Detailed description of the study
Syphilis is an infectious disease caused by Treponema pallidum. Transmission of infection occurs primarily through sexual contact without the use of barrier contraception. However, it is possible to become infected with treponema pallidum through contact and household contact if personal hygiene rules are not observed, as well as transmission of the pathogen from mother to child during childbirth or breastfeeding. Syphilis can affect any organs and systems. In the absence of timely treatment, the disease becomes chronic. Initially, a hard chancre is formed at the site of contact with the source of infection - a painless ulcer with a small amount of transparent content on the surface. Often the body reacts to the introduction of the pathogen by inflammation of the lymph nodes located near the site of the lesion. Within a few weeks, a scar forms in place of the chancre. However, the disease does not recede, and after some time the infected person notices the appearance of a specific rash on the body - the appearance of small bright pink spots (rosacea rash). This stage is called secondary syphilis. The disease is prone to periodic exacerbations with changes in the nature of the rash. Tertiary syphilis is the result of untimely diagnosis and treatment of this disease. Along with the formation of nodes and tubercles on the skin, which are called gummas, prone to ulceration and scarring, damage to internal organs is observed. Diagnosis and treatment of syphilis is carried out by a dermatologist. To confirm the diagnosis, a modern test for determining rapid plasma reagins, or RPR test (Rapid Plasma Reagins), is used. These proteins are antibodies to the lipid components of cells destroyed by the pathogen.
What does it mean to donate blood for breast cancer?
This study is the first in the chain of necessary tests to diagnose syphilis. The principle of its operation is based on the recognition of antibodies to cardiolipin (an element located inside the membranes of bacteria). These antibodies begin to form at the initial stage of the disease (after several weeks of illness). To carry out the analysis, blood is taken from the patient or a lymph node is punctured. In 80% of cases, such a study makes it possible to identify the disease at an early stage.
A blood test for bladder cancer is prescribed strictly according to indications
Decoding the test for syphilis RPR
A positive test reaction usually appears 3-5 weeks after infection or a week after the appearance of the primary chancre on the body.
The test can also be positive within a year after syphilis has been cured and in some other diseases (antiphospholipid syndrome). When performing an analysis over time, the titer of RPR antibodies decreases. With complete cure of syphilis, the RPR analysis becomes negative in 98% of cases.
If the RPR test for syphilis is positive for the first time, the next step to confirm the infection is to test for total antibodies to Treponema pallidum.
A false positive test result can be found in pregnancy, tuberculosis, oncology, diabetes mellitus, gout, pneumonia and autoimmune diseases, as well as in the presence of other types of treponemas in the body, drug addiction, viral hepatitis, etc.
A negative test result cannot completely exclude late tertiary and early primary syphilis.
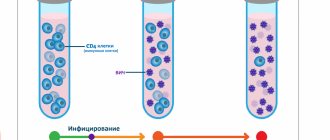
Dynamics of antibody formation in syphilis.
Despite the downward trend in the incidence of syphilis in the Russian Federation, the problem of the epidemiology of the disease remains relevant. There is a predominance of latent forms, cases of congenital syphilis are being recorded, and the number of cases of neurosyphilis is growing both in Russia as a whole and in individual regions, including Moscow [1].
A significant place in controlling the spread of syphilitic infection is occupied by diagnostics carried out by laboratory methods. It is especially important in latent forms of the disease, when it is necessary to make an early diagnosis, prevent the development of congenital syphilis, as well as late forms of infection.
In Russia, currently, absolute priority in the diagnosis of syphilis is occupied by serological research methods, among which non-treponemal (NTT) and treponemal (TT) tests are distinguished.
All modern NTTs are flocculation tests, in which the cardiolipin-lecithin-cholesterol complex, which is an antigen of non-treponemal origin, is used as an antigen.
