You can familiarize yourself with other diseases starting with the letter “G”: Ganglioneuritis, Ganglioneuroblastoma, Ganglionitis of the pterygopalatine node, Soft tissue hematoma, Hematomyelia, Hemiballism, Hemorrhagic stroke, Ganglioneuroma, Hemangioblastoma, Hemifacial spasm, Generalized epilepsy, Germinoma of the brain, Hydrocephalus, Hyperventilation syndrome, Hyperkinesis, Hypersomnia, Hypertensive cerebral crisis, Hypertensive encephalopathy, Hypnic headache, Brain glioma
Hypertensive encephalopathy: how to maintain brain health
Chronic progressive damage to brain tissue caused by pathology of cerebral hemodynamics, which is provoked by prolonged hypertension, is called hypertensive encephalopathy. It develops in patients with poorly controlled, sudden increases in blood pressure. Characteristic symptoms of HE are signs of dyscirculatory encephalopathy. To make a diagnosis, not only an examination by a neurologist is required, but also a consultation with a psychiatrist and cardiologist, magnetic resonance imaging of the brain and a study of brain dynamics. Therapy requires taking antihypertensive drugs to stabilize blood pressure and adding nootropic, neuroprotective and symptomatic drugs.
Diagnostics
For early detection of encephalopathy in elderly people who already have cerebrovascular accidents, periodic monitoring by a neurologist is recommended. This applies to diabetics, hypertensive patients, and patients with atherosclerosis.
Diagnostics include:
- ophthalmoscopy;
- Echo-EG;
- EEG;
- REG;
- Ultrasound of blood vessels of the head and neck;
- duplex scanning;
- MRA/MRI;
- coagulogram, cholesterol level determination, blood pressure measurement.
Consultations not only with a neurologist, but also with a cardiologist, endocrinologist, ophthalmologist, and nephrologist can be scheduled.
General information about the disease
Discirculatory encephalopathy is most often caused by atherosclerosis. The second place among the causes of pathology is hypertension. GE is included in a separate category in ICD-10. It occurs in patients against the background of chronic symptomatic hypertension or hypertension. The term appeared in 1985. It was introduced into use by neurophysiologists N.V. Lebedev and I.V. Ganushkina. Hypertensive encephalopathy occurs with damage to small vessels. This distinguishes it from the atherosclerotic form. But the difference is conditional, since atherosclerotic changes rapidly progress against the background of GE.
Which doctor should I contact?
Discirculatory encephalopathy refers to neurological disorders. If alarming symptoms appear, you should consult a neurologist as soon as possible. The specialist will conduct an examination, make an accurate diagnosis and prescribe adequate treatment. The sooner help is provided, the more optimistic the prognosis for the patient
Get diagnosed with disculatory encephalopathy at Clinic No. 1:
- MRI
- Consultation with an ophthalmologist
- EEG, REG
- Ultrasound of vessels
- Duplex scanning
For one-time payment for services - 20% discount
Call
The reasons that provoke it
The disease develops against a background of high blood pressure, regardless of whether hypertension is primary or secondary, forming against the background of endocrine disorders, kidney damage or atherosclerosis of the aorta. Hypertension can be provoked by pathologies such as chronic pyelonephritis, glomerulonephritis, hypercortisolism, pheochromocytoma, hyperaldosteronism. The development of hypertensive encephalopathy is caused by factors such as:
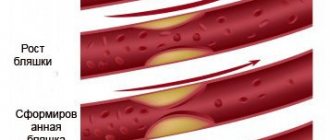
Hypertensive crises, since a rapid rise in blood pressure thins and increases the permeability of the vascular wall. Because of this, hemorrhagic impregnation of the cerebral tissue occurs at the site of thinning;- Uncontrolled high blood pressure leads to more rapid changes in blood vessels than in patients who regularly receive antihypertensive therapy. It is worth noting that even with the use of medications, in some cases it is not possible to correct hypertension;
- High pulse pressure aggravates the course of the pathology, since it causes additional stress on the muscular system and vascular walls. According to studies, the difference between diastolic and systolic pressure is 40 mm Hg. st;
- Nocturnal hypertension is dangerous because it occurs hidden. Because of this, it is not corrected in a timely manner and leads to prolonged spastic states of cerebral vessels with the development of ischemia in the tissues of the central nervous system.
