Hypotensive effect - what is it? This question is asked by women and men who are faced with the problem of high blood pressure or hypertension for the first time and who have no idea what the hypotensive effect of the drugs prescribed to them by their attending physician means. An antihypertensive effect is a decrease in blood pressure under the influence of a particular drug.
Experienced professional therapists of the highest category at the Yusupov Hospital Therapy Clinic, who are proficient in advanced treatment and diagnostic methods, will provide qualified assistance to patients with arterial hypertension and select an effective treatment regimen that eliminates the development of negative consequences.
Classification of antihypertensive drugs
Medicines that correct blood pressure are divided into two large groups: first-line and second-line drugs. Moreover, they can be of rapid or prolonged action, belong to different pharmacological groups, that is, control different processes in the body.
First line
This is a large group of antihypertensive drugs, which are prescribed from the very beginning for the treatment of already confirmed hypertension, and includes 5 types of medications:
| Group representatives | Pharmacological properties |
| ACE inhibitors: Rasilez, Captopril, Enalapril | Medicines reduce peripheral resistance by expanding the lumen of blood vessels, which leads to a decrease in pressure without changing heart rate or cardiac output - this makes the drugs relevant for CHF. The effect begins after taking the first dose, and over time, a stable stabilization of blood pressure values occurs. Taking the latest generation of drugs improves the functioning of the kidneys and nervous system; the drugs show a minimum of side effects. |
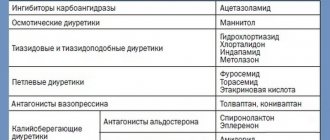
Diuretics
| The drugs have different mechanisms of action and point of application, but all quickly remove excess water from the body along with sodium, relieving the heart and blood vessels. They change water-salt metabolism and metabolism. Contraindicated for gout, but are the drugs of choice for diabetes. |
| Angiotensin receptor blockers (ARBs): Valsartan, Telmisartan, Micardis, Irbesartan, Teveten Plus | The hypotensive effect is based on the ability of the drugs to disrupt the contact of angiotensin with the receptors of the cells of the internal organs, due to which the vascular wall relaxes, the pressure decreases, and the kidneys additionally stimulate the excretion of excess water and salts. Contraindicated for pregnant women and patients with individual intolerance to the components. They have virtually no complications. |
Adrenergic blockers
| They block adrenergic receptors, thereby reducing blood pressure, and at the same time slowing down the heart rate, therefore they are contraindicated for bradycardia. |
| Calcium antagonists: Amlodipine, Verapamil, Verapamil retard, Lercanidipine, Nifedipine retard, Felodipine, Diltiazem | They reduce the penetration of calcium ions into vascular muscle cells, thereby reducing their sensitivity to vasopressors and relieving vasospasm. Metabolic processes remain inert, while the level of left ventricular hypertrophy decreases, which reduces the risk of stroke. |
Second line
Antihypertensive drugs of this group are recommended for the relief of essential (primary) hypertension only in certain patients, for example, pregnant women, the elderly, and all those for whom expensive drugs are an unbearable burden for a long time. There are also 5 types of them:
| Group representatives | Mechanism of action |
| Rauwolfia preparations: Raunatin, Rauvazan, Reserpine | They demonstrate a pronounced hypotensive effect and have a low cost. |
| Central α2 receptor agonists: Clonidine, Methyldopa, Moxonidine | They affect the central nervous system, reduce sympathetic hyperactivity, reducing blood pressure. Side effects include drowsiness and fatigue. |
| Direct-acting vasodilators: Nitroglycerin, Bendazole, Hydralazine, Nitrong, Milsidomin | Centrally acting drugs gently dilate blood vessels, reducing venous flow to the heart muscle, reducing oxygen deficiency in the myocardium, and increasing heart rate. They have many contraindications, so they are prescribed only by a doctor. |
| Antispasmodics: Dibazol, Euphylline, Theophylline | They act on the smooth muscles of blood vessels, reduce pressure, dilate them, reduce blood viscosity, and prevent thrombosis. |
| Combined: Tonorma, Ziak, Enap-N, Vazar-N, Kaptopress | They lower blood pressure in different ways, since they combine several antihypertensive drugs. |
Most often, these drugs are not recommended as independent therapy; they are an auxiliary arsenal that purposefully enhances the effect of the main drugs.
Choosing an antihypertensive drug for the treatment of arterial hypertension
O.D. OSTROUMOVA
, Doctor of Medical Sciences
professor, I.I.
KOPCHENOV , Candidate of Medical Sciences,
Department of Faculty Therapy and Occupational Diseases of Moscow State Medical University named after. A.I. Evdokimova The article presents modern approaches to the differentiated selection of antihypertensive drugs.
The advantages and limitations of the main 5 classes of antihypertensive medications are described. Data are provided on the choice of drug within a class, taking into account specific clinical situations. The main goal of treatment for patients with arterial hypertension (AH) is to minimize the risk of developing cardiovascular complications (CVC) and death from them [1]. To achieve this goal, it is necessary not only to reduce blood pressure (BP) to the target level, but also to correct all modifiable risk factors (smoking, dyslipidemia, hyperglycemia, obesity), prevention, slow the rate of progression and/or reduce target organ damage (TOD) , as well as treatment of associated and concomitant diseases (coronary artery disease, diabetes mellitus, etc.).