NTT - microprecipitation reaction with plasma and inactivated serum (RMS), rapid plasma reagin test (RPR), venereal disease research laboratory (VDRL) test, etc. - used for screening
population for syphilis, monitoring the effectiveness of therapy (based on the antibody titer in paired sera obtained before and after treatment) and determining the activity of the infection (based on the height of the antibody titer).
In TT, an antigen of treponemal origin is used - pathogenic Treponema pallidum, both whole cell and in the form of recombinant proteins or synthetic peptides.
Modern TT - enzyme-linked immunosorbent assay (ELISA), passive hemagglutination reaction (RPHA) and its analogues, immunofluorescence reaction (RIF), immunoblotting (IB), immunochemiluminescence (ICL), simple rapid bedside tests (RBT), immobilization test of Treponema pallidum ( RIBT) - used to confirm
positive results of NTT and
screening
for syphilis (ELISA, RPGA, simple rapid tests).
Since serological diagnosis of syphilis is currently the most popular and includes a range of various research methods, their use raises a number of problems that often baffle dermatovenerologists. Among them, three main groups can be distinguished:
1. diagnostic errors made at various stages of the study
;
2. false positive (FPR) or biological false positive reactions (BLPR);
3. discrepancy between the results of individual studies.
Diagnostic errors made at various stages of the study are
As a rule, they are associated with violations committed at the preanalytical, analytical and postanalytical stages of the study.
It has now been established that up to 60-70% of diagnostic errors occur at the preanalytical
stage of the study, which is mainly the responsibility of
clinic workers
(doctors, nurses) [2-7].
Errors made at the preanalytical stage may be associated with improper preparation of the patient for the study or with testing of blood sera that are not suitable for the study.
It should be remembered that blood from a patient with suspected syphilis must be obtained on an empty stomach. On the eve of the study, the patient should not drink alcohol, medications or drugs. Blood is not taken from febrile patients, women during menstruation and in the first week after childbirth.
It is prohibited to use blood serum with signs of hemolysis, bacterial growth, as well as chylous (fatty, milky-white) serum for testing, as their testing may lead to false results.
At the analytical stage of the study, for which laboratory workers are responsible, errors can be caused by:
— low qualifications of laboratory staff and non-compliance with instructions for using reagent kits;
— lack of internal laboratory quality control of research and the practice of external quality control of research in the laboratory;
- improper storage of biological material (blood serum before testing for syphilis should be stored in a household refrigerator at a temperature of 4–8 ° C for no more than 74 hours; longer storage is possible at a temperature of –15 ° C and below; in this case, only a single dose
freezing/thawing frozen blood sera before testing);
- improper storage of reagent kits before testing - the expiration date and storage conditions are indicated on the reagent kits (in instructions or boxes for kits) (in a household refrigerator, at room temperature, frozen at a low temperature). Violation of these conditions leads to damage to the kits and loss of diagnostic activity.
Critical factors leading to errors at the post-analytical stage 3 of the study are:
— low level of training of clinic workers who do not know about modern tests for syphilis and do not know how to interpret them correctly;
— absence or low quality of a quality management system in an institution, when errors are possible due to incorrect labeling of test tubes, incorrect filling out of forms with research results, errors when entering research results into a laboratory journal, medical history or outpatient card, loss of research results.
Decision maker or BLPR
may be associated with low quality diagnostic tools (low sensitivity and specificity), but may also be due to other reasons.
One of the likely causes of false-positive tests for syphilis are technical errors accompanying the collection, delivery, storage of blood serum samples and the performance of serological tests for syphilis; violations related to the storage of reaction ingredients, failure to follow instructions when performing research and working on appropriate equipment.
BLPR registered in persons who do not suffer from syphilis using NTT are possible in case of HIV infection, hepatitis C, pregnancy, elderly patients, severe somatic pathology (including endocrine, oncopathology, diseases of the cardiovascular system, gastrointestinal tract). intestinal tract, lungs, with some dermatoses) [8-16].
