Violation of the rheological properties of blood and its fluidity is a significant risk factor for the development of dangerous processes, primarily thrombosis.
Such clots provoke blockage of blood vessels, which immediately leads to emergency conditions, death, or requires immediate surgical intervention due to tissue death - gangrene.
Thrombosis therapy involves the use of a special group of medications like Urokinase. They have a lot of side effects, so they are used with great caution and in the most extreme cases. As a preventive measure, other means are prescribed.
Antiplatelet agents are a special type of drugs used to prevent the clumping of formed blood cells, platelets, and others as part of prevention.
Prescribed for the treatment of most cardiovascular pathologies in the acute phase and during the rehabilitation period. They should also be used with great caution, because they thin the blood and can cause dangerous complications.
Accordingly, neither thrombolytics nor antiplatelet agents can be used without permission. The issue is always resolved strictly at the discretion of the doctor.
Mechanism of action
Antiplatelet drugs (another name for this pharmacological group) have a complex way of influencing the body.
First of all, the effect is on blood clotting. The basis is the regulation of the biochemical characteristics of hemostasis.
Without going into the complex features of the process, we can say that ultimately a group of effects is achieved:
- Decreased platelet aggregation. Simply put, their sticking together is a result of an inadequate condition. The main clinical effect gives the name to the drugs of this type.
- Blood thinning. Achieved indirectly. The rheological properties of the fabric are restored. Due to this, a change in viscosity occurs, normalizing the pressure on the walls of blood vessels. Additionally, degeneration of the endothelium of arteries and veins is prevented.
However, long-term use of antiplatelet agents is not possible. Because there is a high risk of developing dangerous bleeding, which can lead to death.
Moreover, it is unacceptable to use drugs from this pharmaceutical group while taking thrombolytics (Uro-, streptokinase and other medications).
There is another type of drug, which is very similar in properties and clinical effect to the one described. These are the so-called anticoagulants. Often even doctors use both terms as synonyms, however, these are different types of drugs.
The second among those mentioned have an active effect, work faster, the effect is short-term, but much more pronounced.
Rapid blood thinning is observed, which makes anticoagulant drugs ideal for preventing the formation of blood clots, especially in emergency conditions. It makes sense, however, to approach the purpose and use with great caution.
The danger of such medications is also many times higher, which can put an end to health or even life if used incorrectly.
Attention:
The parallel administration of anticoagulants and thrombolytics is strictly prohibited. Because the risk of massive internal bleeding increases several times.
Thus, the basis of disaggregants is the ability to influence biochemical processes in the body and the composition of the blood, preventing the adhesion of its formed cells and the formation of blood clots.
Natural antiplatelet agents and anticoagulants
Some foods, dietary supplements and herbs have blood thinning properties. Naturally, they cannot be supplemented with medications already taken. But in consultation with your doctor, you can use garlic, ginger, ginkgo biloba, fish oil, and vitamin E.
Garlic
Garlic is the most popular natural remedy for the prevention and treatment of atherosclerosis and cardiovascular diseases. Garlic contains allicin, which prevents platelets from sticking together and forming blood clots. In addition to its antiplatelet effects, garlic also lowers cholesterol and blood pressure, which are also important for cardiovascular health.
Ginger
Ginger has the same beneficial effects as antiplatelet medications. You need to consume at least 1 teaspoon of ginger every day to notice the effect. Ginger can reduce the stickiness of platelets and also lower blood sugar levels.
Ginkgo biloba
Consuming ginkgo biloba can help thin the blood and prevent platelets from becoming too sticky. Ginkgo biloba inhibits platelet activating factor (a special chemical that causes blood to clot and form clots). Back in 1990, it was officially confirmed that ginkgo biloba effectively reduces excessive platelet adhesion in the blood.
Natural supplements will also help prevent the development of thrombosis
Turmeric
Turmeric can act as an antiplatelet drug and reduce the tendency to form blood clots. Some studies have shown that turmeric may be effective in preventing atherosclerosis. An official medical study conducted back in 1985 confirmed that the active component of turmeric (curcumin) has a pronounced antiplatelet effect. Curcumin also stops platelet aggregation and also thins the blood.
