How to prevent a stroke?
05.08.2019
«
Companion
»
Scientist Dmitry Napalkov: seven rules help prevent stroke
Dmitry Napalkov, professor of the department of faculty therapy No. 1 of the medical faculty of the First Moscow State Medical University named after I.M. Sechenov, spoke to the Sobesednik publication about measures to prevent stroke
Every year, about 12 million cases of stroke are recorded worldwide. In Russia, someone has a stroke every minute and a half. This insidious disease can happen to anyone, regardless of age or genetics. When this happens to a loved one or an acquaintance, we grab our heads: well, surely everything could have been prevented? Can! Only for this you need to comply with several important conditions. One of my friends had a stroke while he was on a business trip. I worked all day long without rest. I had a sharp headache, my mind was so clouded that I couldn’t even speak two sentences. Colleagues did not immediately call an ambulance. They gave me some kind of pill: “Just lie down, everything will pass.” After a couple of hours, the situation worsened so much that only intensive care was able to pump out my friend.
Doctor of Medical Sciences, Professor of the Department of Faculty Therapy No. 1 of the Faculty of Medicine of the First Moscow State Medical University named after I.M. Sechenov Dmitry Napalkov to our question - how to prevent a stroke? – answered this:
– Everyone wants to prevent themselves from having a stroke, but few people do anything about it. Cardiovascular diseases depend mainly on lifestyle. Lack of physical activity, unhealthy diet, and bad habits are very serious risk factors. However, with serious disturbances in the functioning of the heart and blood vessels, nutrition and exercise alone will not help. You must take medications as prescribed by your doctor. And be very careful! For example, a well-known anticoagulant (vitamin K antagonist), used to prevent stroke, imposes severe dietary restrictions: raspberries, green tea, green vegetables, cabbage, eggs and other foods rich in vitamin K are undesirable. However, science does not stand still, and a new generation of drugs has now been created - for example, based on direct thrombin inhibitors. They do not require dietary restrictions.
Do not neglect measures such as: reducing the amount of salt in the diet to 5 g per day (about half a teaspoon), avoiding foods high in cholesterol. Add fruits, vegetables, whole grains and low-fat dairy products to your daily diet, as well as one serving of fish two to three times a week. See a specialist regularly. It is important to consult not only a therapist, but also a neurologist. It is necessary to do an ultrasound of the neck vessels and receive a health card.
Monitor your blood pressure. Arterial hypertension increases the risk of stroke several times. Therefore, it is advisable to measure your blood pressure levels at least once a week. Even if you feel well and do not have symptoms of hypertension such as headaches, fatigue and sleep disturbances, an increase in resting pressure readings above 140/90 mm Hg. Art. – this is already a reason to see a doctor.
World practice shows that by controlling blood pressure alone, it is possible to reduce the risk of stroke by 50%.
Control your weight. Neurologists agree that weight loss is one of the most effective measures in preventing stroke. Excess body weight contributes to the development of high blood pressure, diabetes and puts increased strain on the heart muscle.
It is clear that we cannot reduce our weight without a proper diet. It is worth giving up fatty and heavy foods to reduce blood sugar and cholesterol levels. To get results, you must stick to the diet for at least 3-4 months.
Be active. Physical inactivity, or too low a level of physical activity, is the scourge of our time. Therefore, it is important to do physical exercise for more than 30 minutes at least 5 times a week.
Aerobic exercise is the best way to prevent stroke—repetitive exercise that increases the supply of oxygen to the body. Your doctor will choose the best exercise for you, taking into account your age and existing diseases.
Well, these rules are available to everyone: use the stairs instead of the elevator, better get off one stop early and walk, find time to walk during your lunch break.
Treat diabetes. Those who suffer from diabetes have a significantly increased risk of stroke. Patients with diabetes suffer strokes much more severely than others. This is because due to atherosclerosis, many arteries are unable to move oxygen. And alas, the prognosis for stroke in diabetes mellitus in most cases will be much worse.
Drink less alcohol. Until recently, the relationship between alcohol consumption and stroke remained in question, but today there is no doubt: alcohol significantly increases the risk of stroke.
Stop smoking. Smoking people have a stroke 2-3 times more often than non-smokers. Conclusion: the more you smoke, the higher your risk of stroke! In addition, the age of the smoker is of great importance: in men and women who smoke under the age of 55, smoking is the main risk factor for stroke.