ESLD can be divided into acute (registered within 6 months from the moment of detection) and chronic (more than 6 months). Acute ESBL are observed, as a rule, during acute infections of a viral and bacterial nature, after vaccination. Chronic ESLD can be observed in diseases of an autoimmune, endocrine nature, oncological processes, leprosy, chronic liver diseases, other (usually chronic) diseases, with injection drug use, and in old age.
LPRs are also found in endemic treponematoses and spirochetosis. However, these cases can hardly be classified as “false positive”. Treponematosis and spirochetosis are caused by bacteria belonging to the group of spirochetes, including Borrelia, Spirochaeta, Leptospira, Treponema pertenue
(yaws/yaws tropical),
T. carateum
(pint),
T. pallidum
subspecies
endemicum
(bejel).
Antibodies to pathogens in these diseases are close in composition to antibodies to T. pallidum
and are determined by the same methods [17].
To differentiate between false and true NTT seropositivity, TTs are used.
However, serological DPR for syphilis can also be observed during T.T. Thus, positive results of ELISA and RPGA were noted in patients with infectious mononucleosis, drug addicts, patients with collagenosis, in persons with malignant neoplasms, and in patients with endocrine pathology. In these cases, it can be difficult to distinguish true reactions from false ones, because syphilis can be combined with the above diseases. Positive results of TT can also be observed in elderly patients [18–21].
The following approaches can be used to differentiate between ESLD and early latent syphilis (ESS):
— carrying out a set of laboratory tests (NTT, several TT);
— obtaining comprehensive information about the patient and his sexual partners, including not only clinical and anamnestic, but also social and epidemiological data;
— conducting new, high-tech research.
For differential diagnosis between ESBL and RCC, differential diagnostic criteria can be used, including both serological and clinical and anamnestic indicators, as well as socio-epidemiological characteristics of patients [22].
Thus, for BLPR, registration of low titers of NTT (≤1:4), negative or weakly positive TT results, fluctuations in test values when repeated in the same laboratory, spontaneous (without antibiotic therapy) decrease in titers or negative seroreactions are more typical; from clinical and anamnestic indicators - the absence of anamnestic indications of rashes in the genital area within 2 years before treatment, the absence of enlarged inguinal lymph nodes, the absence of indications of syphilis and objective data indicating syphilis in a sexual partner; from social and epidemiological indicators - the age of patients over 40 years old, the presence of somatic pathology, late sexual debut (after 20-25 years), monogamous sexual relationships, the presence of a permanent job.
Patients with RSS are more characterized by high titers of NTT (≥1:8), sharply positive results of TT in the full complex, stable (positive) test values, decreased titers or negative seroreactions after specific therapy; from clinical and anamnestic indicators - anamnestic indications of rashes in the genital area within 2 years before treatment, the presence of enlarged inguinal lymph nodes (usually unilateral), data of confrontation - sexual contact with a patient with syphilis; from social and epidemiological indicators - the age of patients is under 20 years old, the absence of somatic pathology, early (up to 13-15 years and earlier) sexual debut, promiscuity, multiple sexual partners, lack of permanent work.
Inconsistency between individual studies
.
This problem has been of concern to dermatovenerologists for quite a long time, and is associated primarily with the complexity of serodiagnosis of syphilis. In particular, it worsened after a reversion algorithm for diagnosing syphilis, starting with the use of TT (as opposed to the traditional algorithm starting with NTT), began to be introduced into the practice of dermatovenerological institutions [23]. At the same time, a lot of unexplained cases appeared with discrepancies in the results of individual tests. This mainly concerned cases with positive TT results and negative NTT results, which were registered among categories of patients not belonging to the so-called “nuclear” groups (somatic patients, pregnant women, donors).
So what could be causing discrepancies in serological test results?
One of the reasons for the discrepancy in the results of serological reactions to syphilis may be differences in the timing of their positivity and negativity, associated with the peculiarities of the development of the immune response in syphilis
(drawing).
As is known, treponeme-specific antibodies related to Ig M
.