But it is better to avoid foods and dietary supplements that contain large quantities of vitamin K (Brussels sprouts, broccoli, asparagus and other green vegetables). They can dramatically reduce the effectiveness of antiplatelet and anticoagulant therapy.
Acetylsalicylic acid
And its derivatives. The most common group of pharmaceuticals in medical practice with high proven effectiveness.
When compared to the other types described below, these drugs are about average in safety and effectiveness.
The classic and long-outdated Aspirin is currently still actively used, despite the high risks.
It does a good job of urgently restoring blood flow, but is absolutely not suitable for long-term use. As part of modern practice, its safer analogues are prescribed.
Aspirin-Cardio
Perhaps the most popular modification of the drug based on acetylsalicylic acid. It has a different dosage than its predecessor and is positioned as a means for the systemic, complex treatment of cardiovascular diseases.
Whether this is true or not, doctors have not come to a consensus. The main feature of Aspirin-Cardio is the possibility of long-term use with fewer risks to health and life.
The antiplatelet effect is achieved after several days of use, so the product can be considered relatively safe.
At the same time, in addition to restoring the rheological properties of liquid connective tissue, Aspirin-Cardio relieves inflammation, pain, and normalizes body temperature.
Such non-selectivity can play a cruel joke; you need to be careful when using it and carefully monitor your own feelings.
The concentration of acetylsalicylic acid in this drug is three times higher than in the classic variation of Aspirin, which also imposes a lot of restrictions. All issues are resolved at the discretion of the treating specialist.
Thrombo-ASS
In fact, there is no big difference between the old analogues based on acetylsalicylic acid and this name. In both cases, the concentration of the active substance is identical.
The difference lies in the form of release. The coating of the drug Thrombo-ACC prevents the rapid absorption of acid in the digestive tract and reduces the destructive effect of this phenomenon.
Therefore, the medication is considered not so aggressive towards the organs of the gastrointestinal tract. The advantage is quite controversial, taking into account the mass of analogues of other groups, as well as the higher cost of Trombo-ACC.
In any case, the issue of choice and appointment is decided by doctors. Unauthorized use is not possible if there is a desire to preserve health.
Aspicor
It has a minimal dosage of acetylsalicylic acid, in addition, it is considered safer than aspirin-containing analogues, not as aggressive and “clean”, therefore it can be used indefinitely as a maintenance treatment. But not in the “role” of the only medicine, but in the system.
The cost of Aspicor also makes the drug simple and affordable, because the price is not much different from that of a regular obsolete analogue.
In all cases, medications based on acetylsalicylic acid have a significant disadvantage. They are not selective.
The antiplatelet effect is complemented by an anti-inflammatory and antipyretic effect; it is logical that the drug affects many functions and organs, including the digestive tract and heart.
If used excessively, it can cause bleeding and increases the fragility and permeability of blood vessels.
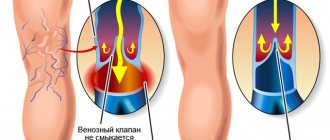
Is Detralex an anticoagulant or not?
- Detralex is classified as a venotonic . The active ingredient of the drug is the semi-synthetic flavonoid diosmin, which has a positive effect on venous tone.
- The action of Detralex is aimed at reducing the period of blood passage through the veins, strengthening the walls of capillaries and preventing the development of varicose veins. The drug is prescribed for varicose veins and hemorrhoids. Available in tablets and cream form for external use.
Drugs
ADP blockers
Agents that reduce the effect produced by a special substance - adenosine phosphate. This compound provokes platelet clumping through a complex bond with fibrinogen, therefore drugs of this type affect the fundamental processes of thrombus formation.
Moreover, unlike the previous ones, they are more selective and are used with less caution, although they can cause harm if used incorrectly.
Ticlopidine
A relatively old, well-studied name. The product was first synthesized in the late 70s of the last century. It is still actively used, represented by a list of trade names: Tiklid, Tiklo, Aklotin, Tagren.
