Treatment and prevention of neuroses
The cause of neuroses is psychological tension, which arises under the influence of stress and gives rise to internal conflict. In other words, a neurotic disorder is a distorted way of adapting the psyche to unbearable circumstances.
A neurotic disorder does not change personality and does not take away a person’s ability to think critically about their condition - this distinguishes neuroses from psychoses, when changes in the psyche are deeper and more persistent. Therefore, treatment of neuroses is usually successful and should result in complete recovery, provided that all the necessary conditions are met.
How do neuroses manifest themselves?
What comes to the fore in a state of neurosis: emotional instability, difficulties in adapting to rapidly changing circumstances, fear of the slightest changes, self-doubt, the desire to always focus on a certain standard, excessive sensitivity to the mood of others and anxiety when negative emotions of another, obsessive movements hands, frequent weakness and health complaints.
Neurotic disorders are characterized by a combination of anxiety and depression. Phobias, obsessions, panic attacks, headache attacks, hypochondriacal thoughts, disorders of a psychosomatic nature - manifest themselves depending on the type of neurosis.
Neurotic symptoms are a way to somehow stabilize the situation, to bring something permanent into your life against the backdrop of the factor that caused the neurosis. Psychologists and psychiatrists note that even without treatment, a neurotic disorder can go away if the trigger factor has been eliminated.
Treatment of neurotic disorders
The main method of treating neurosis is psychotherapy. Deep techniques are often used for this, but rational psychotherapy is increasingly used. The choice of method depends on the clinical picture observed by the psychotherapist. In some cases, immersion in the internal causes of neurosis can only harm the patient, so it is not always necessary to look for a psychoanalyst or Gestalt therapist as a doctor.
Physiotherapy is a method that helps you move from stressful thoughts to feeling your body. Often, the effects of relaxing and restorative massage techniques, swimming, electrical impulse therapy, and gymnastics help to normalize the psychological sphere and get rid of neurosis.
Drugs for the treatment of neurotic disorders are also selected based on the symptoms observed by the doctor. Tranquilizers and antidepressants are used only when other treatment methods have no effect without them, and are discontinued whenever possible when a lasting effect from treatment is obtained.
Sedatives and nootropics are used during the entire course of therapy, depending on the clinical picture. Glycine , a drug created by microencapsulation of the amino acid of the same name, is prescribed as a permanent drug for the complex treatment of neuroses The use of Glycine allows you to gradually restore the protective capabilities of the nervous system from the inside, increasing resistance to neurotic disorders.
Prevention of neurosis
Stress is an integral part of life, and neurotic disorder can be caused by any of them. By correctly experiencing stress, you help the nervous system cope with the load and avoid fixing the problem in the form of neurosis
- If you are experiencing negative emotions, it is important to give them an outlet. Playing sports, in particular martial arts, helps a lot with this. But any socially acceptable way to relieve stress will be helpful. Just don't relieve stress with alcohol
- Rest, sleep as much as you need to recover. Don't work too hard and take your vacation on time. Simple methods of protecting yourself from overload help you stay healthy
- Resolve conflicts as they arise, do not hide emotions for the greater good. This approach to maintaining peace will not be useful to either side.
- Take Glycine to prevent neuroses. The amino acid glycine improves energy production in the nervous system and protects it from overload. The drug is safe for children and adults, recommended for stress.
VSD exacerbation, neurosis...