They appear as part of the development of the primary immune response, starting from the 2nd week after infection, can be recorded already during the incubation period, then their number increases, reaching a maximum at 6-9 weeks after infection, after which it gradually decreases [24-26 ]. Treponema-specific IgM
is recorded in reactions such as ELISAIgM, RIFIgM, 19SIgM-FTAabs, IgM immunoblotting.
Treponema-specific IgG
begin to appear in the blood of a patient with syphilis from about the 4th week after infection.
Their number reaches a maximum in secondary syphilis, as well as in RSS, and can remain at a high level throughout the rest of the life of the patient who has ever had syphilis, which serves as the basis for a retrospective diagnosis of syphilis. Treponema-specific IgG
is determined in reactions such as ELISAIgG, IgG immunoblotting, RPGA, RIT, RIF.
RIBT is one of the oldest, “classical” tests of syphilidology, still used in Russia, becomes positive approximately from the second half of the primary period of syphilis and can then remain positive for the rest of the life of a patient who has had syphilis, especially starting from the secondary stage [27 ].
Antibodies detected in NTT (antibodies against lipoid antigens of Treponema pallidum), as well as in RIBT, are detected in the blood from the second half of the primary period of syphilis; their concentration reaches a maximum during secondary and RSS, and then, as syphilis progresses to the later stages (tertiary, visceral, late neurosyphilis), they can be spontaneously eliminated, and NTT can become negative.
In this regard, it is not surprising that the results of individual serological tests at different stages of syphilitic infection may not coincide.
There is an effect (or period) of the so-called serological window, known for many infections [28, 29]. For syphilis, it includes the period of incubation and the onset of primary syphilis, when hard chancre in the form of erosion or ulcers has already appeared, and serological reactions that record the presence of reagin antibodies to lipoid antigens of Treponema pallidum are still negative. However, other treponemal “early” reactions may be positive, in particular, ELISAIgM, RIFIgM, 19SIgM-FTAabs, IgM immunoblotting, and also (in some patients) RIF.
The so-called phenomenon or prozone effect
when a patient with “blooming” syphilis (secondary, PSS) has a negative result of serological tests for syphilis (in particular, NTT) due to the competition of antibodies with different valences for antigen binding sites; in this case, blockade of antigenic determinants and a paradoxically negative reaction result can be observed [30-35]. The way out of this situation is to dilute the blood serum and retest it in dilutions (titers).
Negative results of serological tests (all or part) for syphilis may be due to immunosuppression
accompanying HIV infection, as well as other diseases/conditions associated with the development of immunosuppression (for example, patients receiving chemotherapy for cancer) [36]. The solution in this situation lies in a detailed study of the patient’s medical history, examination of them for HIV infection, staging more sensitive serological tests and the use of direct research methods.
Discrepancy between the results of serological tests may occur due to different analytical sensitivity of the tests
5 . To date, serological tests have been developed that have very high analytical sensitivity: for example, diagnostic kits for immunoblotting and RPGA, the sensitivity of which, according to the literature, is significantly higher than that of RIFabs., which is considered a generally recognized arbiter reaction [37].
Finally, discrepancies in the results of serological reactions can be observed due to the different nature and composition of the antigens included in them
and accordingly determined antibodies. So, for example, in NTT we determine antibodies to the cardiolipin antigen - antiphospholipid immunoglobulins, in ELISA - antibodies to protein antigens or lipoproteins. When performed simultaneously, the results of studies in different reactions may not coincide.
Options for combinations of non-treponemal and treponemal serological tests
In clinical practice, various combinations of NTT and TT results may occur, the interpretation of which is sometimes difficult.
So, classic combinations. When can this be observed?
NTT - negative, TT - positive.
