According to statistics, cardiovascular diseases occupy a leading position in the world in terms of prevalence. Among them, myocardial infarction is considered the most dangerous. It causes very significant damage to humanity. More than half of patients who survive this disease become disabled, and about 13% do not survive even with intensive care. The cause of high mortality and severe consequences is often untimely and unqualified diagnosis. The troponin test for myocardial infarction allows one to fairly accurately determine the presence of pathology and begin to eliminate it. Its use is also effective in monitoring the course of the disease.
Methods for detecting myocardial infarction
Timely diagnosis of myocardial infarction allows you to quickly take appropriate measures and not only facilitates the course of the disease, but also often becomes the key to saving the patient. Today, pathology is diagnosed using:
- physical examination. The method is based on observation of external signs and symptoms of the disease. Pulse and blood pressure are also measured;
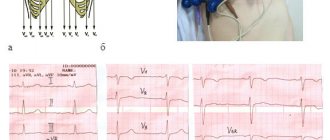
- electrocardiography. The data displayed on the electrocardiogram allows the doctor to accurately determine cardiac dysfunction;
- echocardiography (ultrasound of the heart). The patient is examined using an ultrasound sensor. The method is most effective in detecting acute myocardial infarction;
- radiography. The studies are carried out in a clinical setting using an X-ray unit. Diagnostics gives a general picture of the condition of the patient’s organs and in particular the heart. The method is effective in preventing complications that often accompany myocardial infarction;
- laboratory research. They are based on the study of blood tests of the patient, which during myocardial infarction significantly changes its composition and structure. In addition to changes in the content of constant components in the blood, with necrosis of the heart muscle, special proteins - markers - are released into the circulatory system.
Differences between quantitative and qualitative methods for diagnosing myocardial infarction
A quantitative method for diagnosing myocardial infarction is a laboratory blood test, the result of which is a specific number. This type of troponin determination is quite lengthy and requires the use of sophisticated laboratory equipment. An increase in this protein in the blood (in acute myocardial infarction) compared to the preliminary result means that the disease is characterized by an unstable course, and therefore more aggressive treatment is necessary.
A qualitative method is an express diagnosis of myocardial infarction, which uses a special test strip. This study takes from 20 minutes to 1 hour.
The role of troponins in the body
Troponins are unique markers of cardiac activity that make it possible to detect pathologies even after some time. The location of these proteins is the heart muscle. They are responsible for the contraction and relaxation of the myocardium. A disturbance in an organ, namely a heart attack, causes tissue destruction and promotes the penetration of troponins into the circulatory system, which subsequently makes it possible to judge the presence of this pathology.
Troponins act as a kind of lubricant for striated muscles.
By type, troponins are divided into I, T and C. Each of these three proteins is equally responsible for the normal functioning of the myocardium. However, having different molecular weights, they perform their specific functions. The troponin complex provides relative gliding of striated muscles. The content of protein T in the complex is twice that of the others. In the diagnosis of myocardial infarction, special attention is paid to troponins T and I. They inform about pathological changes in the tissues of the heart muscle. The unequal lifetime of proteins makes it possible to conduct research at different stages of disease development.
The lifespan of troponin I reaches up to a week, after which it ceases to exist. For troponin T, this period extends to 10–18 days. This difference makes it possible to determine the exact date of a heart attack, regardless of the patient’s well-being at the time of crisis.
Troponin T, due to its specificity and sensitivity, makes it possible to determine the minimal zones of cardiac muscle death in patients suffering from coronary disorders. Such pathologies are classified as microinfarctions. If an increased concentration of troponins T and I is observed in patients in whom coronary syndrome is acute, then even minor deviations in the electrocardiogram (for example, a reduced ST segment, an inverted T wave) are guaranteed to indicate the presence of myocardial infarction.