Atherosclerosis develops in the damaged vascular wall (thickening of the wall and reduction of the lumen), and this increases the risk of blood clot formation in the vessels of the brain. Smoking affects the properties of special blood cells called platelets, resulting in an increased risk of blood clots in the large arteries that carry blood to the brain and heart. Smoking also increases blood pressure, which is one of the most important risk factors for stroke.
By the way! A study of thousands of patients over 35 years (Nurses' Health Study) showed that a typical European diet, including large amounts of meat, eggs, fried and salty foods, refined bread, full-fat dairy products, sweet desserts and chips, increases the risk of stroke by 58% . While eating whole grains, fruits, vegetables and fish reduces this risk by 30%.
Link to publication: /sobesednik.ru
The need for prevention
Meanwhile, many dangerous diseases can be prevented. Analyzing the chain of events that led to a heart attack or brain stroke, doctors and their patients are often convinced that the cause of the disease is a simple reluctance to take care of oneself, listen to one’s condition and give up bad habits. Even bitter experience turns out to be powerless here: having recovered from myocardial infarction, many patients continue to indulge their weaknesses, regardless of the recommendations of doctors. As a result, a relapse of the disease occurs, and possibly death.
Simple measures for the primary prevention of heart attack and stroke in old age do their job well. Conventionally, they can be divided into four groups:
- use of preventive medications;
- changing your daily routine and diet;
- treatment of systemic diseases that increase the likelihood of developing damage to the cardiovascular system, including diabetes;
- regular monitoring of the state of the circulatory system and maintaining it in good shape.
ALCOHOL
Alcohol abuse leads to an increased risk of hemorrhagic stroke (bleeding in the brain). Reduce the amount of alcohol you consume to a minimum.
OBESITY
Excess weight negatively affects the functioning of your heart and blood vessels. People who are overweight or obese often have high blood pressure and diabetes. These factors significantly increase the risk of developing a recurrent stroke. To reduce the risk, measures to correct body weight are necessary, which your doctor can suggest for you individually.
WHAT CAUSES TIA OR ISCHEMIC STROKE?
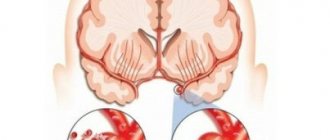
Blockage of a cerebral vessel by a thrombus, cutting off blood supply to a part of the brain, is the most common cause of stroke or transient ischemic attack. There are two ways of developing a brain catastrophe: the first is when a blood clot forms directly in a cerebral vessel (this is the so-called atherothrombotic stroke), and the second is when a blood clot forms elsewhere in the body, breaks off and is carried by the bloodstream into the brain, leading to a stroke (embolic stroke). ).
The most common signs of stroke
- Sudden weakness, numbness, paralysis of a part of the body: face, arms, legs, half of the body.
- A sudden, intense headache, sometimes described as the worst headache of your life.
- Sudden loss of vision clarity.
- Sudden speech impairment (inability to speak or understand someone else's speech)
- Sudden dizziness, loss of coordination, nausea, vomiting, and sometimes loss of consciousness.
Stroke may recur if effective prevention of this disease is not carried out. Unfortunately, people who have had a stroke or transient ischemic attack have a very high risk of developing another stroke. According to scientific research, a person who has had a stroke is 15 times more likely to have the event happen again compared to people who have not had a stroke. The condition of cerebral vessels affected by atherosclerosis and the predisposition of the blood coagulation system to the formation of intravascular thrombi cause these complications. It has been proven that the risk of recurrent stroke can reach 30% during the first year after the first event and decreases slightly in subsequent years. Your healthcare provider can determine how high your risk is for the event to happen again and take steps to reduce that risk.
EFFECTIVE PREVENTION OF REPEATED STROKE MUST INCLUDE THE SUCH DIRECTIONS
- Daily monitoring and effective treatment of high blood pressure. Your blood pressure should be 140/90 mmHg. Art., and for patients with concomitant diabetes mellitus 130 per 80 mm Hg. Art.
- It is mandatory to take medications that “thin” the blood (antiplatelet agents after atherothrombotic stroke and anticoagulants after embolic stroke), intended to prevent intravascular thrombus formation.
- Control and correction of cholesterol levels significantly influence the further progression of atherosclerosis. In patients with high cholesterol levels, it is mandatory to prescribe drugs that lower the level of cholesterol in the blood serum.