The target blood pressure level is considered to be not exceeding 140/90 mmHg. Art. If the prescribed therapy is well tolerated, it is recommended to reduce blood pressure to lower values. In patients with a high and very high risk of cardiovascular disease, it is necessary to maintain blood pressure at 140/90 mmHg. Art. and below for 4 weeks [1]. In the future, subject to good tolerance, it is recommended to reduce blood pressure to 130–139/80–89 mmHg. Art.
Currently, 5 main classes of antihypertensive drugs (AGDs) are used for the treatment of hypertension: angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II AT1 receptor blockers (ARBs), calcium antagonists (CAs), beta-blockers (BABs) and diuretics [1 ]. Alpha-adrenergic blockers (AABs), imidazoline receptor agonists, and direct renin inhibitors can be used as additional drugs in combination therapy [1].
The choice of drug is influenced by a number of factors, the most important of which are [1]:
• the patient has other risk factors; • POM; • associated clinical conditions (ACS), kidney damage, metabolic syndrome (MS), diabetes mellitus; • concomitant diseases for which it is necessary to prescribe or limit the use of antihypertensive drugs of various classes; • history of individual drug intolerance; • the likelihood of drug interactions with drugs prescribed to the patient for other diseases; • socio-economic factors, including the cost of treatment.
When choosing an antihypertensive, it is necessary first of all to evaluate its effectiveness, the likelihood of side effects and the benefits of the drug in a certain clinical situation (Fig. 1 and 2). According to the results of multicenter randomized trials, none of the main classes of antihypertensive drugs has a significant advantage either in lowering blood pressure or in reducing the risk of cardiovascular events and death from them. A more significant factor in reducing the risk of cardiovascular events during antihypertensive therapy is the amount by which blood pressure decreases, so it is impossible to accurately predict which antihypertensive agent will be most effective in a given patient. Each of the representatives of the main classes of AGP has its own pros and cons (Fig. 1 and 2), so a universal ranking of AGP does not seem necessary. In each specific clinical situation, it is necessary to take into account the peculiarities of the action of antihypertensive drugs of various classes, identified in randomized trials [1]. Thus, the choice of a particular antihypertensive, especially at the start of treatment, should be based on the results of large clinical studies that have proven the high effectiveness and safety of using this particular drug in patients in a similar clinical situation [1].
ACE inhibitors
According to Russian pharmacoepidemiological studies, ACEIs are the most prescribed class of drugs for the treatment of cardiovascular diseases, including hypertension, due to the important role of activation of the renin-angiotensin-aldosterone system (RAAS) in the pathogenesis of these conditions [1].
Depending on the chemical structure of the active part of the molecule that binds to ACE, drugs of this class are divided into 3 groups [2]:
• ACE inhibitors containing a sulfhydryl group (captopril); • ACE inhibitors containing a carboxyl group or carboxyl dipeptides (enalapril, lisinopril, ramipril, perindopril, cilazapril, benazepril, quinapril, trandolapril, spirapril); • ACE inhibitors containing a phosphoryl group (fosinopril).
The effectiveness of therapy is significantly influenced by such parameters of the pharmacokinetics of ACE inhibitors as bioavailability, biotransformation (whether the drug is an active substance or a prodrug that is converted into active metabolites in the body), elimination routes and the duration of inhibition of ACE activity. Based on this, ACE inhibitors are divided into 2 groups according to their pharmacokinetic properties:
• active substances (captopril, lisinopril); • prodrugs: precursors of ACE inhibitors (fosinopril, all carboxyl dipeptides except lisinopril). Prodrugs are converted to their active form by hydrolysis of the ester linkage as they pass through the gastrointestinal mucosa and in the liver (for example, enalapril is converted to enalaprilat). The action of drugs in this group is realized more slowly, and the effect lasts longer. If liver function is impaired (liver cirrhosis, severe hepatitis, etc.), their effectiveness decreases, which requires dose adjustment [2].
Among the drugs in this group, fosinopril occupies a special place. A special feature of the drug is a dual balanced route of elimination - through the liver and through the kidneys (in a ratio of approximately 50:50). This means that in patients with impaired liver function, this fosinopril will be excreted through the kidneys, and in patients with impaired renal function, through the liver (gastrointestinal tract) [2]. In clinical practice, this provides the advantage of the drug, which is expressed in the absence of the need for dose adjustment in patients with concomitant renal or liver failure [2].
ACE inhibitors have proven effective in reducing the rate of progression of POM and reducing the degree of pathological changes. ACEI therapy leads to a decrease in the severity of left ventricular myocardial hypertrophy (LVMH), including the fibrous component, a significant decrease in the level of microalbuminuria (MAU) and proteinuria, and prevents deterioration of renal function [1]. The most pronounced antihypertensive effect of ACE inhibitors was observed in patients with increased activity of the RAAS [1,2]. In addition, ACE inhibitors slow down the degradation of bradykinin, which, on the one hand, enhances their antihypertensive effectiveness, and on the other hand, contributes to the development of such characteristic side effects as dry cough and angioedema.