This combination of test values can be observed:
- at the beginning of the primary period of syphilis - during the “serological window”, i.e. in the first 2-3 weeks after the appearance of chancre, when NTT have not yet been positive, and TT (especially IgM
- test options) are already positive;
- in the case of late untreated syphilis, if the NTT were spontaneously negatived (this happens in 20-40% of cases);
- with early syphilis, successfully treated (can be observed for the rest of the patient’s life, especially if he received treatment for secondary syphilis or RSS);
- with a false positive TT result; in this case, as a rule, a low level of TT seropositivity is observed; the study should be repeated in the same laboratory with the same test system.
NTT and TT are positive.
It would seem that this is a completely understandable situation, indicating that the patient has syphilis. However, other options are also possible. This situation can also be observed:
- after a patient with syphilis receives adequate treatment for early syphilis (within 1-1.5 years after the end of treatment for syphilis, as a rule, with delayed negativity of serological reactions), but it can persist for the rest of the patient’s life, especially if he received treatment for about secondary syphilis or RSS;
- in the case of treated late syphilis (serological reactions may remain positive forever);
- for treponematoses and spirochetosis (pinta, pagel, borreliosis, relapsing fever), if infections are caused by pathogens that are antigenically similar to T. pallidum
;
— in case of registration of false positive results of serological reactions (malignant neoplasms, autoimmune diseases, diseases of the gastrointestinal tract, severe chronic infections); in this case, as a rule, low titers of seroreactions are recorded, but they can also be high.
NTT - positive, TT - negative.
As a rule, this is a classic situation for false-positive NTT results for syphilis.
However, such a combination is possible in case of primary syphilis (when the IgG
variant of TT was used, for example, RPGA, RIBT, which had not yet been positive) and in the case of treated syphilis with a low concentration of antitreponemal antibodies.
NTT and TT are negative.
This situation can be observed:
- if the patient has never had syphilis;
- during the incubation period and at the beginning of the primary period of syphilis;
- for syphilis in a patient with severe immunosuppression (HIV infection, previous chemotherapy for a malignant neoplasm);
- in the case of a “prozone” effect in a patient with secondary, PCC (many antibodies competing for binding sites with the antigen);
— the patient received treatment for primary syphilis.
Clinical situations in the diagnosis of syphilis using ELISA and RMP methods
Practice shows that in the Russian Federation, ELISA technology in combination with NTT (RMP, RPR) is most often used to diagnose syphilis. This is due to the availability of a large selection of ELISA test systems offered by domestic and foreign manufacturers, the convenience of conducting ELISA tests “on-line” in large laboratories (centralized and laboratories of dermatovenerological dispensaries). At the same time, the use of various ELISA variants (with the determination of total antibodies ELISAat, as well as ELISA-IgM, ELISA-IgG) often leads to difficulties in interpreting the results obtained. Therefore, we will focus on the most common situations.
The initial period of syphilitic infection.
In the early stage of infection (incubation, the onset of primary syphilis), patients can have both positive (usually in low titer) and negative bladder cancer, a positive result of determining total antibodies (SAT) and
IgM
by ELISA.
The result of determining IgG
antibodies can be positive in a low titer (with a low positivity rate) or negative.
The results of serological testing may look like this: RMP ± , IFAsat +;
M+; G ± .
The initial period of syphilitic infection is characterized, as a rule, by the production of “early” treponeme-specific IgM
-antibodies and can be missed if the result of bladder cancer is negative and there is no due vigilance on the part of the dermatovenerologist. An important point to avoid mistakes may be to perform an ELISA test for clinical and epidemiological indications (indication of sexual contact with a patient with an infectious form of syphilis, the presence of a primary affect), as well as repeating the study after 5-7 days with a new portion of blood. Reproduction of the results obtained or positivity of breast cancer and IgG-ELISA will in this case be additional confirmation in favor of syphilis.
The period of “height” of infection
.
This refers to secondary syphilis, when antibodies detected in TT and NTT are recorded in the blood of a patient with syphilis.
As a rule, this period does not raise any doubts; it is accompanied by clinical manifestations and the following serological picture: bladder cancer +;
IFAsat +; M+; G+. If the sensitivity of ELISA-IgM test systems is not high enough, the following results of serological tests can be observed: RMP+; IFAsat +; M–; G+.
