Final rating 0 (0 reviews)
Thanks to the author - Marina Kuznetsova
Today we will look at popular preparations containing iron for oral administration.
Here's what we'll look at:
- Differences between divalent and trivalent iron preparations. Their advantages and disadvantages.
- Features of some popular products.
- What effect do iron supplements have on teeth? How to avoid darkening?
- What questions should a buyer ask when selling iron supplements?
- What C.U. give to the client?
- Why can vegetarians have normal hemoglobin?
- What can be recommended to a buyer without a doctor’s prescription so as not to cause harm?
- Why does hemoglobin not increase despite long-term use of iron-containing medications?
- How long can pregnant women take iron supplements?
Well then. Let's get started.
All iron preparations can be divided into two groups: ferrous and trivalent iron preparations.
Ferrous iron preparations, their advantages and disadvantages
Representatives:
- Aktiferrin,
- Sorbifer Durules,
- Tardiferon,
- Totem,
- Fenyuls,
- Ferretab comp.
Benefits of ferrous iron supplements
- Well absorbed through the gastrointestinal mucosa.
- Increases hemoglobin faster than ferric iron supplements. They normalize hemoglobin after 1 - 2 months, and iron reserves return to normal after 3-4 months. For comparison: on average, ferric iron preparations normalize hemoglobin within 2-4 months, and iron reserves within 5-6 months from the start of treatment.
Disadvantages of ferrous iron preparations
- Very toxic. There is a high risk of iron overload, because the absorption of ferrous iron through the mucous membrane of the digestive tract is uncontrolled, and it may happen that all the transport proteins that should pick up iron and carry it either to the depot or to the sites of hemoglobin formation are occupied. Free iron then enters the bloodstream and causes various damage. There are many side effects from this. The risk of overdose is especially high in children. Do not recommend these drugs yourself!
- Ferrous iron promotes the formation of a large number of free radicals - harmful atoms or molecules that trigger a chain of new damage.
- Eating reduces their absorption, so ideally approximately 30-60 minutes before meals But they often cause abdominal pain, constipation, diarrhea, and patients are forced to take them during or after meals.
Some manufacturers, knowing such a sin behind their brainchild, recommend taking them before or after meals. “After” means if it is poorly tolerated. But this affects the absorption of iron and the speed of onset of the effect.
How do ferrous iron preparations differ from each other?
First of all, because they contain different iron salts: sulfate, fumarate, gluconate.
Of these, ferrous sulfate is the most toxic.
Ferrous sulfate preparations are prohibited for use in a number of countries for pregnant women, children and those with digestive tract diseases.
Remember, Ferroplex used to be in dragees? When I worked as a local pediatrician, a 9-month-old baby died in my area from Ferroplex poisoning - the adults left the package open in a visible place.
Other iron salts (fumarate, gluconate) are less toxic and safer.
The preparations also differ in the form of release and the content of “pure” iron.
The minimum effective therapeutic daily dose of iron is 100 mg, and the average daily therapeutic dosage is 100-300 mg.
The dosage of an iron supplement primarily depends on the purpose for which the drug is taken, and then on the severity of the anemia.
And the goal could be like this:
- Raise iron reserves in the depot. This is called “latent iron deficiency,” when hemoglobin and red blood cells are normal, but ferritin and some other blood parameters are reduced. It can be suspected by sticking in the corners of the mouth, dry skin, brittle hair, and split nails.
- Cure iron deficiency anemia.
- Prevent anemia in pregnant women.
After reading all this, you should have questions:
- Which preparations contain less toxic iron salts?
- How much iron is contained in different preparations?
A small cheat sheet for this group will help you. The download link is at the end of the article.
Symptoms of iron deficiency anemia (IDA, sideropenic syndrome)
Symptoms of iron deficiency anemia can, to one degree or another, appear much earlier than a person gets ready to get tested. Most often the skin and its appendages are affected, that is, nails and hair, the gastrointestinal tract, as well as the cardiovascular and nervous systems. In descending order of frequency of symptoms of long-term, slowly developing anemia, the signs are arranged as follows:
- increased skin dryness,
- excessive striations, layering and fragility of nails, changes in their structure and shape;
- hair begins to grow more slowly, and the ends of the hair split;
- mild fatigue and weakness appear, which intensifies as anemia progresses;
- shortness of breath on exertion, and as it progresses, pallor;
- if there is cyanosis of the nasolabial triangle, that is, its cyanosis, cyanosis of the earlobes or the tip of the nose, then this may not indicate anemia, but some kind of cardiovascular pathology, for example, a heart defect with a decrease in oxygenation of the capillaries with oxygen;
- an earthy complexion along with pallor may indicate the presence of malignant neoplasms;
- patients with anemia sometimes complain of a special, painful sensation of smells, hyperosmia, and taste perversion. Sometimes it is common to eat chalk, tooth powder or paste, raw cereals, and so on;
- fainting and dizziness, especially during a rapid transition from a horizontal to a vertical body position, can also be a serious sign of progressive anemia.
