclerotherapy and laser technologies in combination with wearing compression garments and taking phlebotonics.
At the first consultation, the phlebologist conducts an examination, ultrasound, makes a diagnosis and creates a treatment plan. Treatment is carried out according to indications, and then all that remains is to follow the recommendations regarding proper nutrition, physical activity and the preventive use of compression. Author of the article: Letunovsky Evgeniy Anatolyevich
Last update: 09/28/2020.
CVI - treatment at home
Don't be afraid if you are diagnosed with CVI. Treatment with folk remedies will alleviate the situation. For example, venotonic drugs will help. They strengthen the walls of blood vessels, stimulate microcirculation, and quickly relieve the feeling of tired legs and swelling. Patients are also treated with blood thinning medications.
Do you need to relieve the pain of CVI? Treatment with traditional methods:
- Apple vinegar. Twice a day for 30 minutes. Apply gauze soaked in vinegar to your feet for 30 minutes. Keep your legs higher. Reviews about the product are contradictory, but the majority note a positive, weak effect.
- Bell pepper. Dilute a teaspoon of pepper powder in a glass of hot water and drink three times a day. The product stops leg pain and improves blood flow. But CVI does not go away that easily, treatment, the results are still not the same as when treated by a professional phlebologist.
Symptoms of the disease
Let's look at the general symptoms first. It should be remembered that in the initial stages of the disease they appear one at a time and are often “blurred”. The more the disease progresses, the more pronounced the symptoms, and they most often appear in groups. So:
- pain in the legs, feeling of heaviness, fullness;
- spider veins;
- swelling - first passing after rest, then permanent;
- night cramps in the legs;
- dryness, unhealthy shine of the skin, age spots or areas of discoloration;
- trophic ulcers at an advanced stage.
Consultation with a surgeon: when to contact, how is the appointment?
Symptoms of CVI by stage
| Stage | Description |
| 0 | The person is able to work, there are no symptoms, they do not appear after sports and other activities. |
| 1 | Slight pain, heaviness in the legs and swelling at the end of the day, which disappears in the morning, mild cramps. A person is not limited in physical activity and can work at the same pace. |
| 2 | Manifestations of venous insufficiency become pronounced. These are skin pigmentation, dermatological diseases, severe swelling, skin necrosis in some areas. It becomes difficult for a person to work physically or play sports. |
| 3 | Trophic ulcers appear and tissue metabolism is completely disrupted. A person loses his ability to work. |
Symptoms of AHF
Signs of the disease are more pronounced and appear much faster compared to CVI:
- Pain in the legs that increases with movement;
- just below the site of vein blockage there is large swelling;
- difficulties in any physical activity;
- pallor or bluishness of the skin;
- at the site of pathology, skin temperature decreases by 2-3℃;
- body temperature can rise to 40℃;
- increasing pain to unbearable;
- “referring” pain to the groin and pelvis area.
Important! To reduce the likelihood of a blood clot breaking off with subsequent thromboembolism, the patient needs to limit movement. Bed rest is recommended for up to 10 days; the affected leg should be higher than the body.
Prevention of chronic venous insufficiency
If you perform simple activities every day, the risk of developing CVI is reduced significantly. Even if CVI is discovered, treatment will not be so serious, especially in the early stages.
- You should lead a healthy lifestyle and play sports.
- Follow a diet.
- Wear comfortable shoes and use orthopedic insoles.
- Use elastic compression.
If the first signs of CVI still appear, you cannot postpone a visit to a phlebologist. He diagnoses the degree of CVI. Any delay in time is fraught with complications. Some of them are fatal. If the disease has nevertheless developed to a complex stage, you should not despair. Even complex cases can be cured using modern endovascular surgery, see the photo on our clinic’s website.
Treatment of venous insufficiency is available in the following branches:
Treatment of venous insufficiency in the Primorsky region
Address: St. Petersburg , Primorsky district, st. Repisheva, 13
Treatment of venous insufficiency in the Petrograd region
Address: St. Petersburg , Petrogradsky district, st. Lenina, 5
Treatment of venous insufficiency in Vsevolozhsk
Address: Vsevolozhsk , Oktyabrsky Prospekt, 96 A
Frequently asked questions from our patients on the Internet
My legs are constantly swollen, how can I restore blood circulation in my legs? Maria from Arkhangelsk asks:
Dear Maria! To restore blood circulation in the legs, you first need to find out the cause of the swelling. As a rule, from a modern point of view, you need to start with an ultrasound duplex scanning of veins and consultation with a phlebologist.
How to identify blood clots in the legs? Oksana from Vladimir is interested in:
Dear Oksana! If you have the slightest suspicion of thrombosis, you should urgently seek medical help. A good diagnosis begins and always includes vascular ultrasound. This technique allows you to accurately determine not only blood clots in the legs, but also the cause of their occurrence. However, the method has a pronounced operator dependence, and it is better to trust professionals in their field.