Ekaterina, Moscow
7243 views
November 23, 2020
Good evening, dear doctors. I am asking you for advice, because the district clinic refused to issue a referral to a neurologist, citing the pandemic... all that remains is to crawl back. I have VSD and am hypotensive, working pressure is 90/65, and tachycardia, pulse at rest is approximately 85. A week ago, osteochondrosis (chronic in the cervical and thoracic region) worsened. Or rather, I thought so... There is no obvious pain in the back (as happened before). But my head is terribly dizzy, or more precisely, it’s not dizzy, but moving. There is a sharp reaction to all sharp sounds and light. It all started with stress about 1.5 weeks ago. The night after the stress I couldn’t sleep, my blood pressure dropped to 80/54. My arms and legs were icy, and I was shaking all over, pounding inside, tremors in my hands. You fall through in a dream and are thrown back out of sleep with terrible tachycardia, it was very scary. And then everything went like clockwork. My stomach hurt, I urgently had a gastroscopy and colonoscopy, and my gastritis worsened. A bad blood test came back: Bilirubin 37, Hemoglobin 149, Cholesterol 7.8. I went on a diet. And my condition began to deteriorate sharply. The local therapist recommended a standard set for chondrosis, namely Costarox + Neuromultivit IM + Cerebrolysin 5 ml IM + Amelotex ointment. And of course Mydocalm 125 2 rubles per day + Omeprazole. This scheme helped me before. This time everything went wrong. Mydocalm just made me crawl, feel sick, my head felt like it was under water. I lasted 3 days, couldn’t drink anymore, stopped drinking, although my head cleared up. So far the rest of the treatment is of no use. Cerebrolysin causes an eerie ringing in the ears, and all sounds become aggravated. My hands and feet are constantly icy, attacks of dizziness are accompanied by some kind of hot flashes. It’s simply impossible to eat, nausea. And then I decided to drink Afobazol... and a miracle: my stomach begins to let go, it straightens up as if it were something, my back lets go a little, the warmth comes straight out. On the contrary, from injections there is a feeling of burning, burning and tingling. This makes me doubt that this is real neuralgia - but if afobazole helped for the first 4 days, now everything has returned to a pinched state again, with regular use. Feeling good after a warm bath, everything is warm, the head clears, but not for long, about 40 minutes. And again dizziness, nausea, and an unsteady gait sets in with hot flashes. Vessels have always been a weak point. Please tell me an adequate treatment regimen for neurosis, based on low blood pressure (all muscle relaxants make the condition even worse). And Afobazole, by the way, normalizes blood pressure and the pulse is noticeably lower. I am sure that the back pain is neurological in nature. Once upon a time, I was prescribed Sirdalud, Grandaxin - they generally make me feel terrible, panic, fear... I don’t even know how I can relax my back muscles, and most importantly, get rid of dizziness. I have an active life, I have a small child, I don’t sit still. And now I feel like a vegetable (not in my body, but from the outside). unpleasant and scary feeling. Neurosis is my guess, there is no one to diagnose...
The question is closed
VSD
Neurosis.
bad condition
Panic attacks. Stop being afraid of them. Psychologist's advice
Many people complain about panic attacks, but not everyone understands the essence of this phenomenon and therefore they are even more afraid. Often people who have experienced a panic attack are so frightened by this that they subsequently live in constant fear of a repetition of this “terrible” state.
Let's clarify what this disorder consists of and why it causes such a public outcry.
One should not think that panic attacks are something new, hitherto unknown to science, it’s just that in our age of loud slogans they have received a new name, brighter and more noticeable than “paroxysmal anxiety disorder”, “VSD” or “sympathoadrenal autonomic crisis”. Of course, doctors knew about this disorder before the beginning of the twenty-first century, it’s just that people in non-medical professions knew less about it, and with the advent of the Internet, panic attacks began to seem like the trend of the century.
The disease manifests itself in the form of sudden attacks of anxiety, accompanied by an increase in heart rate, sudden changes in blood pressure, sweating, discomfort in the chest and abdomen, often a feeling of nausea, a feeling of shortness of breath, palpitations, dizziness and an altered perception of what is happening, and often reaches the fear of losing sanity or sudden death. No wonder: the person just felt quite comfortable, and suddenly there is such a “bouquet” of bright unpleasant symptoms. The emergence of fear logically follows from the above, but, unfortunately, it further aggravates the condition.
One of the means of combating diseases is prevention, so in this case, developing a certain attitude towards such attacks in advance means coping with them to a large extent.
Anxiety is fear without an object, fear of uncertainty, the unknown. In the modern metropolis there are too many factors influencing a person, so it is not surprising that anxiety disorders are so common. And if an anxious person has an attack with increased heart rate, a surge in blood pressure, and dizziness, whoever wants to think about a heart attack or stroke. Fortunately, anxiety attacks go away on their own in a short time, leaving no consequences.
Fear and anxiety are necessary feelings that prepare us to face danger. We must be ready to run away or fight, and therefore fear and anxiety are associated with rapid changes in the body.
Firstly, to react quickly, you need speed - and the amount of adrenaline in the blood rapidly increases. Secondly, it is important to prepare more strength - and at the same time the heartbeat increases, the breathing rate increases (even a feeling of lack of air appears) in order to deliver more oxygen and nutrients to the muscles, and thirdly, for the same purpose, the vessels serving the muscles dilate.