Hypertensive form of encephalopathy - what is it?
Hypertensive encephalopathy syndrome is a dysfunction of the brain as a consequence of advanced hypertension. The disease was studied back in 1928.
Since then, medicine has been able to accumulate sufficient experience for targeted therapy. Today it is known for sure that encephalopathy is a consequence of:
- Sudden changes in blood pressure;
- Eclampsia;
- Hypertensive crisis;
- Acute pyelonephritis.
The most dangerous complication is in the form of a hypertensive crisis, when in acute hypertensive encephalopathy the clinic manifests itself with serious symptoms: severe cognitive impairment, tissue necrosis, and lack of normal functioning of organs and systems.
Fortunately, the disease can be corrected if it is detected early and treated adequately.
Development mechanism
When blood pressure rises, a compensatory mechanism appears, causing the small vessels of the arterioles to narrow to prevent their rupture. The pathogenesis is due to the fact that a regular increase in blood pressure leads to hypertrophy of the muscular layer of the walls of arterioles, which leads to thickening of the walls of blood vessels and a narrowing of their lumen. The process occurs in all tissues, but the most quickly affected are the brain, heart, and kidneys. As the lumen of the cerebral arterioles decreases, cerebral perfusion begins to fall and chronic ischemia of the central nervous system develops. Brain tissue suffers from a constant lack of oxygen and nutrients, which leads to degenerative processes. Atherosclerotic changes further aggravate cerebrovascular insufficiency and intensify its symptoms.
This leads to early damage to the white matter, expansion of the perivascular spaces, and demyelination of nerve fibers. Degenerative processes are accompanied by individual local foci - lacunar infarctions. But basically the changes are diffuse in nature and symmetrical in both hemispheres. They begin from the lateral ventricles and spread periventricularly.
Classification of encephalopathy
GE progresses gradually. Symptoms worsen and the condition of cerebral tissue deteriorates. To prescribe effective therapy, a classification has been developed that allows us to determine at what stage the pathology is. Neurologists distinguish three stages of hypertensive encephalopathy:
At the first stage, one can note the presence of subjective sensations of the patient, including complaints of fatigue, memory loss, and headaches. Objective symptoms are not expressed. Cognitive disorders are only detected through rigorous testing;- At the second stage, pronounced neurological symptoms appear: atactic, pyramidal, vestibular, subcortical, dysmnestic syndrome. Most often, one of the symptoms is dominant. Cognitive impairment remains moderate, but social adaptation is reduced. There are objective difficulties in pre-professional activity;
- At the third stage, the symptomatic picture increases and other syndromes join. The debut of parkinsonism, pseudobulbar syndrome, and epileptic seizures is possible. There are severe cognitive impairments, including dementia. Household and professional adaptation is disrupted.
Symptoms and stages of development
Symptoms of the disease vary depending on the degree of damage:
- In the first degree of DEP, anxiety, vulnerability, irritability, and frequent mood swings appear. The patient gets tired quickly and periodically complains of headaches. Memory deteriorates, fatigue is observed after physical exertion. Unsteadiness, unsteady gait, and nausea may occur.
- The second stage is characterized by more serious symptoms, obvious cognitive impairment and movement disorders appear. The headache becomes frequent, the patient feels a noise in the head, lethargy, and sleeps poorly. There may be difficulties with swallowing, coordination, speech, hearing are impaired, tremors of the head and hands, and convulsions appear. There may be flashes of light in front of the eyes.
- The third degree is accompanied by a serious lack of coordination and is essentially vascular dementia. Vision, hearing and speech are impaired, the patient's behavior is inadequate. There is a shuffling gait, constant tremors of the head and hands, fecal and urinary incontinence, and convulsions.
Clinical manifestations
At the initial stage, slowly progressive nonspecific symptoms are observed. It includes:
Cephalgia;- Chronic fatigue;
- Memory impairment;
- Decreased concentration.