Typically, any anemia in its development goes through several stages before it becomes clinically and laboratory noticeable. The main stage from which the anemic process begins is the prelatent, or latent phase. There is no clinically significant iron deficiency yet; reserves that should be in the body are consumed to cover it. Then ferritin and transferrin begin to decrease, the concentration of free iron in the blood serum begins to change, and only then, as a gross laboratory symptom of anemia, the concentration of hemoglobin also decreases, since it is in the hemoglobin molecule that there is a special structure - heme, which contains iron.
The most common side effects of drugs containing iron
- Pain, discomfort in the abdomen.
- Constipation or diarrhea.
- Nausea, vomiting.
- Darkening of tooth enamel.
- Painting the stool black. Nothing wrong with that. Simply unabsorbed iron leaves the body naturally.
Drug interactions of ferrous iron preparations
- Calcium, magnesium, levothyroxine (Euthyrox, L-thyroxine), antacids reduce iron absorption.
- In turn, iron supplements reduce the absorption of fluoroquinolones and tetracyclines (Doxycycline, Unidox, Tetracycline, etc.).
- If you take these drugs together with drugs from the NSAID group, the risk of damage to the mucous membrane of the digestive tract increases.
- During treatment with ferrous iron preparations, you should refrain from drinking alcohol - it increases the frequency of toxic reactions.
Interaction with food of ferrous iron preparations
Milk and dairy products, cereals, egg yolks, coffee, tea and some other foods reduce iron absorption. In this regard, the interval between taking the ferrous iron preparation and consuming these products should be at least 2 hours.
What else?
Ferrous iron preparations can cause exacerbation of chronic inflammatory diseases of the stomach and intestines.
If a patient has such a problem, the drug must be chosen especially carefully.
As a last resort, as I already said, take it during or after meals.
The treatment will be longer but safer.
Now do you understand what questions you need to ask the buyer when selling these funds? What recommendations should you give, what should you warn about?
I will list it all below.
In the meantime, I’ll dwell on the features of individual ferrous iron preparations. Let me remind you once again that I will only talk about drugs for oral administration.
Introduction
Iron deficiency anemia (IDA) is one of the most common diseases in the world [1, 2], and among women of fertile age it is in first place in terms of incidence, often being a complication of pregnancy and childbirth, as well as a number of gynecological diseases [3–7] .
Another group of patients that especially often suffer from IDA are young children [8, 9], and in them IDA accounts for about 90% of all anemia. Nevertheless, any person, regardless of gender and age group, has a fairly high risk of encountering this problem at one stage or another in their life. Among the world's population, the incidence of IDA is unevenly distributed. According to experts from the World Health Organization (WHO), in developing countries it is several times higher than in developed countries. The range of fluctuations in the prevalence of IDA in the population ranges from 5 to 40% or more [10]. IDA is a polyetiological disease; it can have many different causes and predisposing factors [11]. These include socio-economic conditions, availability of medical care, nutritional habits, level of sanitary culture, prevalence of parasitic infestations and many others.
Etiology and pathogenesis of IDA
The development of IDA is associated with iron deficiency in the body, which in turn may be a consequence of impaired intake, absorption or increased loss of this microelement. In different sex and age groups, the predominant causes of IDA are distributed as follows:
- in women of fertile age [3–7]: heavy menstrual bleeding and menorrhagia (including due to pathologies of the reproductive system, such as endometriosis and fibroids),
- pregnancy (multiple pregnancies accompanied by early gestosis are in a special risk area),
- childbirth (especially repeated births with short intervals between them, as well as complicated by bleeding),
- miscarriages, frequent abortions,
- lactation;
- blood loss due to pathology of the gastrointestinal tract - gastrointestinal tract (esophageal bleeding, peptic ulcer of the stomach and duodenum, ulcerative colitis, Crohn's disease, polyposis, rectal fissures, hemorrhoids, tumors, etc.),
- iron deficiency at birth,
Iron plays an important role in the functioning of all organs and systems. It is a key element of the hemoglobin molecule, acting as a component of the protoporphyrin prosthetic group, responsible for the binding and transport of oxygen. Iron also takes part in the process of oxidative phosphorylation in cell mitochondria, in collagen synthesis, porphyrin metabolism, is present in significant quantities in muscle myoglobin, and is also necessary for the full functioning of the immune system [1]. And yet, the participation of iron in the processes of tissue respiration determines the main biological significance of this microelement. It is natural that with the development of IDA, one of the most significant problems becomes precisely tissue hypoxia and the pathology that it provokes [23–25].