The drug is used both as part of urgent care for emergency conditions, and for the treatment of chronic diseases associated with a violation of the rheological properties of the blood.
Basically, the medication is prescribed for the purpose of treating long-term conditions, preventing dangerous complications, and thrombosis. The question is open and remains at the discretion of the doctor.
Clopidogrel
There is no consensus in the medical community about what is more effective, this name or Ticlopidine. The authors hold different points of view.
However, practitioners agree that before and after surgical interventions, especially for cardiac diseases, preference should still be given to Clopidogrel, as it is the optimal combination of effectiveness and safety.
It is not prohibited to use the pharmaceutical product either in emergency conditions or for a long time, depending on the indications.
In any case, both names have significant potential and can be dangerous if used incorrectly.
Medicines to reduce the effect of ADP are also taken in isolation, as the main ones in therapy. Especially in mild cases, but more often prescribed in a system with others. Depends on the situation.
Is Curantil an anticoagulant or not?
- Curantil tablets are prescribed for the prevention of arterial and venous thrombosis, as well as for disorders of cerebral and arterial circulation.
- The principle of operation of Curantil as an anticoagulant is to prevent platelets from sticking together into clots. In addition to the main function, the composition of Curantil tablets has an immunomodulatory effect, which helps minimize viral and colds. The complex effect is the advantage of this drug.
- Curantil is prescribed for the prevention of strokes and heart attacks, and also as a component of complex treatment of a specific disease.
For thrombosis
Phosphodiesterase inhibitors
They influence another mechanism of blood clot formation. They have fewer contraindications and are considered safer when compared with the previous two pharmaceutical groups.
It makes sense to use them after emergencies, surgical interventions during the rehabilitation period, or as medications for the prevention of heart attack, stroke, and acute hemodynamic disorders associated with changes in blood properties.
Common names include Dipyridamole, Triflusal. Both are relatively old. They have several trade names that differ from the main ones, for example Curantil.
They often provoke allergic reactions, therefore they require careful prescription and monitoring of the patient’s condition.
GPR blockers
Agents that reduce the sensitivity of platelet glycoprotein receptors act mildly and are relatively rarely tolerated.
The basis of the influence of medications of this type is the ability, relatively speaking, to instruct platelets not to interact with factors that provoke aggregation, that is, their sticking together.
The rheological properties of blood change slightly; the effect of HPR blockers is high, but short-lived. Therefore, it makes sense to use the remedy either within the framework of acute conditions or to select a clear regimen and dosage.
Among the names are Eptifibatide (Intergrilin), Tirofiban, and others.
Medicines of this type are most widely used when used in patients with acute conditions in a hospital. For example, with coronary insufficiency.
It also makes sense to use them in a system with classical medications based on Aspirin.
Is Clexane a direct anticoagulant or not?
- Clexane is a modern analogue of heparin, prescribed for the prevention of venous embolism and thrombosis that occurs during surgical interventions, cardiac and respiratory failure, angina pectoris and other pathologies. Clexane is a direct-acting anticoagulant. With its participation, a number of chemical reactions in the blood are triggered - enzymatic coagulation.
- Injections with the blood-thinning anticoagulant drug Clexane are administered twice a day for two weeks. As with other anticoagulants, Clexane has a side effect - the likelihood of bleeding, especially in older patients. The drug is used only for monotherapy and is not combined with other substances.
Arachidonic acid production inhibitors
Reduce the rate of synthesis of the named substance. In general, they are similar to the previous group of medications with an antithrombotic effect. The difference is selectivity.
This category of drugs affects many factors of platelet “clumping”, and therefore poses a much greater danger to the health and life of the patient than others.
When using it, you need to constantly monitor the person’s condition over time. To quickly adjust the dose or discontinue the drug.
Among the names: Indobufen, Ibustrin and others.
What is the difference between anticoagulants and antiplatelet agents?