As the pathology develops, certain neurological syndromes appear. Dysmnestic syndrome is manifested by memory impairment. With a subcortical disorder, tremor, secondary parkinsonism, and hyperkinesis dominate. Vestibular is characterized by unsteadiness of gait, pyramidal - muscle weakness such as mild hemiparesis.
Also observed:
- Narrowing the range of interests;
- Deterioration in the speed and productivity of thinking;
- Apraxia, that is, difficulties with organizing activities;
- Motivation problems;
- Increased emotional lability;
- Problems in the cognitive sphere arise due to a lack of a critical attitude towards one’s own state;
- Behavioral and affective disorders.
The clinical picture is characterized by a transient improvement of the condition and flickering of the symptomatic picture.
The third stage of the disease is accompanied by severe cognitive and organic disorders:
Agnosia;- Apraxia;
- Dysarthria;
- Decay of intellectual abilities;
- Personality change;
- Mental disorders;
- Loss of professional skills;
- Pseudobulbar palsy;
- Vascular dementia with personality disorder;
- Violent crying;
- Swallowing disorder;
- Epileptic paroxysms caused by lacunar infarctions;
- Syncope;
- Increases in ataxic, pyramidal and parkinsonian syndrome, which limit the possibility of household services and independent movement.
Possible complications
Hypertensive encephalopathy in its chronic form is often accompanied by acute episodes that occur against the background of a rapid rise in blood pressure. They are caused by hypotonic dilatation of intracerebral vessels and disruption of vascular regulation. This condition is caused by sweating of blood plasma with the formation of perivascular edema. In the absence of adequate timely treatment, the acute form of HE can lead to hemorrhagic or ischemic stroke, lacunar infarction. Pseudobulbar syndrome arising against the background of pathology leads to dysphagia, which leads to possible food getting stuck in the larynx and asphyxia, as well as the reflux of food particles into the respiratory tract, threatening the development of aspiration pneumonia.
Who is diagnosed with encephalopathy?
Surprisingly, the discirculatory form of the pathology is more often detected in hypertensive patients in young or middle age. Statistics show a significant spread: 0.5–15% of hypertensive patients are at risk of developing cerebral encephalopathy of varying severity.
Primary signs stop quickly: after 1-2 days they disappear. At risk are patients experiencing constant stress and excessive stress on the brain. Such conditions cause an increase in blood pressure and vascular spasms, and, therefore, provoke the development of the disease.
If vision problems unexpectedly arise - sharpness decreases, signs of color blindness appear, or one eye goes blind, one of the reasons will be encephalopathy. In any case, in 4 out of 11 examined people, as practice shows, this is exactly what happens.
Per 100 thousand people, the incidence rate of hypertensive encephalopathy looks like this.
| Men | Women | |||||||||
| Age, number of years | 3-14 | 14-25 | 25-40 | 40-60 | 60 + | 3-14 | 14-25 | 25-40 | 40-60 | 60 + |
| Number of patients | 0.5 | 30 | 40 | 50 | 186 | 0.5 | 30 | 40 | 50 | 186 |
Diagnostic methods
If a characteristic symptomatic picture develops against the background of hypertension, the specialist suggests hypertensive encephalopathy. Diagnostics is required to exclude other cerebral pathologies, as well as to assess the degree of changes in the central nervous system and blood vessels. The main diagnostic stages include:
Consultation with a neurologist to assess the patient’s neurological status. In the initial stages of the disease, it remains unchanged. Anisoreflexia may develop. Cognitive testing is also carried out to determine minor mnemonic, gnostic and praxic changes;- Cardiac examination can confirm the presence of hypertension. The specialist may prescribe echocardiography, ECG, daily blood pressure monitoring;
- A mental examination is carried out by a neuropsychologist, a psychiatrist, if there are suspicions of mental abnormalities. During the consultation, anamnesis collection, conversation, testing and observations are carried out;
- Study of cerebral hemodynamics using duplex scanning of cerebral vessels, magnetic resonance imaging of cerebral vessels, transcranial ultrasound. Diagnostics makes it possible to identify narrowing of the lumen of arterioles, determine where the most pronounced changes are localized, and also clarify the degree;
- Laboratory tests to determine the level of lipid spectrum and cholesterol in the blood. In addition, a Rehberg test, a biochemical blood test and a urine test are required to assess kidney function;
- MRI of the brain is the most informative method, allowing maximum visualization of the state of brain tissue and detection of disorders at the earliest stages. Reveals diffuse degenerative changes, foci of previous lacunar infarctions in stage II-III hypertensive encephalopathy and excludes organic pathologies of the central nervous system.