A natural source of iron is food, which provides about 10–20 mg of this microelement daily in a normal, complete diet. Of this amount, no more than 10% (about 2 mg) is absorbed, which provides the daily need for iron. At the same time, most healthy menstruating women lose up to 20-30 mg of iron every month. A similar or even more critical situation may arise with some chronic diseases. It can be difficult to replace what is lost with iron from food, even if its content in the diet is quite high. The problem is aggravated in the presence of impaired absorption and absorption of iron. A gradually developing imbalance between the intake and loss of iron depletes its reserves in the body, leading to an iron deficiency state, in particular to IDA with progressive hemic hypoxia and accompanying metabolic disorders.
Depending on the predominant mechanism of development of iron deficiency, anemia is divided into the following groups [25]:
- associated with blood loss;
- associated with impaired iron absorption;
- associated with an increased need for iron;
- nutritionally dependent.
In some cases, signs from several groups with varying degrees of severity may occur.
Clinical manifestations and diagnosis of IDA
The main clinical manifestations of IDA are characterized by hypoxic and sideropenic syndromes [1, 2, 27, 28].
Signs that make up hypoxic syndrome:
- pallor of the skin and visible mucous membranes;
- cardiopalmus;
- noise in ears;
- headache, dizziness;
- general weakness;
- loss of appetite;
- decreased performance, concentration, memory impairment.
Components of sideropenic syndrome:
- perversion of taste and smell;
- dry skin, pigmentation (“coffee with milk”);
- deformations and changes in the structure of nails (cross-striations, concavity, thinning, fragility);
- deterioration of hair condition (fragility, dullness, split ends, hair loss up to alopecia);
- manifestations of angular stomatitis (“jams”);
- burning sensation in the tongue.
In addition to the listed symptoms, the development of neurosis-like disorders, the manifestation of neurasthenia, disorders of peripheral circulation and microcirculation, decreased tolerance to physical activity, changes in metabolism in the myocardium are also possible, leading with long-term IDA to increasing symptoms of myocardial dystrophy, as well as shifts in the autonomic regulation of cardiac activity towards sympathicotonia .
Negative changes in the functioning of the gastrointestinal tract are noted. Patients with IDA often suffer from chronic gastritis and intestinal pathology. Syndromes of impaired absorption of iron in the intestine are often secondary in nature, further aggravating iron deficiency [17]. Regenerative disorders in the gastric mucosa are currently considered as the causes of decreased secretion and acid formation in IDA.
IDA negatively affects the immune system [29]. Thus, iron deficiency indirectly disrupts the functioning of the cellular component of anti-infective immunity: the proliferation of lymphocytes slows down and the microbicidal activity of granulocytes decreases. This may lead to a slight increase in the risk of developing infections and their unfavorable course.
The listed variety of clinical manifestations of IDA, which sharply reduce the quality of life of patients, once again emphasizes the particular importance of timely diagnosis and full correction of this condition. A separate problem is the low specificity of most clinical symptoms [28], which makes it difficult to confidently diagnose IDA solely on their basis.
In this regard, laboratory data, incl. general blood analysis:
- assessment of hematocrit (diagnostic sign - its decrease);
- study of the number of red blood cells and reticulocytes in the blood (the number of red blood cells may be within normal limits or reduced, reticulocytosis is not typical, but can be observed with bleeding);
- determination of the average concentration and average content of hemoglobin in erythrocytes (these indicators are reduced, which reflects hypochromia of erythrocytes); determination of the shape and size of red blood cells (characteristic of anisocytosis with a tendency to microcytosis).
If IDA is suspected, it is also recommended to examine such indicators of iron metabolism as ferritin level (decreases), serum transferrin and serum iron-binding capacity (increases), serum iron and transferrin iron saturation coefficient (decreases).
For successful treatment, it is also important to determine the cause of the development of IDA, possible sources of blood loss, and concomitant diseases. For this purpose, X-ray examination of the chest organs, ultrasound examination of the abdominal organs, pelvis, and retroperitoneal space are used; electrocardiography, esophagogastroduodenoscopy, colonoscopy, as well as biochemical blood test, general urine test, etc. The results of basic studies help to choose the direction of further diagnostic search.