Having studied the properties of the two types of drugs, we can come to the conclusion that they are both designed to do the same job (thin the blood), but using different methods. The difference between the mechanisms of action is that anticoagulants usually act on proteins in the blood to prevent the conversion of prothrombin to thrombin (the key element that forms clots). But antiplatelet agents directly affect platelets (by binding and blocking receptors on their surface).
When blood clots, special mediators released by damaged tissues are activated, and platelets respond to these signals by sending special chemicals that provoke blood clotting. Antiplatelet drugs block these signals.
Herbal remedies
Their pharmacological effectiveness has not been proven. These are medicines based on Ginkgo Biloba.
Such “medicines” do not make much sense in purchasing and using them for their intended purpose.
This also includes conventionally “folk” recipes based on ginger, St. John’s wort and others. This is not a treatment, just an amateur activity.
Herbs can be used as an aid only if the doctor agrees to it. Therapy does not tolerate creativity; it requires common sense, accurate calculations and analytical work.
Other drugs
These include those used for long-term treatment of abnormalities: Pentoxifylline (the most popular in clinical practice), Reopoliglucin (identical to the previous one, but safer and used in a wide range of cases).
Another type is complex medicines, which contain several components.
For example, Cardiomagnyl (Aspirin and magnesium, respectively), Aspigrel, Coplavix, Agrenox and others. The doctor decides whether it is worth prescribing such “explosive mixtures”.
In most cases, precise dosing is required, so it is better to give preference to two separate items.
It is safer, more effective and provides the doctor with the tools to fully control the process.
Moreover, the price of such “hybrids” is quite high, which completely eliminates any objections on this score from manufacturers. The issue is decided at the discretion of the treating cardiologist.
Antiplatelet therapy in patients with stable angina
Lecture transcript
XXV All-Russian Educational Internet Session for doctors
Total duration: 18:02
00:00
Vladimir Trofimovich Ivashkin, Chairman of the Interdepartmental Scientific Council on Therapy of the Russian Academy of Medical Sciences, Academician of the Russian Academy of Medical Sciences, Doctor of Medical Sciences, Professor:
— I would like to introduce Professor Grigory Pavlovich Arutyunov, already known to you. He will begin the anniversary XXV Internet Session with a very interesting, in my opinion, message: “Antiplatelet therapy in patients with stable angina.” Please, Grigory Pavlovich.
Grigory Pavlovich Arutyunov, Doctor of Medical Sciences, Professor, Head of the Department of Therapy of the Moscow Faculty of the State Educational Institution of Higher Professional Education "RGMU RosZdrava", Vice-Rector for Medical Work of the State Educational Institution of Higher Professional Education "RGMU RosZdrava", Honored Doctor of the Russian Federation:
— Thank you very much, Vladimir Trofimovich. Dear comrades! I would like to draw your attention to the problem of platelet aggregation, since it is becoming one of the most important. We are trying to fight for the restoration of myocardial blood flow and peripheral blood flow in patients with coronary heart disease.
This is an extremely important point. We must firmly remember that not only the surgeon must fight for the restoration of blood flow and its preservation, but the therapist must fight in the daily planning of treatment for patients with coronary heart disease. Let's look at the basic methodology of modern cardiology.
We will look at understanding the continuum. Any cardiologist and therapist understands that there is a continuous series of events that gradually develop in the vessel of each patient: from silent plaque growth we move on to an unstable plaque.
Please note that as the plaque transitions from one state to another, a blood clot develops on it. We see an acute myocardial infarction, during which the development of repeated myocardial infarction is possible.
Again, the basis is a change in local blood flow in the peri-infarction zones, which allows the focus of necrosis to spread and expand. At the terminal stages, when severe circulatory failure develops, impaired peripheral circulation due to increased platelet aggregation, due to the development of thrombosis, the prognosis sharply worsens.
If we layer the concept of thrombus formation on the foundation of the methodology of modern cardiology, on the atherosclerotic continuum, I think you will agree with me that the struggle for blood fluidity, for the preservation of the lumen of the vessel becomes a defining event.
02:20
Let's look at the fundamental drugs, which from the point of view of world cardiology are the basis for preserving the lives of our patients. Please note that in the dark square there are four classes of drugs that regulate and truly affect the reduction in the likelihood of death in patients.