As is known, in patients with diabetes, hypertension greatly increases the risk of developing both macrovascular (myocardial infarction, stroke) and microvascular (angiopathy, retinopathy, nephropathy) complications. It was found that ACE inhibitors have additional advantages for this group of patients compared to other classes of antihypertensive drugs: they largely reduce the risk of all complications and inhibit the development of chronic renal failure (CRF), i.e., they have a nephroprotective effect [1]. The use of ACE inhibitors significantly slows down the onset of “renal death” (dialysis or kidney transplantation) both in diabetic nephropathy and in hypertension with proteinuria without diabetes [3]. That is why they are indicated for all patients with a combination of diabetes and hypertension, as well as for patients with hypertension and microalbuminuria without diabetes [1].
A reliable clinical marker of an increased risk of complications, both cardiovascular and renal, in patients with hypertension, especially in combination with diabetes, is microalbuminuria [1]. By the degree of reduction of microalbuminuria during treatment, one can judge the reduction in the risk of complications. The effectiveness of ACE inhibitors in patients with microalbuminuria is due to the fact that angiotensin II plays a key role in the development of organ damage in hypertension, especially nephropathy and chronic renal failure. Angiotensin II stimulates the activity of the sympathetic nervous system, which entails an increase in the production of angiotensin II by the kidneys, activation of the RAAS, triggering a cascade of neurohumoral and structural-functional changes that lead to the development of proteinuria, cell proliferation, matrix accumulation and ultimately the formation of glomerulosclerosis [3 ].
The ACE inhibitor lisinopril has been found to reduce the level of microalbuminuria by 48% [4]. In addition, in patients with hypertension and diabetes, lisinopril has a number of additional positive effects on carbohydrate metabolism, in particular, it reduces the level of glycosylated hemoglobin and increases tissue sensitivity to insulin [5].
Of interest are the results of a study examining the effect of another ACE inhibitor, fosinopril, on the risk of micro- and macrovascular complications.
In the PREVEND-IT study (n = 864), it was proven that therapy with another ACE inhibitor, fosinopril, prevents the progression of microalbuminuria, as well as the development of cardiovascular complications in patients with hypertension [6, 7]. During therapy with fosinopril at a dose of 20 mg/day for 46 months in patients with hypertension and microalbuminuria, the level of urinary albumin excretion decreased by 26% compared with placebo, and the main combined indicator of cardiovascular mortality and hospitalization for heart disease was - by 40%. The use of pravastatin in this category of patients did not affect the level of microalbuminuria, and the rate of cardiovascular mortality and hospitalization decreased by 13% [6, 7].
One of the current problems is the treatment of hypertension in patients with MS. As is known, abdominal obesity is an independent risk factor for the development of complications in patients with hypertension [1, 8]. It has been established that in middle-aged patients with excess body weight, the risk of developing hypertension increases by 3 times, and in young people - by 6 times. According to the Framingham study, every 4.5 kg of excess weight increases systolic blood pressure in men by 4.4 mmHg. Art., and in women by 4.2 mm Hg. Art. Treatment of such patients poses certain difficulties [8].
According to the TROPHY study, the number of patients in whom it was possible to achieve normalization of blood pressure was significantly greater in the lisinopril group compared with the hydrochlorothiazide group (when using the drug in doses of up to 50 mg/day) [9]. At the same time, the level of glucose in the blood serum decreased in the lisinopril group, and increased in the hydrochlorothiazide group. The potassium level in the lisinopril group remained virtually unchanged, whereas in the hydrochlorothiazide group it decreased significantly. These properties convincingly demonstrate the feasibility of using lisinopril in obese patients with hypertension.
Another important property of ICE is its antiatherosclerotic effect. Thus, the results of the PHYLLIS study [10] showed a slowdown in the progression of atherosclerosis of the carotid arteries in patients with hypertension during therapy with fosinopril. The study involved 508 patients with hypertension and asymptomatic atherosclerotic lesions of the carotid arteries. Patients were divided into groups depending on the therapy: 127 patients received hydrochlorothiazide at a dose of 25 mg/day, 127 - fosinopril at a dose of 20 mg/day, 126 - 25 mg of hydrochlorothiazide and an additional 40 mg of pravastatin, 128 - 20 mg of fosinopril and 40 mg pravastatin. The average follow-up period was 2.6 years [12, 13]. The level of blood pressure achieved during treatment when measured in the clinic and on an outpatient basis in patients did not differ between groups. Intima-media thickness (IMT) significantly increased in the group of patients receiving only hydrochlorothiazide. In groups of patients taking fosinopril, a significant decrease in IMT thickness was observed [10]. Thus, it has been shown that fosinopril has an antiatherogenic effect in patients with hypertension.