Consultation with an epileptologist and electroencephalography can reveal paroxysmal activity. If renal dysfunction is detected using urine tests, consultation with a nephrologist and ultrasound of the kidneys is necessary.
During diagnosis, it is very important to distinguish hypertensive encephalopathy from Parkinson's disease, slow CNS infections, encephalitis, brain tumors, Alzheimer's, demyelinating diseases and Creutzfeldt-Jakob disease. The vascular nature of the lesion is revealed by traces of lacunar infarctions, noticeable during MRI.
Methods of therapy
How effective the treatment will be primarily depends on whether the blood pressure can be stabilized. Neurological therapy is carried out while taking antihypertensive drugs and treating the primary disease that provokes hypertension. Treatment of hypertensive encephalopathy is aimed at improving cerebral perfusion, restoring the functions of the central nervous system, and maintaining the metabolism of brain tissue. For this purpose the following are assigned:
Preparations to improve blood microcirculation. The course takes anticoagulants, for example dipyridamole, acetylsalicylic acid. Taking pentoxifylline can also improve microcirculation;- Vasodilators help relieve spasm of arterioles, that is, the main pathogenetic link in the development of GE. The choice of drugs should take into account the presence of side steal syndrome. It is necessary to focus on such medications as: calcium channel blockers, phosphodiesterase inhibitors, a2-adrenergic receptor antagonists;
- Symptomatic drugs that are prescribed depending on the clinical picture accompanying encephalopathy. For hyperlipidemia, the prescription of statin drugs is indicated. If there is a decrease in cognitive abilities, taking nootropics is necessary. When mental abnormalities occur, mood stabilizers, sedative pharmaceuticals, and tranquilizers are needed. For epileptic paroxysms - anticonvulsants;
- Neuroprotectors can increase the resistance of nerve cells to a reduced supply of nutrients and chronic hypoxia. This group of drugs includes antioxidants: lipoic acid, ethylmethylhydroxypyridine succinate and amino acid drugs: glycine, aminobutyric acid.
Drug therapy for hypertensive encephalopathy
Hypertensive encephalopathy is a progressive damage to the brain substance caused by a lack of blood circulation in the cerebral vessels due to a poorly controlled increase in blood pressure (BP). Pathomorphological changes in the cerebral vessels in arterial hypertension (AH), such as plasmatic and hemorrhagic impregnation, necrosis of the vascular wall with its subsequent thinning and adaptive thickening of the walls of extracerebral vessels, are defined by the term “hypertensive angioencephalopathy”.