These are acetylsalicylic acid and clopidogrel. These are statins and must be titrated to achieve the target cholesterol level. These are beta blockers and ACE inhibitors. Today I will allow you to draw your attention to the issue of aspirin and clopidogrel as the basis of drugs that affect blood fluidity and aggregation.
Let's see how an atherosclerotic plaque develops. Here is one of the options for the development of a plaque. The plaque grows into the lumen of the vessel. You can clearly see how its size increases as the patient ages. It may sooner or later crack, tear, or even not collapse completely, but a blood clot will grow on it.
There is another form of plaque growth. The plaque grows into the vascular wall. The paradox is that this plaque can rupture or tear. The endothelium above it can also be damaged, which will lead to thrombus formation.
Let's look at more modern views on atherosclerotic plaque.
You can see very clearly that the plaque is always a ring (it is now illuminated in yellow on your screens). The plaque does not break through. The arrow shows where the intracoronary ultrasound probe is located. It is natural to imagine that along such a long length of an atherosclerotic plaque, in its strange spatial shape, the probability of plaque rupture becomes obvious and highly probable.
A simple tear, and not destruction, will always lead to a change in its properties. Platelets will begin to adhere, and fibrin filaments will begin to fall out on the adhered platelets, on which other blood cells will sit. This is how a blood clot grows in the lumen of a vessel. The basis was abnormal platelet aggregation, increased platelet aggregation and the pathological process they started.
04:37
It's very important for us to introduce the bottom of this slide where it says "thrombus."
When a blood clot has formed, then only thrombolytics will help. When a network of fibrin threads has formed, in which the formed elements of the blood are entangled, only thrombolytics will help. The therapist must be very clear about all the stages of this process. We need to intervene early.
It is very difficult to dissolve such a network. Look, this is a dense network in which the formed elements of blood sit. It is very difficult to dissolve it. It is much easier to intervene at earlier stages. Let's see what antithrombotic therapy drugs we can use today.
- The first group is everything that affects platelet adhesion and aggregation.
- The second group is what inactivates thrombin.
- The third group is vitamin K dependent coagulation factors.
- The fourth group is what destroys the formed blood clot (thrombolytics).
Let's look at the first stage, where the therapist must work in his daily routine. These are three possible directions for blocking platelet aggregation.
The first (the most common in the world). This is an effect on platelet aggregation inducers and their receptors. The second (more theoretical - difficult to apply or not at all used in everyday practice) is the effect on the systems of secondary messengers (those compounds that transmit a signal from the surface of the platelet into the cell). Finally, a new, unfortunately, has not yet proven itself as we would like (at least in everyday practice), class: action on glycoprotein receptors IIb/IIIa.
The second class is not used not because it has been little studied, but because it is well known: representatives of the second class are not used as disaggregants, since they are nonspecific only for the platelet. They can cause severe vasodilation and a decrease in blood pressure, which will sharply worsen the prognosis of a patient with coronary heart disease.
Drugs of the first direction, which will influence the perception by the platelet receptor of a signal for aggregation and adhesion to the vascular wall, were discovered a very long time ago - 112 years ago. This is Hoffmann, who discovered the drug, which he called aspirin. About 70 years later, a completely new effect of aspirin (not anti-inflammatory, but in addition to anti-inflammatory) was established: the ability to influence platelet aggregation.
Around the same period, it was established that a significantly lower dose than previously thought inhibited platelet aggregation. Finally, the most important discovery is the effect on cyclooxygenase, which was discovered 40 years ago. This is an irreversible impact. This is very important to remember!
07:24
The therapist should imagine that any changes in the endothelium will cause platelets to adhere. Unfortunately, adhered platelets will lead to the appearance of conglomerates. This is platelet aggregation. There the fibrin threads will begin to fall out. This will already be an irreversible process.