It has not yet been precisely determined which of the troponins, T or I, provides more reliable information about myocardial infarction. Cardiac protein I seems to be a more effective marker of the myocardium, but in terms of standardization it is inferior to troponin T. The test based on the latter is patented by a specific manufacturer, supported by numerous studies and fixed results. The production of troponin I tests involves many companies using different methods and reagents, the effectiveness of which is difficult to verify.
Blood troponin levels
The presence of troponins in the blood does not necessarily indicate myocardial infarction. Thus, the blood of a completely healthy person can contain about 0.1 ng/ml of these proteins. It all depends on the characteristics of the body and its condition at the time of the test.
The appearance and increase in the level of troponin T in the blood can be a consequence of:
- consumption of alcoholic beverages;
- recent surgery;
- myocarditis;
- pericarditis;
- infective endocarditis;
- traumatic changes to the skeleton.
Also, a high concentration of this protein can be a consequence of sepsis (acute infection of the body as a result of pathogenic microbes entering the blood).
Rapid test for determining cardiac troponin
The troponin test is a qualitative test for determining elevated troponin concentrations in the blood after myocardial infarction. A rapid test for determining troponin is performed on a special plate with 2 stripes. One of the bands contains polyclonal antibodies to troponin (the band is designated by the letter “T”), and the other strip is a control (designated by the letter “C”). Until the test sample is applied to the test strip, both stripes remain invisible. After placing a drop of blood into a special well on the plate, a specific immunochromatographic reaction occurs. The control strip “C” should always be colored, and this indicates the correctness of the test and the suitability of the reagents. The “T” strip is colored only if the patient’s blood contains a significant amount of troponin, otherwise it remains colorless.
Such a rapid troponin test for myocardial infarction allows us to establish an increased concentration of troponin in the blood in just 20 minutes, which suggests myocardial infarction.
Reason for performing a troponin test
Reasons for performing a troponin test are symptoms consistent with myocardial infarction. The procedure is carried out on the condition that rapid laboratory tests are not possible. The rapid test provides instant information and saves precious time allocated to save the patient.
Testing for troponins is most necessary for atherosclerotic patients, overweight people and those suffering from angina pectoris. The reasons for the test are:
- Sudden pain inside the chest, on the left side, which radiates to the left shoulder, collarbone, ear, and is also noted in the neck and between the shoulder blades.
- Sharp fluctuations in blood pressure.
- Changes in heart rate.
- Choking, pallor of the patient, dizziness. sweating
- Weakness, nervous disorders.
When should you do a troponin test?
Myocardial infarction is an acute, life-threatening condition caused by a circulatory disorder in the myocardium as a result of complete or partial blockage of a coronary artery by a thrombus.
This leads to ischemia and necrosis of part of the heart muscle. Subsequently, the chances of a successful outcome depend on the timeliness of medical care. The myocardial infarction test is performed at the first symptoms of a heart attack:
- pain in the chest and heart area, aggravated at rest, of a compressive nature, with a feeling of squeezing or burning;
- pain in the arm, neck, jaw, on the back in the area of the shoulder blades or between them, discomfort in the abdomen;
- severe weakness and shortness of breath with a feeling of lack of air, fear of death;
- sticky cold sweat, chills, trembling in the arms and legs;
- nausea, vomiting, unstable blood pressure against the background of heart pain and a general progressive deterioration of the condition.
Also, the use of a rapid heart attack test is recommended for patients with angina pectoris, coronary artery disease with frequent attacks of chest pain.
Troponin analysis is used:
- at home, if it is impossible to see a doctor for heart pain;
- when severe pain occurs, in patients with chronic cardiac pathology;
- within 2-4 hours after the first symptoms of a heart attack appear;
- at the prehospital and hospital stage, to confirm the diagnosis.
Troponin test in action
Troponins during myocardial infarction make themselves felt almost immediately after the incident. Their influence is reflected in the breakdown of the protein complex into molecules and subsequent penetration into the blood. This phenomenon has been used in medicine for more than a decade and has successfully proven itself in modern diagnostic methods.