Angiotensin II receptor blockers
There are two mechanisms in the action of angiotensin II (AII) on blood vessels: pressor and depressor. The first is mediated by the effect of AII on type 1 receptors and leads to vasoconstriction, sodium and fluid retention, increased sympathetic activity, decreased vagal tone, cell proliferation and a positive inotropic effect. The depressor effect of AII is realized through stimulation of type 2 receptors, which leads to vasodilation, especially pronounced in the vessels of the brain and kidneys, natriuretic effect, antiproliferative effect, activation of kininogen, release of nitric oxide and prostaglandin I2 [1, 2]. The antihypertensive effect and other pharmacological effects of AT1 receptor blockers (ARBs, sartans) are based on two mechanisms - direct and indirect. The first is associated with a weakening of the effects of AII under conditions of selective blockade of AT1 receptors. The second is due to reactive hyperactivation of the RAAS under conditions of blockade of AT1 receptors and additional stimulation of AT2 receptors [1, 2]. The antihypertensive effectiveness of ARBs is not influenced by the activity of the RAAS, gender and age of the patient.
ARBs have been proven to have a positive effect on the condition of target organs and reduce the risk of developing all cardiovascular complications [1, 2]. In addition, drugs in this group are characterized by the highest patient adherence to treatment due to high efficiency and the best treatment tolerability among all classes of antihypertensive drugs [1, 2]. In recent years, the scope of application of ARBs has expanded significantly. IHD, nondiabetic nephropathy, left ventricular dysfunction were added to the list of indications (diabetic nephropathy, proteinuria/MAU, chronic heart failure, LVMH, paroxysmal atrial fibrillation, cough while taking ACE inhibitors, etc.); In addition, ARBs can now be prescribed to older patients [1].
The first and extremely important study confirming the enormous potential of sartans in the treatment of hypertension was the LIFE study (Losartan Intervention For Endpoint reduction in hypertension study) [11]. More than 9,000 patients with hypertension and LVMH took part in it. Patients received either losartan 50 mg or atenolol 50 mg, with the option of adding 12.5 mg hydrochlorothiazide and subsequently increasing the dose of the drugs until the target blood pressure level was achieved. During the 5-year follow-up, patients receiving losartan, compared with the atenolol group, had a 13% reduction in the incidence of major cardiovascular events (primary endpoint), including a 25% difference in the incidence of strokes. Of course, the main mechanism for this effectiveness of losartan is its ability to reduce the severity of LVMH (p < 0.0001 for the Sokolow-Lyon index and for the Cornell product) [11]. It is known that LV hypertrophy is an independent serious risk factor for cardiovascular events [1]. The same study demonstrated a decrease in the incidence of new cases of type 2 diabetes (by 25%) and a decrease in the severity of insulin resistance when treated with losartan [11].
It is worth noting that among all ARBs, only losartan with proven effectiveness significantly increases uric acid excretion (up to 300%), which makes its use attractive in patients with gout [13]. As is known, hyperuricemia is one of the components of metabolic syndrome and an independent risk factor for CVD. The experiment showed that losartan has the ability to block the transport of urate through membranes in the proximal renal tubules [2]. Thus, ARBs reduce the risk of developing diabetes mellitus, making their use especially relevant in patients with hypertension and MS [1].
ARBs are also characterized by a pronounced nephroprotective effect, which was proven by the results of the large RENAAL study (n = 1,513), which assessed the effectiveness of losartan in patients with hypertension, type 2 diabetes mellitus and diabetic nephropathy. As a result of taking losartan (50–100 mg/day), the risk of a double increase in plasma creatinine concentration was reduced by 25%, and the risk of developing end-stage chronic renal failure was reduced by 28%. In addition, compared with the placebo group, patients in the losartan group had a statistically significant reduction in the level of proteinuria and the frequency of initial hospitalization [12].
Thus, ARBs have established themselves as indispensable drugs in the treatment of such a socially significant disease as hypertension. Their effect is multifaceted and is determined not only by the effect on blood pressure, but also by the normalization of the functioning of the RAAS and the organoprotective effect; The drugs have a favorable metabolic profile and an extremely low incidence of side effects.
Calcium antagonists
The effectiveness of AKs as antihypertensive agents is due to a slowdown in Ca current through the α1- and α2-adrenergic pathways and calcium channels of peripheral vessels, a decrease in the sensitivity of arterial vessels to the endogenous influences of norepinephrine, vasopressin, histamine, serotonin, acetylcholine, which leads to a decrease in total peripheral vascular resistance and BP [1, 2, 14]. AAs are divided into 3 subgroups depending on the chemical structure [1, 2, 14]:
1) dihydropyridines (nifedipine, amlodipine, felodipine, etc.); 2) phenylalkylamines (verapamil); 3) benzodipines (diltiazem).
There are significant differences in the ability of AA to affect the myocardium, vascular wall and cardiac conduction system. Dihydropyridines have a pronounced selective effect on the vascular muscles, leading to dilation of peripheral arteries, do not affect the conduction system of the heart and practically do not cause a decrease in the contractile function of the myocardium [1, 2, 14]. Non-dihydropyridine AKs (verapamil and diltiazem) are characterized by negative ino- and dromotropic effects. All AAs are metabolically neutral and do not have a negative effect on carbohydrate, lipid and purine metabolism. In addition to the antihypertensive effect, ACs have organoprotective and antianginal properties, inhibit platelet aggregation, significantly reduce the risk of stroke, and are the first choice drugs in elderly patients and patients with isolated systolic hypertension [1, 2, 14].