We need to intervene (on the left side of this slide) where we can still stop the pathological process. You and I know for sure that acetylsalicylic acid will affect the level of thromboxane 2. This is a very important issue. You just need to remember, and ASA will achieve its effect within the first 60 minutes after taking the drug. This is an extremely important detail that we will turn to again when we talk about combination therapy.
But it is important to remember the second point. One dose of ASA retains its effect for 11 days. This is the time that a platelet cell lives. Platelets are nuclear-free cells (we know for sure), and if this is so, they are deprived of the ability to synthesize their own proteins. This will mean that one dose will have an effect for 7-10 days. This is an extremely important point.
So, if a drug with a half-life of 20 minutes is effective for the next 7-10 days, it is undoubtedly extremely important in our daily practice. It is very important to note that its effect begins immediately.
What do we know today? The most important thing (highlighted in yellow) is that you don’t have to chase large doses. A dose of 75-150 milligrams has a fairly effective effect on platelet aggregation and adhesion. This has been proven in all major studies.
09:09
Look: simply using ASA reduces the likelihood of death from myocardial infarction by 23%. Almost 50% - the development of a new non-fatal myocardial infarction. Approximately the same 50% – the development of ischemic stroke. In all major studies, aspirin has proven its effect.
What other classes are there besides aspirin?
These are ticlopidines. What is the problem with ticlopidines? Firstly, we don't really know how they work. Very significant side effects of this drug have been noted. This influences the development of neutropenia and, unfortunately, a sharp decrease in platelet count.
Any prescription of ticlopidine requires the physician to monitor a clinical blood test. The therapist must interpret these numbers and understand what is or is not happening in the patient's body. When we realized that ticlopidine, a good drug, has a huge number of side effects, attention was paid to a special class - clopidogrel drugs.
Look at the bottom of the slide.
We know that its peak effect will occur on days 4-7. If aspirin - within the first hour, then clopidogrel - 4-7 days. We can think about their possible combination, but we also know another very important thing: clopidogrel is 2-4 times less likely to have any side effects than ticlopidine. This makes him very attractive.
It is important for the therapist to understand that people with enormous comorbidity are coming to him. These are people who have already suffered a myocardial infarction, people with circulatory failure and multifocal atherosclerotic process. It is very important for the therapist to look at the lower limbs, hair, see what kind of pulsation is in the lower limbs, whether the patient experiences a feeling of coldness in the leg, because this is one of the manifestations of atherosclerosis of the femoral arteries.
Such patients have high comorbidity. CAPRIE studies were taken. In these patients, they decided to see whether clopidogrel would help people who had had a myocardial infarction prevent the development of new myocardial infarctions. Huge study: 19 thousand patients. They all received clopidogrel. The fate of these patients was monitored for approximately two years.
11:29
Here's what we managed to establish. The risk of myocardial infarction is reduced by 3.7%. This is a very important event. Ischemic stroke - approximately 7%. But damage to the arteries of the lower extremities is 23.8%. In the group as a whole – by about 9%. We are reaching the plus and this is a huge event. We have obtained a drug with fewer side effects, with fewer manifestations of gastropathy in patients who take it, but with a pronounced effect on multifocal atherosclerosis.
It is very important for us to pay attention that we are starting to talk about a special form of clopidogrel. It's called Lopirel. There are many clopidogrels in various generic versions. Why are we talking about lopirel as a special drug? I want to introduce into this problem.
Lopirel is s or sinistra, or a levorotatory isomer. The history of left-handed isomers goes back to Louis Pasteur. Pasteur first noticed that in acetic acid there are two classes of crystals that rotate a beam of light in different directions - left- and right-handed. He divided them into two classes and didn't even think much of it.
But later it was discovered that levorotatory isomers have completely different medical activity.
Let's look at the example of quinidine.
Quinidine has left-handed and right-handed isomers. It is well known that dextrorotatory isomers have a special anti-inflammatory effect, while levorotatory isomers do not have such an effect. A potent drug used in the treatment of malaria. Levorotatory and dextrorotatory isomers are special drugs in which there is a mixture of left- and right-handed isomers (racemic mixtures).