Please also pay attention to the following factors that significantly influence the development of a recurrent stroke:
Antiplatelet therapy
The effectiveness of the use of antiplatelet agents to prevent recurrent IS has been confirmed by many researchers. Four antiplatelet drugs have been shown to reduce the risk of recurrent IS after stroke or TIA.
The results of a meta-analysis of data from 287 studies, including 212 thousand patients with a high risk of occlusive vascular events, showed that against the background of antiplatelet therapy, the number of cases of non-fatal stroke decreased by an average of 25%, and vascular mortality - by 23%. Moreover, according to a meta-analysis of 21 randomized trials that compared antiplatelet therapy with placebo in 18,270 patients who had a stroke or TIA, antiplatelet therapy leads to a 28% relative risk reduction in nonfatal stroke and a 16% relative risk reduction in fatal stroke [ 10].
Acetylsalicylic acid
The clinical effectiveness of ASA for the secondary prevention of IS was first shown in 1977. Subsequently, numerous international placebo-controlled studies demonstrated that ASA at a dose of 50–1300 mg/day is effective in the prevention of recurrent IS or TIA [10, 15].
The first experience in world clinical practice of using small doses of ASA (1 mg/kg/day) in patients with cerebrovascular pathology due to hypertension, carried out at the Research Institute of Neurology of the Russian Academy of Medical Sciences, showed a rapid and persistent elimination of platelet hyperaggregability due to an almost 3-fold decrease in the initial concentration of thromboxane A2 in the blood regardless of the gender of patients and the type of ischemic cerebrovascular accident. The study included patients with TIA and post-IS [5].
Two large international controlled studies compared the effectiveness of different doses of ASA for patients with TIA or IS (1200 vs. 300 mg/day and 283 vs. 30 mg/day) [25, 40]. In both studies, high- and low-dose ASA was effective in preventing IS, but higher doses of ASA were associated with a higher risk of gastrointestinal bleeding [10].
When choosing the optimal daily dosage of ASA for the prevention and treatment of IS, its side effects play an important role. Like other non-steroidal anti-inflammatory drugs, ASA can have both local (due to irritation of the mucous membrane) and systemic (by reducing the synthesis of prostaglandins) damaging effects on the mucous membrane of the gastrointestinal tract (GIT) when taken orally, including. including the occurrence of erosions and ulcers, as well as the development of gastrointestinal bleeding. The frequency of this complication directly depends on the daily dose. Thus, the side effect of ASA on the gastrointestinal mucosa decreased when taking 300 mg/day compared with the use of higher (1200 mg/day) doses of ASA and amounted to 31 and 41%, respectively, for discomfort in the abdominal area, 3.1 and 4. 8% for gastrointestinal bleeding (UK-TIA Study Group, 1991) [25]. At the same time, the ESPS 2 (European Stroke Prevention Study 2) study showed that low doses of ASA do not completely eliminate its ability to induce bleeding [19].
To eliminate the adverse effect of ASA on the gastrointestinal mucosa, various dosage forms with an enteric coating have been proposed, for example thrombo ASA. Absorbed from the upper part of the small intestine, this drug causes local ulcerogenic effects to a much lesser extent.
Ticlopidine
The effectiveness of ticlopidine (thienopyridine) was assessed in three randomized trials in patients with cerebrovascular disease. The CATS (Canadian-American Ticlopidine Studi) trial compared the effectiveness of ticlopidine 250 mg/day with placebo in the prevention of stroke, MI, or death due to vascular pathology in 1053 patients with IS. Ticlopidine has been shown to lead to a 23% reduction in the relative risk of meeting the combined endpoint of the study [27]. The TASS (Ticlopidine Aspirin Stroke Study), which compared the effectiveness of ticlopidine (250 mg twice daily) and ASA (650 mg twice daily) in 3069 patients with a recent minor stroke or TIA [30], demonstrated a reduction in the relative risk of stroke. by 21% over a 3-year follow-up, as well as a slight (9%) reduction in the risk of end events (stroke, MI, death due to vascular pathology) when using ticlopidine.
The most common side effects of ticlopidine: diarrhea (approximately 12%), gastrointestinal symptoms, rash, hemorrhagic complications, are identical to those that occur when taking ASA. Neutropenia was observed in approximately 2% of patients receiving ticlopidine in the CATS and TASS studies. However, the incidence of particularly severe complications was less than 1%; in almost all cases they were reversible and disappeared when the drug was discontinued. In addition, thrombocytopenic purpura has been described.