The most important characteristic of AKs is their ability to inhibit the progression of atherosclerosis [14]. The mechanisms of the anti-atherosclerotic effect are to slow down the proliferation of smooth muscle cells by suppressing the release of the corresponding growth factor, inhibiting vascular intimal hyperplasia, reducing the adhesion of monocytes and the uptake of cholesterol esters by macrophages, inhibiting the expression of the HMG-CoA reductase gene, a beneficial effect on the HDL/LDL ratio, stabilization of the plasma membrane , which prevents the penetration of free cholesterol into the vessel wall, and the antioxidant effect of AA [14]. The prospective, randomized, double-blind study of the vascular effects of amlodipine (PREVENT) assessed the effect of the drug on the progression of early atherosclerosis [15]. The results of treatment with amlodipine besilate 10 mg once daily were compared with the effect of usual therapy (clinicians were allowed to use any drugs or interventions they considered necessary). The study involved 825 patients; the follow-up period was 3 years. The primary end point was the dynamics of the condition of the coronary arteries with initial atherosclerotic changes (initial stenosis 30%), which was assessed using quantitative coronary angiography (QCA). Other endpoints included the dynamics of changes in the diameter of segments of coronary arteries affected by atherosclerosis according to CCA data, the rate of progression of carotid atherosclerosis, which was determined using two-dimensional echography, and clinical outcomes. Amlodipine was prescribed at a dose of 5 mg/day, then increased to 10 mg/day for 4 weeks. The study included patients aged 30–80 years with a left ventricular ejection fraction of 40% or more.
Ultrasound examination of the carotid arteries showed that in patients with coronary atherosclerosis, long-term therapy with amlodipine significantly slows down the progression of carotid atherosclerosis [15]. Measurements in 12 carotid artery segments were taken before treatment, at the end of the 4-week dose titration period, and at 6, 12, 24, 30, and 36 months (final visit). In patients receiving amlodipine, the thickness of the intima-media complex decreased by 0.013 mm over 3 years, and in the placebo group it increased by 0.033 mm (p = 0.007).
In the PREVENT study, 3 years of amlodipine therapy led to a significant reduction in the incidence of adverse clinical outcomes in patients with coronary atherosclerosis. With long-term treatment with amlodipine, the incidence of hospitalization for unstable angina and congestive heart failure decreased by 35% compared with that in the placebo group (p = 0.01). The incidence of coronary artery surgery in the amlodipine group decreased by 43% compared with that in the placebo group (p = 0.001) [15]. After 36 months, amlodipine therapy led to a reduction in the total incidence of any CV events or interventions on the coronary arteries by 31% (p = 0.01), mainly due to a significant reduction (by 33%) in the frequency of hospitalizations for unstable angina and surgical interventions on the coronary arteries arteries (by 43%) [15].
AKs are indicated for a combination of hypertension and coronary artery disease [1]. In these patients, third-generation dihydropyridine AKs (primarily amlodipine) are indicated in the following situations [1, 14]:
• as first-line drugs for variant angina; • in patients with angina pectoris in case of persistent angina attacks during therapy with beta blockers, their combination with prolonged dihydropyridines is indicated.
It should be noted that retrospective case-control studies have shown that the relative risk of developing cardiovascular events or death in patients with hypertension when treated with short-acting nifedipine is significantly higher than when treated with diuretics or beta blockers [14]. At the same time, the use of long-acting dihydropyridines does not lead to an increase in the risk of myocardial infarction compared with that when using diuretics, beta blockers, ACEIs and ARBs [14]. Therefore, in clinical practice, the use of prolonged dihydropyridine AA (IIb and especially III generation) is preferable.
Thiazide and thiazide-like diuretics
Thiazide and thiazide-like diuretics (TD) have a pronounced antihypertensive effect. The effectiveness of TD treatment in lowering blood pressure and reducing cardiovascular mortality has been proven in numerous controlled comparative randomized studies, as well as the results of meta-analyses [1].
TDs act on the cortical segment of the loop of Henle and in the initial region of the distal tubules, where in healthy people up to 5–8% of filtered sodium is reabsorbed, they inhibit the activity of a special sodium-chlorine transporter and promote increased excretion of sodium and chlorine ions, as well as water and potassium ions and magnesium [2].
Due to the direct and indirect vasodilating effect of diuretics, a decrease in blood pressure, a decrease in total peripheral vascular resistance, and a decrease in venous return to the heart are noted. The action of thiazide and thiazide-like diuretics begins 1-2 hours after oral administration and lasts for 12-24 hours in most patients (24 hours for the thiazide-like diuretic indapamide).