Typically, clopidogrel is a racemic mixture, and lopirel is a levorotatory isomer. We are now talking about clopidogrel. In this study, we got another very important thing - a reduction in peripheral artery lesions by 23.8%. Since atherosclerosis is absolutely the same in all large arteries, this means that the drug acts in all manifestations of the atherosclerotic process.
13:48
It is very important to look at the fourth line.
It says: 30-day death from myocardial infarction. You see a significant decrease in deaths on the 9th month and on the 30th day, when the patient is still in the cardiology department. This suggests that the use of clopidogrel turned out to be effective both in the acute state (the ninth month is the situation when the patient enters the clinic) and at long-term stages.
In other words, clopidogrel becomes a drug that has equally proven itself in acute conditions in intensive care units and has proven itself in subsequent stages of treatment.
As for the third class of drugs - IIa/IIIb receptors - these are receptors that catch fibrin threads and trigger further thrombus formation. They have shown little success in everyday chronic therapy. They remained for use in surgical patients.
Today the question is: how, in what situations, to use clopidogrel, as the drug that is most interesting for our perception of this aspect of medicine?
First. If the patient is in emergency condition: loading dose – 300 mg. Together with acetylsalicylic acid, the subsequent dose is 75 mg once a day. If the patient is transferred from the intensive care unit to the cardiology department, the usual dose is 75 mg daily in combination with acetylsalicylic acid.
I ask you to pay attention to this.
Acetylsalicylic acid gives effect within an hour. Clopidogrel reaches its maximum on days 4-7. This way you cover the entire period when you start combining these drugs. Outside the hospital, in the clinic - 75 mg once a day (together with acetylsalicylic acid).
It is important to pay attention to the opinions of experts. Clopidogrel is equally effective in ST-segment elevation, when you are even planning thrombolytic therapy, and in patients who have had a myocardial infarction.
We will return once again to the levorotatory isomer. Lopirel is a levorotatory isomer. I have already said that levorotatory and dextrorotatory isomers are different. It is very important to note that this is a completely different form. There is almost 100% levorotatory isomer. The levorotatory isomer, having approximately the same properties as the racemic mixture, has absolute biological equivalence and, very importantly, therapeutic equivalence.
16:16
Therapeutic equivalence implies that a slightly different generic formulation of a drug will have the same effect on the endpoints studied with the other drug. We see absolute proof. The left-handed isomer - lopirel - turned out to be very effective in the treatment of patients with ST segment elevation, without ST segment elevation, in patients with chronic forms at the outpatient stage of treatment of our patients.
It is very important to pay attention to the study called CURE. This study examined patients who had high comorbidity. We looked at how much we can reduce the risk of myocardial infarction after percutaneous intervention on the coronary artery has already been performed.
Look, these are outpatient patients. Every third patient who was on this therapy does not survive a recurrent myocardial infarction. This is a very important find for us. Today we are talking about a combination of two drugs - acetylsalicylic acid and clopidogrel, when we want to achieve greater effect. This adds approximately 9-10% to the effectiveness we give in our daily therapy.
I can only encourage therapists to be more aggressive in influencing blood flow, the likelihood of new blood clots, and reducing this likelihood! This will undoubtedly improve the quality of life and prolong the lives of our patients.
Thank you for your attention.
Vladimir Ivashkin: Thank you very much, Grigory Pavlovich. Very interesting message. We have a lot of questions. I think we'll leave these questions for the next meeting. Thanks a lot!
Indications
{banner_banstat9}
It is impossible to say exactly when you need to take drugs of this type. The list of antiplatelet agents is wide, and the active ingredients also differ. It's worth taking a look at the instructions.
Theoretical speculations make no sense at all, because the question in any case falls on the shoulders of the doctor.
If you present the list on average, you will get the following picture:
- Transient ischemic attacks. Temporary episodes of circulatory disorders. Localization does not play a big role.
- Emergency conditions suffered in the recent past. Heart attack, stroke. In the first case, not everything is so obvious; many medications are not allowed in this situation. In the second one too.
We are talking only about the ischemic type of disorder. Not hemorrhagic, when there was hemorrhage.