If, when a patient visits the cardiology department, he has symptoms of myocardial infarction, but the ECG readings do not give confidence in the latter, a quantitative troponin test is prescribed. This procedure involves accurately determining the amount of troponins in the patient's blood. The measurement is in nanograms per liter. The value of a quantitative test in monitoring the dynamics of changes in cardiac protein content. Thus, the method makes it possible to identify relapses of pathology and provide the patient with more intensive therapy. The disadvantage of a quantitative test is its complexity and the requirement of special equipment. In addition, its implementation takes quite a lot of time.
Standard Troponin Test Kit
Troponin rapid test does not require such high qualifications from a medical worker as other methods. Externally, the product resembles a household pregnancy test. It is represented by a strip with marked divisions. To get the result and draw a definite conclusion about the presence of heart pathology, one drop of blood placed in a special compartment is enough. The procedure takes 15 minutes. The appearance of one strip indicates the normal state of the body. Two stripes indicate that the troponin T level in the blood is exceeded and the patient needs emergency help.
If no stripes appear during the test, this means that the product has expired and the procedure must be repeated using a new test.
The value of the troponin test is in the accuracy and speed of determining myocardial infarction. Even with an atypical form of pathology, which complicates other types of diagnosis, this test will almost certainly indicate the presence of troponin in the blood.
Today, the troponin test can be found on pharmacy shelves. It is almost always included in the products found in ambulances. Relevant personnel are familiar with its use.
It should be remembered that the rapid test is not a 100% guarantee of the presence or absence of myocardial infarction. Even with a negative result, but symptoms of the disease appear, more serious laboratory tests or a repeat test, performed 3-4 hours after the first, are necessary, since the maximum concentration of troponins in the blood is observed only 6-8 hours after damage to the myocardial muscle.
Write to us
About the test
The CardioBSFA rapid test is a test system for the rapid bedside determination of elevated levels of the early cardiac marker cardiac fatty acid binding protein (cFABP) in venous whole blood.
The use of the CardioBSJK rapid test helps in the early diagnosis of acute myocardial infarction, especially in the first 12 hours from the onset of clinical manifestations
- with an atypical clinical picture;
- in the absence of clear electrocardiographic criteria (absence of ST segment elevation, against the background of bundle branch blocks and cicatricial changes in the myocardium).
Areas of application:
- Examination of the patient at home
- Reception of a patient at the clinic
- In the ambulance
- Hospital emergency room
- Laboratory
- Any medical department (BRIT, department of cardiology, therapy, surgery, etc.)
- First aid stations, first aid stations
Setting up the test and evaluating the results
Before starting to use the test, please read the instructions for use carefully.
- 100-150 μl of heparinized whole venous blood is added to the oval window of the tablet.
- The test result is assessed visually in a rectangular window of the tablet after 20-25 minutes as positive (two stripes) or negative (one strip):
Analytical characteristics of the “CardioBSJK” express test
*The sensitivity of the CardioBSJK tests is tested using recombinant cardiospecific BSZHK (human) produced by NPO BioTest LLC.
| Time from the onset of clinical manifestations | 1-3 hours | 3-6 hours | 6-12 hours | 12-18 hours |
| Sensitivity | 86% | 92,4% | 94,5% | 100% |
| Specificity | 87,5% (93,1%*) | |||
| Accuracy of the method | 91,7% (93,3%*) | |||
| Positive predictive value | 94,6% (97,2%*) | |||
| Negative predictive value | 87,4% | |||
Based on the results of a clinical study of 108 patients consecutively admitted to the hospital with suspected acute myocardial infarction. The diagnosis of myocardial infarction was confirmed or removed based on a summary analysis of troponin I indicators, CK-MB series, ECG dynamics, and echocardiography. The results obtained were correlated with the results of the CardioBSJK test. *Analytical characteristics when excluding patients with previously diagnosed stage III-IV chronic renal failure from the sample.