It should be noted that most TDs are characterized by unfavorable metabolic effects. Treatment with high doses of TD (hydrochlorothiazide 50–100 mg/day) can worsen carbohydrate, lipid, and purine metabolism and reduce the amount of potassium in the blood plasma [1]. This circumstance limits the use of drugs of this group in patients with MS and a high risk of diabetes mellitus. The drug of choice in such cases is the thiazide-like diuretic indapamide: it is metabolically neutral and does not have a negative effect on carbohydrate and lipid metabolism [2].
Indapamide occupies a special place in the group of diuretics. The therapeutic effectiveness of the drug is due to its dual action. Firstly, it inhibits the reabsorption of sodium, chlorine, and, to a lesser extent, potassium and magnesium ions in the proximal and distal tubules of the short segment of the nephron; secondly, it eliminates the excess content of sodium ions in the vascular wall, increases the synthesis of prostaglandin E2 and J2, inhibits the influx of calcium ions into the smooth muscle cells of the vascular wall, resulting in vasodilatation and a decrease in their sensitivity to vasopressor agents (catecholamines, thromboxane) [2 , 16, 17]. Indapamide has a diuretic effect when using a dose of 5 mg/day, daily diuresis increases by 20%. At doses of 1.25–2.5 mg/day, the drug acts primarily as a peripheral arterial vasodilator. Moreover, the antihypertensive effectiveness of indapamide at a dose of 2.5 mg/day is comparable to the effect of 20 mg/day enalapril or 5 mg/day amlodipine [3, 9].
Total peripheral vascular resistance during treatment with indapamide 2.5 mg/day is reduced by 10–15%. According to 24-hour Holter blood pressure monitoring, during treatment with indapamide, there is a uniform decrease in blood pressure throughout the day, without a rise in the early morning hours [1]. The drug is effective for normal and impaired renal function.
The antihypertensive effect of indapamide is observed in mild hypertension in approximately 70% of patients. The effect appears after a few days of treatment and gradually increases. With long-term therapy, the antihypertensive effect of this drug remains in 60% of patients [2, 16].
A unique property of indapamide as a diuretic is its positive effect on lipid metabolism. Thus, it was noted that during treatment with indapamide, the level of low-density lipoprotein cholesterol and triglycerides decreases and the level of high-density lipoprotein cholesterol increases [16].
In addition to the antihypertensive effect, indapamide helps reduce left ventricular hypertrophy in patients with hypertension. Six-month therapy with indapamide 2.5 mg/day resulted in a decrease in left ventricular mass index by 13.3% [16].
Unlike thiazide diuretics, indapamide has a nephroprotective effect. Long-term (for 2 years) treatment with this drug in patients with hypertension and functional renal failure was accompanied by an increase in glomerular filtration rate by 28% [16]. Thus, among thiazide diuretics, indapamide is the drug of choice for the treatment of patients with hypertension and dyslipoproteinemia, MS, diabetes mellitus and early renal failure.
Beta blockers
BABs have been proven to be highly effective in reducing the risk of CV events in the treatment of patients with hypertension [1]. Currently, indications for prescribing beta blockers in patients with hypertension are stable angina, previous myocardial infarction, chronic heart failure, tachyarrhythmia, glaucoma and pregnancy.
BBs compete with catecholamines for binding to beta-adrenergic receptors of the heart. The main effects of beta blockers - a decrease in the frequency and strength of heart contractions, antiarrhythmic and hypotensive effects - are due to blocking the influence of mediators on beta1-adrenergic receptors.
The problem that arises when using beta blockers is the unfavorable metabolic effect of a number of representatives of this class on carbohydrate and lipid metabolism, which limits their use as monotherapy in people with MS and a high risk of developing diabetes mellitus. It is worth emphasizing that data on the negative metabolic effects of beta blockers were obtained from the analysis of studies in which atenolol was mainly used. These restrictions do not apply to highly selective blockers (bisoprolol, nebivolol), as well as the third generation drug carvedilol, which, in addition to a pronounced vasodilating effect, also has a cardioprotective effect due to its antioxidant properties [1].
Thus, a differentiated approach to the selection of a class of antihypertensive drugs and a drug within a class will allow individualizing the treatment of a particular patient and increasing its effectiveness.