Early damage to the predominantly white matter of the brain in hypertension, which is the destruction of the myelin of the central conductors, small cavities, dilated perivascular spaces (creblures) due to edema, spongiosis, is caused by damage to the cortico-medullary arteries and has a typical picture on CT (decreased signal intensity) and MRI (increasing signal intensity). This phenomenon, usually detected in areas of the so-called terminal blood supply (periventricular areas of the brain), which are especially sensitive to fluctuations in blood pressure, is called hypertensive leukoencephalopathy, or leukorrheosis. ICD-10 mentions only hypertensive encephalopathy, the terms “hypertensive leukoencephalopathy” and “hypertensive angioencephalopathy” are not used, and the term “progressive vascular leukoencephalopathy” in the classification implies that hypertension is not the only cause of this process. From this point of view, subcortical atherosclerotic encephalopathy (Binswanger disease) is of interest, which is considered by some authors as a variant of hypertensive encephalopathy, and by others as an independent nosological unit, since hypertension is not detected in all patients with brain damage, and in addition, it is not always possible to carry out parallel between the values of systolic and diastolic blood pressure and disease progression. A significant difference between hypertensive encephalopathy and atherosclerotic encephalopathy can be considered the predominant damage in hypertension to small branches of brain vessels, rather than large extracranial and intracranial arteries. However, the division of hypertensive and atherosclerotic encephalopathy is quite arbitrary. Hypertension quite quickly leads to the development of atherosclerotic changes in the vessels of the brain. It is not always possible to detect atherosclerotic changes in extracerebral and cerebral vessels with ultrasound and MRI angiography in patients with hypertension, however, given the low sensitivity of these methods, in such cases it is impossible to completely exclude the presence of atherosclerosis and confidently make a diagnosis of “hypertensive encephalopathy”. Apparently, in most cases we are talking about “mixed” encephalopathy. It is hardly possible to separate these types of encephalopathy based on clinical manifestations. Many works have been devoted to the clinical manifestations of encephalopathy and its course, but there is no exact idea about the pathogenesis of hypertensive encephalopathy. Many researchers artificially expand the concept of “encephalopathy”, using this term to designate the initial signs of cerebrovascular insufficiency, which is not progressive in nature in all cases. Others believe that hypertensive encephalopathy is always a consequence of a malignant variant of hypertension, which is also characterized by kidney damage.
With hypertensive encephalopathy, as with all other forms of discirculatory encephalopathies, three stages of the disease can be distinguished. At stage I
the clinical picture is dominated by subjective disturbances in the form of general weakness and fatigue, emotional lability, sleep disturbances, decreased memory and attention, and headaches.
Neurological disorders are represented by anisoreflexia, incoordination, and symptoms of oral automatism. There are no distinct neurological syndromes at this stage. Violations of memory, praxis and gnosis can be identified, as a rule, only when conducting special batteries of tests. At stage II
, subjective sensations worsen, and distinct neurological syndromes (pyramidal, discoordination, amyostatic, dysmnestic) are formed, usually with dominance of one of them.
Professional and social adaptation of patients decreases. Stage III
, along with an increase in neurological symptoms, is characterized by the appearance of pseudobulbar syndrome, paroxysmal conditions (including epileptic seizures), severe cognitive impairment, which causes social and everyday maladjustment and loss of performance. Thus, hypertensive encephalopathy ultimately leads to the formation of vascular dementia (usually subcortical).
In stages II and III of hypertensive encephalopathy, diffuse changes in the brain substance are usually combined with focal lesions in the form of lacunar infarcts - small cavities ranging in size from 0.1 to 1.0 cm, formed in areas of cerebral ischemia. Either asymptomatic development of a lacunar infarction or the formation of a transient ischemic attack or stroke is possible, which depends on the location and volume of the ischemic focus. The formation of multiple small-focal brain lesions - the so-called lacunar state - significantly worsens the prognosis of hypertensive encephalopathy and reduces the possibility of drug correction of the patient’s condition, even when good control of hypertension is achieved. Treatment of hypertensive encephalopathy includes several areas:
- treatment of arterial hypertension;
- impact on factors that aggravate the course of hypertensive encephalopathy - hypercholesterolemia, increased platelet aggregation and blood viscosity, diabetes mellitus, atrial fibrillation, smoking, alcohol abuse, etc.;
- improving blood supply to the brain;
- improving the metabolism of nerve cells under conditions of ischemia and hypoxia.
There is no doubt that effective therapy for hypertension at the earliest stages of the disease can prevent the development of encephalopathy, but the problem is that many patients do not experience elevated blood pressure for a long time. The basis for the prevention of hypertensive encephalopathy in patients with hypertension is to achieve control over hypertension, namely the target level of blood pressure, at which the threat of the risk of developing cerebrovascular complications is minimal. Tactically, this can be solved by prescribing antihypertensive drugs and correcting existing risk factors. The target blood pressure level can vary significantly depending on the presence of risk factors for the development of cerebrovascular complications (diabetes mellitus, renal failure, etc.). Thus, the target level of systolic blood pressure in the general population of patients with hypertension is less than 140 mm Hg. Art., diastolic - less than 90 mm Hg. Art., while for patients with chronic renal failure - less than 120 mm Hg. Art. and 75 mm Hg. Art. respectively. Achieving the target blood pressure level, especially with initially high blood pressure values in patients with cerebrovascular pathology, should not occur in a short time, as this is fraught with the development of ischemic stroke. Depending on the initial level of blood pressure, duration of the disease, and the severity of cerebral disorders, this period should be from 6 to 12 weeks.