At the same time, all other processes in the body slow down, the vessels in the digestive system narrow, and the stomach shrinks. Associated with this are two symptoms that are similar in their purpose – “bear sickness”, that is, the urge to empty the intestines in a stressful situation, and nausea – as the intention not to waste effort on unnecessary digestion at this moment.
Sweating is explained by intense metabolic processes in the muscles and an increase in temperature, and dizziness is explained by the same increased blood circulation: the brain receives too much oxygen and “gets drunk”, which, against the background of anxiety, can easily be confused with a violation of the perception of reality.
To distinguish a panic attack from a stroke, you need to remember that a stroke is accompanied by numbness or muscle weakness, and loss of the ability to speak. During a panic attack, body and facial movements may be symmetrical. During a heart attack, the pain behind the sternum is prolonged, there may be pain in the left arm, and fear appears due to pain. With panic, a lack of air is felt to a greater extent; fear is associated not with pain, but with pulse rate, increased pressure, dizziness and, in fact, is not a consequence, but a cause.
If you experience sudden attacks of anxiety, it is important to know that their physical, bodily manifestations are not dangerous, because they are not caused by poison entering the body, or a sudden failure in the functioning of important body systems - no, this is a chain of reactions that the brain launched in order to prepare you for an emergency response to an uncertain life situation. In the entire history of medicine (since the time of Hippocrates), not a single case of a panic attack has been recorded that would have led to any serious complication or death. On the contrary, doctors observe such a pattern that people with panic attacks are distinguished by good physical health, their life expectancy is usually longer than the average.
As clinical experience shows, those who cease to be afraid of the recurrence of panic attacks get rid of them forever!
Of course, it would also be wrong to treat a symptom such as a panic attack with disdain, so it is important to get checked by a psychiatrist or psychotherapist, and sessions with a psychologist will help you correct the reason why your brain considers current life circumstances to be dangerously uncertain.
Treatment of panic depressive disorder
For drug therapy, we use a combination of anxiolytics and antidepressants. In this case, preference is usually given to modern drugs from the group of selective serotonin reuptake inhibitors, which practically do not cause serious adverse reactions. The dosage and regimen are always selected individually.
In addition to drug treatment for panic depressive disorder, psychotherapy is very important. The doctor must not only understand the reasons for the patient’s depressed state, numerous complexes, and anxiety, but also teach him to overcome fear and panic. To do this, the specialist simulates a stressful situation and helps the patient cope with it.
Typically, treatment for panic depressive disorder is carried out on an outpatient basis. Hospitalization is possible at the patient’s request for diagnostic examination and the initial stage of therapy.
An individually selected course of treatment allows you to cope with the main symptoms of the disease and prevent panic attacks. Call us at +7 (495) 367-23-13 at any time - we work around the clock. Our operator will answer all your questions, select a convenient time for a visit to the clinic or fill out an application to call a doctor at home.
Panic attack
A panic attack develops very quickly and unpredictably, under the influence of causes known only to the patient. It is characterized by:
- sudden onset;
- relatively short duration (usually 10–15 minutes, less often - up to several hours);
- rapid progression of symptoms (within minutes).
The attack is accompanied by:
- severe tachycardia;
- feeling of suffocation, inability to take a breath;
- hot flashes and diffuse sweating;
- fear of impending death;
- disorientation;
- convulsions, decreased tactile sensitivity.
Panic attacks can be:
- Spontaneous, developing without a clear connection with any circumstances.
- Attributive, arising in certain situations. For example, frightening videos from the scene of an accident or terrorist attack provoke a panic attack on public transport, news about the spread of an infectious disease leads to aggravation in crowded places, etc.