Functional and technical characteristics of the “CardioBSJK” express test
| Operating principle | Immunochromatography |
| Blood sample volume | 120-150 µl |
| Analysis result | Quality, yes-no |
| Evaluation of results | Visual, within 5-25 minutes |
| Hardware | Not required |
| Sensitivity | 15 ng/ml |
| Portability | Compact dimensions 94x20 mm |
| Storage conditions | 4 - 20(degrees) |
| Shelf life | 18 months |
| Package | ETC1-10 individual sealed packages with desiccant in a cardboard box. ETC2 - 10 individual sealed packages with a desiccant in a cardboard box, 10 individual Pasteur pipettes, 10 stickers for the medical history. |
Cardiac marker sBSFA
Cardiac fatty acid binding protein (cFABP) is a cardiac-specific cytoplasmic low molecular weight protein (15 kDa) that binds and transports fatty acids within the cell. A small amount of sBSFA constantly circulates in the blood of healthy people. The upper limit of normal is 6 ng/ml, with background levels fluctuating depending on age, gender and circadian rhythm. sBSFA is excreted from the body by the kidneys, therefore, in patients with renal failure (creatinine > 200 µM), there is a steady increase in the background level of sBSFA in the blood, against the background of a decrease in glomerular filtration.
sFAFA is an early cardiac biomarker. With the development of myocardial necrosis and destruction of the cell membrane, cytoplasmic sFAFA immediately enters the intercellular space. Due to its low molecular weight, it quickly diffuses through endothelial clefts into the vascular bed and enters the bloodstream. The dynamics of the release of sBSFA is single-phase and similar to the dynamics of myoglobin. A diagnostically significant increase in the level of sFAFA is observed 1-2 hours after the onset of pain. The level of sFAFA in the blood reaches its maximum values 6 hours after myocardial necrosis and returns to normal values after 12-18 hours for Q-negative and 24-72 hours for Q-positive acute myocardial infarction (AMI) (Graph No. 1.). The amount of sBSFA in the blood increases in proportion to the extent and depth of the infarction zone, and reaches a level of more than 200-300 ng/ml with a diagnostic level of myocardial necrosis of 15 ng/ml using the immunochromatographic method.
Schedule No. 1. Dynamics of cardiac biomarkers in myocardial necrosis
In the first hours of myocardial infarction, the early cardiac biomarker sFAFA is superior to troponins and MB-CK in sensitivity, and myoglobin in specificity. The “diagnostic window” with a late increase in the bloodstream (5-8 hours) and a late time of maximum increase (11-30 hours) makes the standard cardiac biomarkers CF-CK and troponins uninformative for the early diagnosis of AMI (Table No. 1).
Table No. 1. Dynamics of the level of cardiac biomarkers during myocardial infarction
| Cardiac biomarkers | Detection time from the onset of clinical manifestations, hour. | Time of maximum increase, hour. | Time to return to baseline |
| sBSJK | 1 | 6 | 24-72h |
| Myoglobin | 2 | 6 | 24-39 h |
| MV-KFK | 5 | 14 | 72-120 h |
| Troponin T | 7 | 19 | 7-14 days |
| Troponin I | 6 | 18 | 5-10 days |
Clinical studies conducted earlier by Ishii 1997, Glatz 1997, Okamoto 2000, Ghani 2000, Nakata 2003, O'Donoghue 2006 confirmed the higher diagnostic value of sBSFA in comparison with myoglobin in patients admitted to the hospital with chest pain syndrome and suspected AMI . In all studies, the area under the characteristic ROC curve of specificity and sensitivity for sFAFA is significantly greater than that for myoglobin, which is a result of the high cardiac specificity of sFAFA.
The high cardiac specificity of sBSFA is explained by its maximum concentration in cardiomyocytes (0.5-0.6 mg/g), which significantly exceeds its concentration in other tissues. In addition to myocardial tissue, sBSFA is found in skeletal muscles, the small intestine, some parts of the brain and, according to some data, in the proximal and distal tubules of the kidneys, adipose and other tissues (Table No. 2).