The question of the advisability of prescribing additional pharmacological drugs to patients with hypertension without cerebral symptoms that affect the rheological qualities of the blood, stimulate endothelium-dependent reactions of the vascular wall, improve metabolic processes in brain tissue, and reduce the content of free radicals has not been fully studied. In elderly people with lipohyalinosis of the walls of small vessels, courses of treatment with drugs that improve cerebral blood flow and have neuroprotective properties are advisable even with good blood pressure control. The use of these drugs in courses lasting 2–3 months with breaks of 6–8 months can slow down the development of vascular pathology and prevent damage to the brain substance. Prevention of damage to brain structures in hypertension should include not only effective control of hypertension, but also additional treatment aimed at improving cerebral blood flow and metabolic processes in the brain.
At stage I of hypertensive encephalopathy, it is necessary to add to the main therapy drugs that improve cerebral blood flow and metabolism of nervous tissue, as well as drugs that act on internal factors that can affect the progression of encephalopathy. In stages II and III of hypertensive encephalopathy, the general principles of therapy remain the same, but, first of all, the dosages of drugs acting on cerebral blood flow and metabolic support of brain structures change. To prevent the progression of atherosclerotic processes, normalization of fat metabolism is necessary, which implies a decrease in body mass index (following a low-fat diet) and taking statins. With good and satisfactory blood pressure control, it is possible to prescribe antiplatelet agents to improve the rheological properties of the blood. The use of drugs with a vascular protective effect, which improve the metabolism of brain tissue and have neuroprotective properties, is mandatory at all stages of hypertensive encephalopathy. One of the highly effective drugs of combined action is Mexidol.
Mexidol (2‑ethyl-6‑methyl-3‑hydroxypyridine succinate) belongs to the group of antihypoxants with antioxidant, nootropic and anxiolytic properties. The drug improves cerebral metabolism and blood supply to the brain, microcirculation, rheological properties of blood, reduces platelet aggregation, has a hypolipidemic effect, and reduces the level of total cholesterol and LDL. Mexidol improves cell energy metabolism, synaptic transmission, activates the energy-synthesizing functions of mitochondria, affects the content of biogenic amines, inhibits free radical oxidation of lipids and the synthesis of thromboxane A, enhances the synthesis of prostacyclin, increases the activity of antioxidant enzymes, SOD. The lipid-lowering effect of this drug is to reduce the amount of total cholesterol and LDL, reducing the cholesterol/phospholipid ratio. Mexidol also modulates the receptor benzodiazepine, GABAergic, acetylcholine complexes of brain membranes, enhances their ability to bind, stabilizes biological membranes, membranes of erythrocytes and platelets.
The nootropic effect of the drug is carried out by stimulating the transmission of excitation in central neurons, improving cerebral blood flow, metabolic processes and information exchange between the hemispheres, which helps improve memory, learning, preserving a memory trace and counteracts the process of extinction of acquired skills and reflexes. The drug eliminates the symptoms of hypomnesia, increased absent-mindedness, improves the ability to concentrate and count, short-term and long-term memory. Mexidol accelerates the recovery of motor functions in patients who have suffered a stroke. The drug increases the degree of control of the cerebral cortex over subcortical structures, provides a psychoanalgesic, anxiolytic effect, and reduces extrapyramidal dysfunction. The pronounced antihypoxic and anti-ischemic effect is due to a direct effect on the endogenous respiration of mitochondria with activation of their energy-synthesizing function. The antihypoxic effect of the drug is due to the presence of succinate in its composition, which, entering the intracellular space, under hypoxic conditions is capable of being oxidized by components of the respiratory chain. Mexidol has a pronounced geroprotective effect, helps restore emotional and vegetative status, and smoothes out the manifestations of neurological deficits. For the treatment of hypertensive encephalopathy, Mexidol is recommended to be administered either 100 mg (2 ml) per 10.0 ml of physiological NaCl solution intravenously daily for 10 days; or 200 mg (4 ml) intramuscularly daily for 10 days. After a parenteral course of treatment with Mexidol, it is advisable to take a tablet form of 0.125 g three times a day for 2–6 weeks. You can also start treatment by taking the tablet form of 0.125 g three times a day for a course of at least 4-6 weeks.