The influence of Afobazole on the quality of life of cardiac patients during inpatient treatment
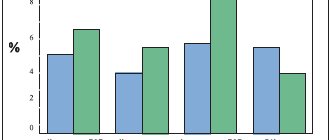
The short stay of the patient in the hospital (about 2–3 weeks) poses the attending physician the task of finding effective techniques that affect quality of life in the most common nosological forms: hypertension (HTN) and coronary heart disease (CHD). This pathology is accompanied by a diverse range of subjective symptoms of maladjustment (general weakness, increased fatigue, deterioration of memory and ability to concentrate, anxiety, decreased mood, and others), which are constantly in the focus of the patient’s attention, and not the blood pressure numbers or the electrocardiogram curve - important objective criteria from a doctor's point of view. Such a discrepancy in views leads to the destruction of the therapeutic alliance between the doctor and the patient, disappointment from contact and the formation of a negative attitude toward following recommendations upon discharge, regardless of the correct drug therapy in accordance with the standards of treatment. The prevalence of adaptation disorders in cardiological practice reaches 51%, the treatment of which seems to be a difficult and at the same time urgent task. Over the past decades, in the treatment of borderline mental disorders, priority has been given to benzodiazepine tranquilizers; Using epidemiological data, a constant increase in their consumption has been established. Long-term use of tranquilizers has shown their wide therapeutic potential. Negative manifestations of the clinical effects of benzodiazepines include side effects, including hypnosedative and muscle relaxant effects, depression of cognitive functions and a decrease in daily activity, changes in tolerance with long-term use and the presence of a predisposition to addictive mental disorders. In the early 80s of the 20th century, the leading laboratories in the world raised the question of creating a drug that would correspond in its anti-anxiety properties to benzodiazepine tranquilizers, but would be free of hypnosedative, muscle relaxant and “amnestic” effects. At the State Research Institute of Pharmacology named after. V.V. Zakusov RAMS, as a result of 15 years of research, the original anxiolytic Afobazole with an optimal balance of safety and effectiveness was obtained [12]. Purpose of the study. To evaluate the effect of Afobazole on the quality of life of cardiac patients during inpatient treatment in the presence of psychosomatic disorders. Material and methods QoL was studied using the international adapted SF-36 methodology [8,14,15] in 95 cardiac patients who were in hospital (23 people with stage II hypertension and 22 with coronary artery disease, angina pectoris of functional class II), who During the first 10 days of hospital stay, Afobazole was additionally prescribed at a dose of 10 mg 3 times a day due to the presence of adaptation disorders. A comparative analysis of the dynamics of quality of life for the same period was carried out in a group of 27 patients with stage II hypertension and 23 patients with coronary artery disease: angina pectoris of functional class II against the background of traditional treatment using phenazepam 25 mg at night. Standard therapy according to the formulary system for hypertension and coronary artery disease included b-blockers, ACE inhibitors, and statins. Statistical data processing was carried out using paired Student's t test using the SPSS software package, version 10.0. Results and discussion In clinical settings, the safety and effectiveness of Afobazole in the treatment of borderline mental disorders has been shown: in psychiatry, cardiology, endocrinology and obstetric and gynecological practice [1–12]. The study of the effect of Afobazole on the quality of life of patients with hypertension was preceded by a study of this indicator in 27 patients against the background of standard therapy. The results of statistical data processing are presented in Table 1 and Figure 1. The results of statistical processing of the SF-36 test against the background of standard therapy revealed an improvement in the quality of life on the SF scale at the trend level, the P criterion was 0.059. In the group of patients taking Afobazole, the quality of life profile significantly changed in several indicators, as shown in Table 2 and Figure 2. The data obtained indicate a significant improvement in the quality of life of patients according to the B, OH and F scales of the SF-36 test. Improvement in scores on the B scale indicates an increase in the ability of patients to engage in daily activities, including housework and outside the home. The OZ scale reflects the patient’s best assessment of his current condition and treatment prospects, and an increase in indicators on the F scale reflects an increase in vital activity. During Afobazole therapy, the tendency (p=0.089) for patients to increase social contacts remained [8]. Ten-day therapy of patients with coronary artery disease did not affect the improvement of their quality of life, either when using standard prescriptions or when taking additional Afobazole. The dynamics of QOL after a course of therapy with Afobazole in the study group of patients are presented in Table 3 and Figure 3. Based on the study of test indicators, an improvement in the QOL of role-emotional functioning was found at the level of a trend (p = 0.68), which suggests a decrease in the influence of the patient’s emotional state on the performance of them in daily activities (including large amounts of time spent, a decrease in the amount of work, a decrease in its quality) and mental health (p = 0.097), which corresponds to a decrease in anxiety and depressive symptoms [8]. Conclusion Thus, a course of treatment with Afobazole for patients with hypertension and coronary artery disease for ten days against the background of standard therapy in a hospital setting allows one to obtain a significant improvement in the quality of life in patients with hypertension, its physical and psychological components. Considering that the maximum effect from taking this drug occurs after 4 weeks, it should be concluded that this drug has the potential to influence the quality of life in patients with coronary artery disease, which, of course, can only be stated after further studies in the conditions of outpatient use of Afobazole until the symptoms of maladaptation are completely eliminated or stabilization of psychosomatic status.