Clopidogrel
The effectiveness of clopidogrel was assessed in comparison with ASA in the CAPRIE study (Clopidogrel Versus Aspirin in Patients at Risk of Ischemic Events, [14]). More than 19 thousand patients with stroke, MI or peripheral vascular disease were randomized to receive ASA at a dose of 325 mg/day or clopidogrel at a dose of 75 mg/day. The primary end event - IS, MI, death due to vascular pathology - occurred with a frequency of 8.7% lower in patients receiving clopidogrel compared to the ASA group.
Two studies [12, 36] indicated a relatively greater effectiveness of clopidogrel (compared to ASA) for patients with diabetes and patients who have already had an ischemic stroke or myocardial infarction. In general, clopidogrel is safer when taken compared to ASA and especially ticlopidine. Clopidogrel, like ticlopidine, was less likely to cause gastrointestinal symptoms and hemorrhage compared to ASA. Neutropenia was not noted at all; there were isolated reports of the occurrence of thrombocytopenic purpura [11].
Thus, clopidogrel is slightly more effective than ASA in preventing vascular events. Clopidogrel may be more effective in patients with high vascular risk (history of stroke, peripheral arterial atherosclerosis, symptomatic coronary artery disease, or diabetes) [28].
Dipyridamole sustained release
Dipyridamole is close to ASA in its effectiveness in reducing the risk of recurrent strokes [19].
Combined antiplatelet therapy
Taking into account the different points of application and mechanisms of action of drugs with an antiplatelet effect, as well as the variability of the platelet response, their combined use to achieve an additive effect of aggregation inhibition seems theoretically justified.
Combination of clopidogrel and ASA
The MATCH (Management of Atherosclerosis with Clopidogrel in High-Risk Patients with Recent Transient Ischemic Attack or Ischemic Stroke, [18]) study, involving 7599 patients who had suffered an IS or TIA and had additional risk factors, assessed the effectiveness and safety of combination therapy, which included clopidogrel 75 mg and ASA 75 mg/day in relation to clopidogrel monotherapy at a dosage of 75 mg. The primary outcome event was a composite of stroke, myocardial infarction, death due to vascular pathology, or rehospitalization associated with ischemic episodes. There was no significant benefit of combination therapy over clopidogrel monotherapy in reducing the incidence of primary endpoints or recurrent ischemic events.
The effectiveness of combination therapy with clopidogrel (75 mg/day) and ASA (325 mg/day) compared with ASA monotherapy (325 mg/day) was assessed in the CHARISMA (Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization Management and Avoidance) study. After 30 months of observation of patients, the incidence of the combined endpoint, which included IS, MI, death from a vascular cause in patients receiving combination antiplatelet therapy, was 6.8% and was less than in the group of patients receiving ASA monotherapy, where this indicator was 7.3% (p = 0.22). Thus, the study did not demonstrate the advantages of combination therapy with clopidogrel and ASA compared with ASA monotherapy for this category of patients [28, 29].
Combination of dipyridamole and ASA
In the ESPS-2 study (European Stroke Prevention Study, [19]), 6602 patients with a history of stroke or TIA were randomized, taking into account the main risk factors for the development of ischemic brain injury, into groups of different regimens of extended-release dipyridamole and ASK. A significant reduction in the risk of stroke was achieved with ASA alone by 18%, dipyridamole alone by 16%, and the combination of both by 37%. No reduction in the risk of death was observed with any of the dosage regimens used. The effectiveness of combination therapy compared with ASA monotherapy was observed in reducing the risk of recurrent stroke (by 23%) and was 25% higher than the effectiveness of dipyridamole monotherapy.
Similar results were obtained in the international randomized, non-blinded study ESPRIT (European/Australian Stroke Prevention in Reversible Ischaemia). The purpose of one of the directions of this study was a comparative analysis of the effectiveness and safety of the combination of ASA (30–325 mg/day) with slow-release dipyridamole (400 mg/day) and ASA monotherapy (30–325 mg/day) in patients who had suffered a TIA or IS ( with a neurological deficit assessed as no more than 3 points on the modified Rankin scale) within 6 months before inclusion in the study. It is important to note that the study included only patients who had suffered atherothrombotic cerebrovascular accidents: 1363 received combination therapy, 1376 received monotherapy. The primary endpoint (vascular death, non-fatal IS, MI, symptomatic hemorrhagic complications) was achieved by 16% of patients receiving ASA monotherapy and 13% of patients receiving combined antiplatelet treatment (hazard ratio [HR] = 0.8; 95% confidence interval [CI] – 0.66–0.98), which allowed the authors to conclude that the combination of ASA and dipyridamole is more effective than ASA in the secondary prevention of vascular complications of IS of atherothrombotic origin. Following the publication of the ESPRIT results, a meta-analysis of studies on the combined use of dipyridamole and ASA, which included all the studies described above, confirmed the reliability of the conclusions of the ESPRIT study [7].