In rare cases, with an excess of antibodies, a “prozone phenomenon” can be observed - a paradoxically negative result, usually NTT. In this case, the following serological testing option can be obtained: RMP–;
IFAsat +; M+;
G+. In such a situation, RMP should be given in dilutions of blood serum with titer determination.
Differential diagnosis of RSS and BLPR.
The most difficult for diagnosis, especially in the absence of manifest manifestations of infection, low titers of bladder cancer, low positivity rate of IFAsat, negative IgM-ELISA, as well as the impossibility of testing for IgG-AT levels and a “negative” (in terms of syphilis) patient history is the following combination of results :
RMP+;
IFAsat+; M–; G+. In this case, differential diagnosis should be carried out between RCC and BLPR. A high titer of treponeme-specific IgG (≥1:1600) will be diagnostic for RSS [22]. Clinical and anamnestic data can provide significant assistance in establishing a diagnosis.
Late syphilis. Retrospective diagnosis.
In the late period of infection, bladder cancer can be negative, weakly positive, or positive in a low titer;
ELISA, on the contrary, is usually positive. At the same time, we have the right to expect positive results when determining total antibodies by ELISA, as well as IgG
in a high titer or with a high positivity rate.
The level of IgM
antibodies as the infection progresses to a late stage, as a rule, falls, and therefore the following combination is expected:
bladder cancer;
IFAsat+; M–; G+, high titer (high positivity rate).
A similar combination of study results may be observed in the case of treated syphilis,
if necessary, confirm the retrospective diagnosis.
However, due to the treatment, IgG
(and positivity rate) may be average or low, or the reaction to
IgG
antibodies may be negative.
The expected result will look like this: RMP–;
IFAsat±; M–; G± (medium, low titer or positivity rate).
Early congenital syphilis. LPR of newborns.
The classic combination of seroreaction results for early congenital syphilis will be as follows:
RMP+; IFAsat+; M+; G+
(M and G - high titer or positivity rate)
Due to the lack of sensitivity of test systems that detect IgM
-antibodies, the result of their determination may be negative, which does not exclude early congenital syphilis in a child.
of IgG
antibodies over time and comparing the results of examination of the child with the results of the mother can help in establishing the diagnosis
High titers of RMP and IgG—
ELISA without a tendency to decrease over the next 6 months after birth, exceeding the same indicators of the mother, testifies in favor of early congenital syphilis.
The combination of results may look like this: RMP+;
IFAsat+; M–; G+ (high titer or positivity rate without a tendency to decrease within 6 months after birth, antibody titers in the child are higher than in the mother).
Low titers or weakly positive results of breast cancer along with negative IgM-ELISA data, low titres or low positivity rate of IgG—
ELISA, accompanied by spontaneous negativity within 6 months after birth and lower values than in the mother, indicate false positive seroreactions in the child. The combination of results will look like this: RMP+(weak+; low titers); IFAsat+; M–; G+ (low titers, low positivity rate; spontaneous negativity of bladder cancer within 6 months after birth; AT titers in the child are lower than in the mother).
Relapse, reinfection.
The occurrence of a clinical-serological or only serological relapse after a treated infection is accompanied by a return of previous symptoms, which include primarily positive seroconversion.
The combination of seroreaction results is as follows: RMP+;
IFAsat+; M–; G+ - relapse. In case of reinfection, the picture will most likely be as follows: RMP+; IFAsat+; M+; G+ - reinfection.
Relapse and reinfection can be differentiated based on clinical, anamnestic and serological criteria (table).
Clinical, anamnestic and serological criteria for the differential diagnosis of relapse and reinfection
Clinical and serological control after treatment of syphilis
.
The main criterion for the quality of syphilis therapy at present is the intensity of the reduction in bladder cancer titers during the first year of observation [23]. The effectiveness of therapy is evidenced by a 4-fold decrease in bladder cancer titers in comparison with the initial (before treatment) data. ELISA results are not taken into account.