- Stable high blood pressure. Hypertension.
- Cardiac surgery performed.
- Obliterating trophic disorders in the lower extremities. For example, atherosclerosis.
- Stroke prevention (read more about primary and secondary measures in this article).
- Coronary heart disease, except in some cases where the drug can cause harm.
The list is very approximate.
Is Xarelto a direct or indirect anticoagulant?
- The active ingredient in Xarelto, a direct-acting anticoagulant, is rivaroxaban. When taking Xarelto, one of the blood clotting factors is destroyed, which prevents the formation of a blood clot.
- The drug is prescribed for deep varicose veins of the leg and pulmonary embolism. Side effects include low blood pressure, headache, allergies , etc. Clinical studies have proven that Xarelto is more effective than Pradaxa.
- Xarelto is prescribed only for the prevention of thrombosis after surgery and is taken strictly according to the regimen in a certain dosage.
Useful reading:
- Composition of a first aid kit
- Allergy medications
- Interaction of drugs with each other and with food
- The drug Bisoprolol
- Drug Modelform
Contraindications
{banner_banstat10}
The same applies to these grounds. The list of antiplatelet drugs is wide; it is impossible to give a complete list without taking into account the specifics of the pharmaceutical product. That's why the abstract is taken.
If we talk about something approximate again:
- Breast-feeding. The active ingredients are transmitted through milk, so use is strictly prohibited.
- Pregnancy in any phase. Will affect the condition of the mother or fetus.
- Age up to 18 years. Contraindication for the predominant number of antiplatelet agents. Use not allowed
- Hemorrhagic stroke, in which bleeding develops into the structures of the brain.
- Heart failure, at any stage. Absolute contraindication.
- Hepatic or renal dysfunction in the active phase, until the condition is compensated. Then - with great care and prudence.
- Ulcer of the stomach, duodenum, mucous membrane of other parts of the digestive tract. Because it is possible to develop bleeding, even fatal.
Even in the absence of clear reasons for refusing use, you need to carefully think about the advisability of using the medication.
Antiplatelet drugs - prescribed for what diseases?
Indications for the use of antiplatelet agents arise against the background of the following diseases:
- acute or chronic myocardial damage;
- previous ischemic stroke;
- hypertonic disease;
- blockage of blood vessels in the lower extremities;
- placental insufficiency;
- previous operations on the heart and blood vessels.
For heart diseases
Antiplatelet agents contraindications:
- stomach and duodenal ulcers;
- increased risk of bleeding;
- renal and heart failure;
- period of pregnancy and lactation.
Side effects
There are relatively many of them. You should start from the name and group of the product. But the question is more transparent.
Particularly common violations among the possible ones:
- Prolonged bleeding that does not stop even after minimal damage: cuts, abrasions. This is almost impossible to avoid.
- Falling blood pressure levels.
- Dizziness, disorientation in space.
- Nausea, rarely progresses to vomiting.
- Allergic reactions. Perhaps the main side effect of the use of drugs to restore the rheological properties of blood.
The intensity varies. It is minimal when a rash forms on the skin before Quincke's edema or even anaphylactic shock. Fortunately, the last option occurs as an exception.
If negative phenomena develop, it makes sense to reconsider the course and regimen of treatment or completely abandon drugs of this type, which is also more of an unfortunate rare case than the rule.
Patients are advised to closely monitor their well-being. If adverse events develop, consult your doctor again.
Is phlebodia an anticoagulant or not?
- Phlebodia is a capillary-stabilizing drug with a pronounced venotonic and anti-inflammatory effect. The active ingredient diosmin improves the functionality and tone of veins, reduces blood stagnation and lymphatic pressure. The principle of action is similar to the drug Detralex. The advantage is a more compact technique.
- The drug Phlebodia is prescribed when venous and lymphatic insufficiency is detected. Active substances improve lymphatic drainage, increase capillary elasticity, eliminate swelling, pain, and trophic disorders. Phlebodia tablets rarely cause side effects such as allergies or gastrointestinal disorders.