The results of the ESPS-2 and ESPRIT studies formed the basis of the ESO (2008) recommendations for secondary stroke prevention, in which the combination of ASA and slow-release dipyridamole is a first-line drug (along with clopidogrel) as an effective antiplatelet therapy (Class I, level of evidence A ). It should also be noted that for those in whom secondary prophylaxis with oral anticoagulants is indicated but is contraindicated, the ESO also recommends a combination of slow-release dipyridamole and ASA (although the level of evidence for this recommendation is low - class IV, GCP - Good Clinical Practice).
Thus, the range of drugs - antiplatelet agents - with proven efficacy and safety in multicenter studies is quite wide, and therefore the question of choosing an oral antiplatelet agent is logical. When choosing antiplatelet drugs after stroke or TIA, the influence of several factors should be taken into account. Concomitant somatic pathology, side effects, and the cost of the drug may influence the choice of therapy: monotherapy with ASA, clopidogrel or a combination of ASA and dipyridamole. The low cost of ASA promotes its long-term use. However, if you look at it differently, even a small reduction in the frequency of vascular episodes observed with the use of dipyridamole or clopidogrel suggests a certain adequacy of the cost-effectiveness ratio of the drugs, which is comparatively more noticeable than with ASA. In patients who cannot tolerate ASA due to allergies or gastrointestinal side effects, clopidogrel or dipyridamole should also be recommended. The combined use of ASA and clopidogrel may be acceptable for patients who have recently suffered an acute coronary attack or stenting surgery [46].
Anticoagulant therapy
It has been established that in more than 67% of cases, strokes develop against the background of cardiac pathology; and about 15% occur against the background of chronic atrial fibrillation.
A breakthrough in the secondary prevention of IS in patients with atrial fibrillation was the use of vitamin K epoxide reductase inhibitors (warfarin, dicumarol, acenocoumarol, phenindione), which reduced the incidence of recurrent strokes in atrial fibrillation from 12 to 4%. The mechanism of action of drugs in this group is the suppression of vitamin K-dependent synthesis of biologically active forms of blood coagulation factors II, VII, IX and X. Doses of drugs that ensure maximum effectiveness of oral anticoagulant therapy largely depend on the individual sensitivity of the patient, and therefore A prothrombin test and international normalized ratio (INR) are used to monitor therapy.
It must be emphasized that therapy with oral anticoagulants after non-cardioembolic ischemic stroke is not more effective than therapy with antiplatelet agents (acetylsalicylic acid - ASA), but leads to a greater number of bleedings [7, 32, 41. However, drugs in this group (with achieving the target INR level of 2 ,0–3.0) are the drugs of choice for the secondary prevention of cardioembolic stroke (in patients with non-valvular atrial fibrillation in both permanent and paroxysmal forms), as well as in most other conditions accompanied by cardiac embolism.
The advantages of warfarin over antiplatelet therapy in the secondary prevention of IS are most clearly demonstrated in the EAFT and ACTIVE W studies.
The EAFT (European Atrial Fibrillation Trial) study included 455 patients with non-rheumatic atrial fibrillation who had suffered a minor IS or TIA within 3 months before inclusion in the study. As the primary endpoint, the study analyzed the incidence of vascular death, nonfatal stroke, nonfatal myocardial infarction, and systemic (noncerebral) thromboembolic episodes recorded at least once every 4 months. Patients were prescribed an open-label oral anticoagulant (the drug was chosen by the attending physician) until an INR of 2.5–4.0 was achieved, or using a double-blind method—ASA (300 mg/day) or placebo. The rate of reaching the end point was 8% per year for patients receiving oral anticoagulants, 17% in the control group. Thus, indirect anticoagulant therapy is more effective than ASA therapy as secondary prevention of thromboembolic episodes in patients who have suffered an IS or TIA [21].