A number of studies provide evidence of the high effectiveness and safety of Mexidol. At the Krasnoyarsk State Medical Academy, the effectiveness and safety of Mexidol was studied in patients with various forms of chronic cerebrovascular insufficiency [5]. After three weeks of use of the drug, a subjective improvement in the patients’ condition was noted (complaints of noise in the head, weakness and anxiety decreased). Mexidol had a positive effect on memory, improved concentration and emotional state of patients. At the Department of Nervous Diseases of the Military Medical Academy of St. Petersburg, the dynamics of changes in neurological symptoms and syndromes in patients with chronic cerebrovascular accidents during complex therapy using the drug Mexidol was studied [6]. During therapy with Mexidol, early normalization of coordination functions and overcoming asthenic syndrome were revealed, and the dependence of the severity of cranialgic syndrome on the degree of dyscirculatory disorders in the veins of the brain and the elimination of its manifestations was shown. At the Research Institute of Neurology of the Russian Academy of Medical Sciences, a comprehensive clinical and biochemical study of the effectiveness of Mexidol in patients with chronic cerebrovascular diseases was carried out with a detailed analysis of the relationship between the clinical effectiveness of the drug and the quantitative characteristics of oxidative stress. Analysis of the study results demonstrated the promise of using Mexidol as a neuroprotector for vascular diseases of the brain. It was concluded that the use of Mexidol in patients with chronic cerebrovascular diseases leads to an improvement in the condition of patients and a decrease in the severity of the most common clinical manifestations of this pathology - asthenic syndrome, psychoemotional disorders and cochleovestibular disorders. The maximum therapeutic effect of Mexidol is observed in patients with an initially increased content of lipid peroxidation products and depletion of the body's antioxidant systems, which indicates the importance of oxidative stress in the pathogenesis of chronic cerebrovascular diseases. The biochemical basis of the therapeutic effect of Mexidol is its antioxidant activity: the drug significantly reduces damage to lipoprotein structures, restoring the activity of the endogenous antioxidant system [7].
Hypertensive encephalopathy is a progressive disease characterized by a variety of neurological syndromes, a high risk of stroke and leading to vascular dementia. Timely and correctly selected therapy makes it possible to maintain the patient’s professional, social and everyday adaptation for many years, and improves the prognosis for the patient’s life expectancy. The effectiveness of treatment of hypertensive encephalopathy increases when antihypertensive drugs are combined with drugs that improve cerebral blood flow, metabolism of nervous tissue and have a neuroprotective effect.
Forecast
A prognosis can only be made taking into account the stage of hypertensive encephalopathy, the possibility of complete pressure correction, the presence of an underlying disease or concomitant pathologies such as endocrine system disorders and atherosclerosis. In the first stage of GE, complex neurological treatment and stabilization of pressure can ensure the patient’s ability to work and long-term intellectual safety. And in stage III, therapy only slows down the progression of the disease and alleviates its manifestations.
Treatment
Efficacy largely depends on successful normalization of blood pressure. As part of symptomatic treatment, measures are taken to improve intracerebral circulation, stimulate local metabolism, and restore brain functions. Pharmacological support includes:
- Vasodilators. Phosphodiesterase inhibitors and calcium channel blockers eliminate arteriolar spasm.
- Means for improving microcirculation. Pentoxifylline and long courses of anticoagulants are recommended.
- Neuroprotectors. Glycine, gamma-aminobutyric acid and antioxidants increase cell resistance to hypoxia and lack of nutritional compounds.
- Other medicines. They are selected taking into account current symptoms and laboratory test data. It may be necessary to prescribe statins, nootropics, tranquilizers, antidepressants, and anticonvulsants.