Literature
1. Diagnosis and treatment of arterial hypertension. Russian recommendations (fourth revision). Systemic Hypertension 2010; 3:5–26. 2. Clinical pharmacology. Ed. V.G. Kukesa, edition 4, M.: “GEOTAR-Media”, 2008. pp. 321–396, 458–479. 3. Rizzoni D., Muiesan ML, Porteri E. Effects of long-term antihypertensive treatment with lisinopril on resistance arteries in hypertensive patients with left ventricular hypertrophy. J. Hypertens., 1997; 15 (2): 197-204. 4. Balázsi I., Takács J. The effect of lisinopril on hypertensive patients suffering in diabetic nephropathy Diabetologia Hungarica, 1999; 7.(N2.): 101-106. 5. Kawahara J., Hsieh ST., Tanaka S. et al. Effects of lisinopril on lipid peroxidation, cell membrane fatty acids, and insulin sensitivity in essential hypertension with impaired glucose tolerance. Am J Hypertens 1994; 7:23A. 6. Asselbergs FW, Diercks GFH, Hillege HL et al. for the Prevention of Renal and Vascular Endstage Disease Interventional Trial (PREVEND IT) Investigators. Effect of fosinopril and pravastatin on cardiovascular events in subjects with microalbuminuria // Circulation. – 2004. – Vol. 110. – P. 2809-2816. 7. Diercks GF, Janssen WM, van Boven AJ et al. Rationale, design, and baseline characteristics of a trial of prevention of cardiovascular and renal disease with fosinopril and pravastatin in nonhypertensive, nonhypercholesterolemic subjects with microalbuminuria (the Prevention of REnal and Vascular ENDstage Disease Intervention Trial) // Amer. J. Cardiology. – 2000. – Vol. 86. – P. 635-638. 8. Chazova I.E., Mychka V.B. Metabolic syndrome. M.: Media Medica, 2004. – 163c. 9. Reisin E. TROPHY study. Hypertens. 1997; 30: P.140-145. 10. Zancetti A., Crepaldi G., Bond G. et al. on behalf of PHYLLYS Investigators. Different effects of antihypertensive regimens based on fosinopril or hydrochlorthiazide with or without lipid lowering with pravastatin on progression of asymptomatic carotid atherosclerosis. Princioal results of PHYLLIS – a randomized double-blind trial // Stroke. – 2004. – Vol. 35. – P. 2807-2812. 11. Dahlof B, Devereux RB, Kjeldsen SE, et al. Cardiovascular morbidity and mortality in the Losartan Intervention for Endpoint reduction in hypertension study (LIFE): a randomized trial against atenolol. //Lancet.– 2002– 359(9311) – P. 995–1003. 12. Brenner B.M., Cooper M.E., de Zeeuw D., Grunfeld J.–P., Keane W.F., Kurokawa K., McGill J.B., Mitch WE., Parving H.H., Remuzzi G., Ribeiro A.B., Schluchter M.D., Snavely D., Zhang Z, Simpson R, Ramjit D, Shahinfar S: Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan (RENAAL). JRAAS 2000;1:328–35. 13. Dang A., Zhang Y., Liu G. et al: Effects of losartan and irbesartan on serum uric acid in hypertensive patients with hyperuricaemia in Chinese population. J hum Hypertense 2006; 20:45–49. 14. Kukes V.G., Ostroumova O.D., Starodubtsev A.K. Calcium antagonists: modern aspects of application in cardiology. Consilium medicum, 2006; Vol. 8 (No. 11): 113–117. 15. Pitt B, Byington RP, Furberg CD et al. (for the PREVENT investigators). Effect of amlodipine on progression of atherosclerosis and the occurrence of clinical events. Circulation 2000; 102(13):1503–10. 16. Preobrazhensky D.V., Sidorenko B.A. Differential drug therapy for arterial hypertension. Consilium Medicum. 2001; Volume 3 (10): 83–87. 17. Passeron J., Panly N., Despart J. International multicentre study of indapamide in the treatment of essential arterial hypertension. Postgrad. Med. J., 1981; 57:53–64.
List of fast and long-acting drugs
The increase in pressure can be spontaneous, sudden or gradual, but steady. This requires the use of rapid or long-acting antihypertensive drugs.
Fast acting drugs:
- Lasix (Furosemide) is a loop diuretic, the drug of choice for emergency care, corrects electrolyte metabolism, causes frequent urination, tablets are effective within an hour, injectable within the first 20 minutes;
- Atenolol (Anaprilin, Sotagestal) - slows down the heart rate while leveling blood pressure, acts after 15 minutes;
- Adelfan - antihypertensive tablets under the tongue, effective in 10 minutes;
- Clonidine – the effect is observed after half an hour, minus – dryness of the mucous membranes;
- Nifedipine – begins to work 5 minutes after sublingual administration;
- Captopril - under the tongue, works in 20 minutes, minus - three times a day.
- Nitroglycerin has a hypotensive effect after 5 minutes, prevents vasospasm, leading to heart attacks.
These antihypertensive drugs are indicated for the relief of hypertensive crises. Complicated crises require injection therapy.
The prolonged group was developed for the convenience of treating hypertension; lifelong use of drugs once or twice a day does not interfere with leading a normal lifestyle:
- Sotalol, Propranol, Carvedilol - non-selective beta receptor blockers;
- Atenolol, Bisoprolol, Betaxol - selective beta blockers;
- Amlodipine, Verapamil, Diltiazem – calcium antagonists;
- Enalapril, Lisinopril, Perindopril – ACE inhibitors;
- Indapamide, Hydrochlorothiazide, Hypothiazide are diuretics.
These drugs are used in the combination treatment of second or third degree hypertension.