Literature 1. Avedisova A.S. New anxiolytic “Afobazol” in the treatment of generalized anxiety disorder (results of a comparative study with diazepam) / Journal. Psychiatry and psychopharmacotherapy (extra-issue). – 2006. – P.13–16. 2. Avedisova A.S., Chakhaeva V.O. The use of the anxiolytic afobazole in the treatment of generalized anxiety disorder (information letter). – M., 2006. – 12 p. 3. Akarachkova E.S. Afobazole is a modern pathogenetic therapy for patients with neurocirculatory dystonia/breast cancer. – T.14, – No. 16. – 2006. – P.11–13. 4. Antonova K.V. thyrotoxicosis. Mental change. Treatment options/breast cancer. – T.14, – No. 13. – 2006. – P.14–15. 5. Buldakova N.G. Psychopharmacotherapy in cardiology/breast cancer. – T.14, – No. 10. – 2006. – P.8–10. 6. Vasilyeva A.V., Poltorak S.V., Polyakov A.Yu., Solomonova S.V. The use of afobazole in the complex treatment of adaptation disorders/Journal. Psychiatry and psychopharmacotherapy (extra-issue). – 2006. – P.24–26. 7. Neznamov G.G., Syunyakov S.A., Chumakov D.V., Teleshova E.S., Davydova I.A., Grishin S.A., Mametova L.E., Syunyakov T.S. New anxiolytic afobazole: results of a comparative clinical study with diazepam in generalized anxiety disorder / Journal. Psychiatry and psychopharmacotherapy (extra-issue). – 2006. – P.17–23. 8. Novik A.A., Ionova T.I. Guidelines for quality of life research in medicine. – St. Petersburg: Publishing House “Neva”; M.: “OLMA-PRESS Star World”, 2002. – 320 p. 9. Pogosova G.V. Modern approaches to the diagnosis and treatment of depressive spectrum disorders in general medical practice (a manual for doctors) / Scientific and practical peer-reviewed medical journal (appendix). – No. 1., 2007. – 24 p. 10. Serov V.N., Baranov I.I. Tranquilizers in obstetrics and gynecology practice/breast cancer. – T. 14, – No. 18. – 2006. – P.3–7. 11. Smulevich A.B., Andryushchenko A.V., Romanov D.V. Psychopharmacotherapy of borderline anxiety disorders (comparative study of the anxiolytic effect of Afobazole and oxazepam in patients with adaptation disorders and generalized anxiety disorder)/BC. – T.14, – No. 9. – 2006. – P.3–7. 12. Smulevich A.B., Andryushchenko A.V., Romanov D.V., Siranchieva O.A. Therapy of borderline mental disorders (study of the effectiveness and tolerability of afobazole)/Mental disorders in general medicine. – No. 1. – 2006. – P.10–16. 13. Nilsson P., Brandstrom H., Lingfors H., Erhardt L., Hedback B., Israelsson B., Sjoberg G. National program of quality assurance in secondary prevention in Sweden. Gender differences in secondary prevention of coronary heart disease: reasons to worry or not?//Scand. J. Prim. Health Care. – 2003. – No. 21. – R.37–42. 14. Ware JE, Kosinski M., Keller SD SF–36 Physical and Mental Health Summary Scales: A User's Manual//The Health Institute, New England Medical Center. Boston, Mass. – 1994; https://www.rhinology.ru 15. Ware JE, Snow KK, Kosinski M., Gandek B. SF–36 Health Survery. Manual and interpretation guide//The Health Institute, New England Medical Center. Boston, Mass. – 1993. 16. Wehler M., Geise A., Hadzionerovic D., Aljukic E., Reulbach U., Hahn EG, Strauss R. Health–related quality of life of patients with multiple organ dysfunction: individual changes and comparison with normative population.//Crit. Care. Med. – 2003. – No. 31. – R.1094–1101.