The ACTIVE W (Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events) study analyzed the effectiveness of warfarin therapy (up to an INR of 2.0–3.0) compared with combined antiplatelet therapy ASA (75–100 mg/day) and clopidogrel (75 mg/day). The study included 6702 patients with atrial fibrillation and one or more risk factors for stroke (age 75 years and older; hypertension; previous IS or TIA; decrease in left ventricular ejection fraction below 45%; peripheral atherosclerosis; coronary artery disease or diabetes in people 55– 74 years old). The primary endpoint was the incidence of IS, non-cerebral thromboembolic events, MI and vascular death. The safety criterion was the incidence of hemorrhagic complications. The study was interrupted in September 2005 due to evidence of superiority of warfarin over combination antiplatelet therapy: 5.64% of patients receiving antiplatelet therapy and 3.94% of patients receiving warfarin reached the end point (p = 0.0002). It should be noted that more than 3/4 of the patients were initially treated with warfarin. The risk of hemorrhagic complications in the study groups did not differ and amounted to 2.4 and 2.2% per year (p = 0.67) in the groups of combined antiplatelet and anticoagulant therapy [6].
However, despite the convincing evidence base, the use of warfarin and other drugs in this group is associated with a number of clinical problems, such as genetically determined resistance to therapy, variability of the anticoagulant effect depending on the diet and concomitant therapy, as well as the need for monthly INR monitoring, which is not always done by patients.
Recent years have been marked by the emergence of several drugs whose anticoagulant effect does not require laboratory monitoring. The drugs dabigatran, a direct thrombin inhibitor, and rivaroxaban, a selective and reversible inhibitor of factor Xa, have proven their effectiveness in the primary and secondary prevention of stroke due to atrial fibrillation, comparable to warfarin, and well tolerated in the RELY [17] and ROCKET AF studies [33 ] respectively.
Anticoagulant therapy after cardioembolic stroke must be carried out for a long time or for at least 3 months after IS that occurred against the background of acute MI [44]. There are conflicting opinions about when anticoagulant therapy should be started. After a TIA or minor stroke, therapy (with warfarin, dabigatran or rivaroxaban) should begin immediately, but in the case of a severe stroke with signs of extensive infarction, according to neuroimaging methods (for example, when the lesion size is more than a third of the blood supply of the middle cerebral artery), anticoagulant therapy is necessary start in a few weeks (the issue must be resolved individually in each case).
Patients with atrial fibrillation and stable coronary artery disease should not combine oral anticoagulants with ASA [26]. Anticoagulant therapy may be preferable for patients with aortic atheroma [20], fusiform basilar artery aneurysm [22], or cervical arterial dissection [24].
Today, according to evidence-based medicine, the use of oral anticoagulants for the purpose of secondary prevention is recommended for patients with atrial fibrillation who have had a stroke, as well as for patients with verified cardioembolic origin of stroke. Moreover, if warfarin is used as an oral anticoagulant, the target INR level is 2.0–3.0 [28, 29]. When using rivaroxaban or dabigatran, INR monitoring is not required.
WHAT IS A TRANSIENT ISCHEMIC ATTACK?
A transient ischemic attack (TIA) or “mini-stroke” occurs when an obstruction to the flow of blood through one of the vessels of the brain is created for a short period of time (up to 60 minutes). This is not yet a stroke, but an alarming sign of the danger of its development, since the mechanisms of occurrence of these two conditions are the same, but lost functions (numbness of an arm or leg, impaired vision or speech) after a transient ischemic attack are very often restored.
WHAT IS ISCHEMIC STROKE?
An “ischemic stroke” means that blood flow through a vessel supplying the brain with oxygen and nutrients is interrupted, and the brain cells in the area where the circulation is disrupted die. In medical parlance, this is called a cerebral infarction. Due to the death of brain cells, a person loses control over the functions for which this part of the brain is responsible. The severity of these disorders depends on the location of the blood clot blocking the vessel and the diameter of the vessel that is blocked. Different areas of the brain control different brain functions, for example, if the right side of the brain is affected, weakness or paralysis of the left side of the body develops. The manifestations of a stroke depend on which area of the brain is affected. Most often, stroke affects people after 60 years of age. Every third stroke that develops is fatal. It may take 6 months or more to restore lost functions after a stroke. Many recover completely and return to work and a full life.