Valid combinations
The compatibility of antihypertensive drugs is necessary in the treatment of high blood pressure. The most commonly used combinations are presented in the table:
| Combination of drugs | Possible applications |
| Beta blockers + diuretics | High blood pressure, uncomplicated hypertensive crisis, hypertension without target organ damage |
| Diuretics + ACE inhibitors | Hypertension resistant to therapy, chronic heart failure (CHF) |
| Diuretics + angiotensin 1 receptor blockers | Isolated systolic hypertension (ISAH), CHF |
| Diuretics + imidazoline II receptor agonists | If beta blockers are contraindicated, but there is a need to add similar agents to the diuretic |
| Diuretics + calcium antagonists | CHF with a sharp rise in pressure, in elderly patients with ISAH |
| Alpha and beta blockers together | Malignant hypertension |
| Beta blockers + ACE inhibitors | Post-infarction condition, secondary prevention, patients with coronary heart disease (CHD), CHF |
| Beta blockers + calcium antagonists | Arterial hypertension (AH), ischemic heart disease |
| Calcium antagonists + ACE inhibitors | Hypertension, nephropathy in the initial stage, ischemic heart disease, signs of atherosclerosis |
| Calcium antagonists + angiotensin 1 receptor blockers | High blood pressure, nephropathy, progressive atherosclerosis |
The effectiveness of any combination of antihypertensive drugs depends on the presence of certain indications, taking into account the metabolic and hemodynamic properties of each component.
Features of the treatment of hypertension in the elderly
Antihypertensive drugs must be taken when the systolic value exceeds 160 mm Hg. Art. Fluctuations in the upper values from 140 to 160 are called the “gray zone”.
Older people need to take medications to lower blood pressure for life. Doctors try to select antihypertensive drugs with few or no side effects.
If the patient has a history of diabetes mellitus, a heart attack, stroke, or other severe conditions, the selection of antihypertensive drugs is carried out with extreme caution.
For convenience, modern long-acting antihypertensive drugs are selected, which can be taken once a day.
At the beginning of therapy, the patient is prescribed half the standard dose, gradually increasing it. This measure is necessary for the body to adapt to changes.
The medicinal product must have convenient packaging. Otherwise, patients suffering from visual impairment and arthritis may find it difficult to open the package, so they may not take the pill on time.
Ignoring arterial hypertension is dangerous for patients of any age, but especially the elderly. Chronic increase in pressure causes additional stress on the heart, vascular and renal systems, as a result of which a hypertensive crisis may occur, accompanied by serious consequences: heart attack, stroke, impaired renal function, pulmonary edema. This increases the risk of patient disability and even death.
In addition to drug therapy, the patient must reconsider his usual lifestyle. It is necessary to eliminate factors that provoke increased blood pressure: physical inactivity, alcohol, smoking, junk food, etc.
Side effects
The negative consequences of taking antihypertensive drugs vary across groups. The main ones are presented in a table:
| Group, individual representatives | Side effects |
| Diuretics - reduce blood pressure, enhancing the effect of other antihypertensive drugs | |
| Thiazides have an average degree of activity: Hydrochlorothiazide, Cyclopenthiazide, Chlorthalidone | Complications after taking:
|
| Loop diuretics - the strongest: Lasix, Furosemide, Indapamide | Call:
|
| Potassium-sparing - weak diuretics: Veroshpiron, Spironolactone, Amiloride, Triamtren | The most dangerous side effect is hyperkalemia, which is life-threatening; other complications are similar to other diuretics |
| Drugs that block the sympathoadrenal system | |
| Centrally acting drugs (virtually irrelevant in modern therapy, with the exception of natural remedies indicated for pregnant women): Methyldopa, Clonidine, Guanfacine, Moxonidine, Reserpine | Most of the negative consequences are associated with the central nervous system: drowsiness, fatigue, apathy; with abrupt withdrawal, there may be rebound syndrome: migraine, anxiety, arrhythmias, abdominal pain |
| Beta blockers: Betaloc, Propranolol, Atenolol, Metoprolol, Bisoprolol, Betaxolol, Nebivolol | There are three big problems associated with these antihypertensive drugs:
|
| Alpha blockers: Prazosin, Terazosin, Doxazosin | They increase the risk:
|
| Mixed type blockers: Labetalol, Carvedilol | Shows type 1 and type 2 side effects |
| Calcium antagonists | |
| Antihypertensive drugs such as dihydropyridines: Nimodipine, Nifedipine, Amlodipine, Felodipine | Cause symptoms associated with excessive expansion of the lumen of the arteries:
They go away on their own and do not require treatment. |
| Phenylamines: Verapamil | Provoke:
|
| Benzodipines: Diltiazem | May lead to bradycardia, sinus node block |
| ACE inhibitors (angiotensin-converting enzyme) | |
| Representatives: Captopril, Enalapril, Fosinopril, Lisinopril, Ramipril, Perindopril | Side effects:
|
| Angiotensin II receptor blockers (ARBs, sartans) | |
| Representatives: Losartan, Valsartan, Candesartan, Telmisartan | They are best tolerated among antihypertensive drugs and are considered the drugs of choice in the treatment of nephrotoxic hypertension. Overdose can cause orthostatic hypotension, contraindicated in pregnant women |
The latest generation of antihypertensive drugs listed in the table have a minimum number of side effects - this is a trend in modern pharmacological practice.