Table No. 2. The content of sFAFA in various tissues (Glatz JFC, Van der Vusse GJ. Cellular fatty acid-binding proteins. Their function and physiological significance. Prog Lipid Res 1996;35:243-82)
| Fabric type | sBSFA content, µg/g |
| Myocardium | 540-600 |
| Striated muscles | 20-170 |
| Brain | 16-39 |
| Small intestine | 2-5 |
An increase in the level of sFAFA , like any other cardiac marker, is a reflection of myocardial necrosis of both coronarogenic and non-coronarogenic origin. The main cause of elevated sFASH levels is acute myocardial infarction. In addition, the increase may be a consequence of the destruction of cardiomyocytes during inflammation, trauma, surgical interventions, intoxication, etc. The level of sFAFA increases with atrial fibrillation, after EIT, with stage III-IV chronic renal failure, acute strokes, and extensive muscle injuries.
Therefore, an assessment of the level of sFAFA should be carried out by a doctor, taking into account all anamnestic and clinical data. Determining the level of sFAFA in a patient with chest pain syndrome in combination with a competent analysis of the clinical case provides significant assistance in the early diagnosis of AMI, especially in the first 12 hours of the disease.
As a result of numerous studies of the diagnostic aspects of the use of this protein, in 2007 the Society of Clinical Laboratory Biochemical Medical Practice of the United States included sBCFA in the list of recommended biomarkers of myocardial necrosis, which is a prerequisite for the use in clinical practice of available diagnostic tests that determine this cardiac biomarker.
Recommendations for use
Before starting to use the test, please read the instructions for use carefully.
- Collect heparinized blood according to the standard method
- Open the individual packaging and place the test on a dry, flat surface.
- Add 120-150 µl of blood into the oval window (Fig. 1)
- Interpret the result after 5-25 minutes. (Fig.2)
| Fig.1 Adding a blood sample for testing | Fig.2 Interpretation of test results |
Interpretation of test results (Fig. 2)
Positive: If the test result is positive, two purple lines appear in the result reading window - test and control. The control line certifies that the plates are working correctly. The color intensity of the control and test lines may be different. The concentration of sFAFA in the blood is higher than the diagnostic level of myocardial necrosis.
Negative: Only one purple line appears - the control line. The concentration of sFAFA in the blood is below the diagnostic level of myocardial necrosis.
Indeterminate: If the control line does not appear, the test results are invalid. In this case, it is recommended to repeat the test using a new test tablet.
Attention! The presence of a test line of any intensity indicates a positive result.
Test evaluation examples
Possible errors when performing the test and ways to eliminate them
1. There are no bars in the rectangular results viewport
| Cause | Elimination methods |
| Insufficient volume of blood sample applied | Take a new test and add a blood sample of 120-150 µl |
| Violation of test storage conditions | Take a new test that has been stored in accordance with the storage conditions, open the individual test package immediately before adding the blood sample |
| Blood viscosity too high | Perform analysis using another method |
2. The appearance of a red background in the window for viewing results
| Cause | Elimination methods |
| Excessive volume of blood sample applied | Take a new test and add a blood sample of 120-150 µl |
| Entering a blood sample into the window to view the results | Take a new test and add a blood sample to the foramen ovale for sample depositing |
| Hemolytic blood | Take a new blood sample or test using another method |
Prevention is better than cure
Any highly effective tests and therapy in prestigious medical institutions are not comparable to full health. No matter how high the achievements of modern medicine, myocardial infarction continues to cripple human lives.
Maintaining a healthy lifestyle significantly reduces the risk of myocardial infarction
Preventive measures that are not difficult for anyone can significantly reduce the possibility of the manifestation of this pathology:
- Increased physical activity.
- Rejection of bad habits.
- Balanced diet.
- Optimism.
- Timely rest and healthy sleep.
- Consultations with a family doctor.
- Prevention of diabetes and hypertension.
Even if a person has never experienced heart failure before, at the slightest suspicion of a heart attack, you should immediately call an ambulance. Self-medication and loss of time are fraught with fatal consequences.