The following combinations may indicate satisfactory treatment results:
— RMP–; IFAsat–;
— RMP–; IFAsat+; M–; G-;
— RMP–; IFAsat+; M–; G+
Combination: RMP+; IFAsat+; M–; G+
in a treated patient with a gradual decrease in RMP titers (within 1.5-2 years after treatment) speaks in favor of a delayed negativity of seroreactions and the advisability of monitoring the patient without active intervention in his fate (i.e., without additional treatment with antibiotics).
A similar combination in a treated patient with an unchanged titer of bladder cancer, the absence of IgM-Ab and the presence of IgG-Ab may indicate the trace nature of the process (immunological memory, idiotype-anti-idiotypic interactions) and does not require the addition of antibiotics [39].
Combination RMP+; IFAsat+; M+; G+
in a treated patient with an unchanged titer of bladder cancer, the presence of detectable IgM and IgG-AT may indicate the persistence of pathogenic Treponema pallidum in the patient’s body and requires the addition of antibiotics.
Thus, the data presented indicate that problems exist in the serological diagnosis of syphilis. This is due to the variety of tests used, differences in their sensitivity and specificity, complexity of diagnosis and other reasons. At the same time, these problems cannot be considered insoluble. The key to successfully solving the problems of syphilis serodiagnosis is knowledge of the patterns of the immunological response to this infection, as well as knowledge of the characteristics of various tests, tactics of their use, correct interpretation and, undoubtedly, the presence of clinical thinking among dermatovenereologists and clinical laboratory diagnostic doctors.
The preanalytical stage includes the doctor’s collection of the patient’s medical history, assessment of clinical symptoms, as well as preparation of the patient for examination, collection, storage and delivery of biological material.
The analytical stage involves conducting research in the laboratory.
The post-analytical stage involves recording research results in laboratory journals or electronically, clinical interpretation of the results and establishing a diagnosis using the results obtained.
Core groups are groups of patients with a high risk of contracting STIs in general and syphilis in particular. The core groups currently include commercial sex workers, men who have sex with men, alcohol abusers, intravenous drug users, and adolescents with deviant behavior.
Analytical sensitivity is the ability of a method to detect the minimum amount of the substance of interest or the smallest differences between two concentrations of the substance being tested.
Preparation for delivery
When preparing to take the test for bladder cancer, you need to follow several recommendations:
- Blood must be donated on an empty stomach. You are allowed to drink plain water before the collection.
- It is recommended to eat your last meal 8 hours before donating blood.
- On the eve of the analysis for bladder cancer, it is recommended to remove fatty, spicy or fried foods, as well as alcoholic beverages from the daily diet.
- Before the analysis, try to avoid heavy physical activity.
- Be sure to notify your doctor about taking medications, the presence of diseases or pathologies, or feeling unwell.
To test for bladder cancer, blood is taken from a vein.
Total antibodies to Treponema pallidum: explanation
A positive reaction to antibodies to Treponema pallidum indicates different clinical stages of syphilis (primary, secondary, latent). Also, a positive test result for total antibodies to Treponema pallidum may persist for some time after a course of treatment for syphilis (“serological scar”).
The test result is negative in the absence of infection or early primary syphilis.
The test for total antibodies to Treponema pallidum may have an equivocal result. Then a repeat analysis for total antibodies is carried out a couple of weeks later.
When is a test ordered?
The main indications for blood sampling for RMP are:
- examination before surgery or admission to hospital;
- mandatory examinations for syphilis of pregnant women, donors and people of certain professions;
- the appearance of the first signs of the disease (enlarged lymph nodes in the groin area, rash on the skin);
- completion of drug treatment of the disease.
Also, a study of breast cancer is mandatory for a child born from an infected mother.
Important! Don’t be afraid to donate blood for bladder cancer; it is best to diagnose the disease in the early stages than to deal with complications later.