How to understand that there are blood clots in the veins? Maxim from Yekaterinburg is interested in:
Dear Maxim! Only a specialist can reliably understand that there are blood clots in the veins, or exclude this situation. Thrombosis can be suspected based on the following signs:
- Swelling of the limb.
- Pain and/or redness.
- Feeling of heaviness and fullness in the limb.
- Vein thrombosis has already been previously diagnosed, since blood clots in the veins often recur.
The best solution would be to consult a phlebologist with an ultrasound scan of the venous vessels. You can make an appointment at our center for a consultation at any time convenient for you by phone.
How to check veins for blood clots in the legs? Asks Valentina from Smolensk:
Dear Valentina! You can check the veins for the presence of blood clots in the legs using ultrasound duplex or triplex scanning of the veins of the lower extremities at an appointment with a phlebologist.
How to treat chronic venous insufficiency at home? Zinaida from Tambov asks:
Dear Zinaida! Chronic venous insufficiency should be treated at home only after a good consultation with a specialist who will diagnose and give recommendations. Otherwise, you have a good chance of getting complications from the disease. When you find yourself on websites that colorfully describe how and what to treat at home, remember that most often professional doctors have nothing to do with such recommendations.
How to deal with the symptoms of chronic venous insufficiency? Nellie from Ufa asks:
Dear Nelly! It is better to start fighting the symptoms of chronic venous insufficiency in the legs before these symptoms appear, that is, with prevention: regular physiological exercise, a balanced diet, the use of compression hosiery for excessive loads, air travel. If signs of CVI appear: swelling, heaviness, varicose veins, you should consult a good specialist. This is the only way you can count on success.
PS I do not advise you to treat the symptoms of CVI at home via the Internet.
How to relieve pain from chronic venous insufficiency at home quickly? Asks Alexandra from Tyumen:
Dear Alexandra! The appearance of pain with varicose veins is most often a symptom of a developed complication, varicothrombophlebitis or deep vein thrombosis. If pain occurs due to varicose veins, stopping it at home is an extremely dangerous undertaking. It is necessary to quickly seek medical help, possibly calling an ambulance. You can quickly relieve pain with any NSAID, for example, ketoprofen or meloxicam (Movalis). But this is purely a temporary measure.
Varicose veins have started, what should I do? Maria from Nizhny Novgorod asks:
Dear Maria! If you have developed varicose veins or there are pronounced signs of varicose veins, you need to contact a professional. The most competent diagnosis and subsequent treatment can be provided to you by specialized centers for the treatment of venous pathology. After the examination, the center specialist will explain to you in detail what and how to do.
What is a good prevention for varicose veins on the legs? Nadezhda from Orenburg is interested in:
Dear Nadezhda! Prevention of varicose veins on the legs includes the following aspects:
- The closest to physiological load on the lower extremities, the involvement of the calf muscles, reducing the time of static load.
- Complete, balanced nutrition.
- For long-term static conditions and air travel, wear compression hosiery of I-II compression class.
Establishing diagnosis
CVI is often equated with varicose veins, which is not correct. Varicose veins are one of the manifestations of pathology. Diagnosis is based on medical history, examination and additional diagnostic methods. The specialist’s task is to determine the presence of chronic venous insufficiency, diagnosis according to the CEAP classification, and formulate treatment tactics. An ultrasound of the veins is mandatory - only an ultrasound examination allows one to study the condition of the venous apparatus and make an accurate diagnosis. The main ultrasound diagnostic methods include Dopplerography and angioscanning.
Doppler ultrasound
Used to study blood flow and diagnose reflux. Informative for the study of superficial veins with the presence of telangiectasia and reticular varicose veins (class C1). In patients with suspected damage to the deep veins of the extremities, with trophic ulcers, the method is often uninformative.
Ultrasound angioscanning
Visualization of deep and superficial veins, assessment of blood flow. According to the results of ultrasound scanning, unaffected veins, vessels with signs of reflux of non-post-thrombotic origin, and vessels changed as a result of previous thrombosis are determined. The method gives a complete picture of the condition of the superficial and deep veins of the lower extremities, and well visualizes the changed vessels. During pregnancy, acute thrombosis, chronic arterial insufficiency, pathologies of the kidneys and liver and many other diseases, ultrasound angioscanning is an important tool for the differential diagnosis of CVI; it identifies pathologies with high accuracy, which allows you to prescribe the correct treatment.
X-ray contrast venography (venography)
Injection of a contrast agent into the vascular bed, followed by a series of x-rays. Currently, the technique is rarely performed, since ultrasound research methods have become much more informative and accessible.
![Rice. 1. Functioning of the glymphatic system of the brain (according to [11]) 1. Glymphatic system functioning (according to [11])](https://expert35.ru/wp-content/uploads/ris-1-funkcionirovanie-glimfaticheskoj-sistemy-mozga-po-11-fig-1-330x140.jpg)