Treatment of IDA
The goal of treatment is to introduce iron into the body in an amount sufficient to normalize hemoglobin levels and replenish tissue iron stores [30–32]. At the same time, normal hemoglobin levels for women are 120–140 g/l, for men – 130–160 g/l, and a serum ferritin level above 40–60 μg/l indicates satisfactory accumulation of iron in the depot. This review examines the correction of IDA exclusively by pharmacological means. However, in some cases (severe IDA, concomitant cardiovascular pathology with the threat of decompensation due to iron deficiency, etc.), concomitant therapy with erythropoietin drugs, as well as blood transfusion therapy, can be prescribed on an individual basis.
When starting treatment for IDA, it is necessary to remember that anemia cannot be corrected with vitamin and mineral complexes containing iron. The vast majority of patients with IDA require special iron-containing medications [32]. Oral administration is a priority as a more convenient and safe way to use such drugs [33–35]. Parenteral iron preparations are used only if there are contraindications to oral administration, their poor tolerability or ineffectiveness. In this case, only the intravenous route of administration is recommended. Intramuscular injections of iron-containing drugs are ineffective and dangerous, because can cause infiltrates and even the development of myosarcomas.
Currently, preference is given to therapeutic regimens that involve taking 100–200 mg of elemental iron per day for adults (the optimal dose recommended by WHO is 120 mg/day). The use of more than 300 mg of iron per day is not advisable, because this usually does not increase the volume of absorption, while at the same time increasing the risk of developing undesirable side effects (stool disorders, signs of gastric irritation, etc.) [36]. When calculating the daily and course doses, the severity of the anemic syndrome, visceral lesions, and serum iron levels are taken into account.
The modern pharmaceutical industry offers a fairly wide range of iron preparations, which differ in their quantitative (high- and low-dose) and qualitative compositions (single-component, combined). Oral iron preparations are also conventionally divided into ionic (salt) divalent (of iron salts, sulfate is most often used) and non-ionic (non-salt) ferric iron preparations based on polymaltose complex hydroxide (HPC) and protein succinylate [37, 38]. Randomized studies in recent years have proven equal effectiveness of both groups. For a more successful result, it is advisable to prescribe vitamins in parallel with iron supplements. For example, ascorbic acid allows for better absorption and assimilation of iron [39] and the full course of plastic processes in the body.
It should be remembered that the therapeutic effect of iron supplements, as a rule, develops quite slowly, so ferrotherapy is a long process. Depending on the severity of iron deficiency, treatment can last from 1 to 3 months or more. At the same time, data are accumulating on the successful use of low-dose drugs in intermittent courses (2 weeks per month), as well as on the benefits of treatment in an alternating mode - every other day for a month [40]. The listed regimens provide a much lower frequency of side effects without loss of effectiveness. To avoid side effects and to increase patient adherence to therapy, it makes sense to refrain from unnecessarily prescribing high-dose drugs and multiple doses throughout the day.
WHO experts recommend the use of drugs with sustained release of iron [41]. This allows you to reduce the frequency of taking the drug, while simultaneously improving its absorption and tolerability. The duration of their use is determined individually, taking into account laboratory parameters. The main course of treatment continues until the optimal hemoglobin level is achieved and iron metabolism in the blood serum is restored. Further, in order to replenish tissue depots, it may be necessary to extend the drug intake for up to 2 months. If iron deficiency is severe, the total duration of treatment with oral sustained-release iron medications is usually 3 to 6 months [37, 41, 42].
Monitoring the effectiveness of treatment for IDA
Monitoring the effectiveness of treatment with iron supplements is carried out by monitoring the following laboratory parameters [42]:
- hemogram;
- ferritin;
- iron binding capacity of serum;
- transferrin.
With adequate therapy, patients’ well-being improves already on the 5th–6th day of taking the drug. On the 7th–12th day, one should expect a reticulocyte crisis - an increase in reticulocytes by 2 or more times from the initial values. Hemoglobin concentration begins to increase after approximately 2.5–3 weeks of treatment. By the end of the 4th week it should increase by 10 g/l. Complete normalization of this indicator is usually observed no earlier than a month from the start of treatment. Hemogram values in mild anemia usually return to normal after 5–8 weeks of ferrotherapy. It is important to dynamically monitor hemoglobin levels during treatment and after completion of the course. This indicator should be monitored monthly throughout the year, which makes it possible to decide on the need for maintenance treatment.
If the target hemoglobin level and normal serum ferritin level cannot be achieved, conditions that interfere with iron absorption, as well as the possibility of adverse drug interactions (for example, with antacids), should be excluded.
Prevention of IDA
Primary prevention of IDA and latent iron deficiency is, first of all, a complete, balanced diet for a person at any age. Secondary prevention of IDA is facilitated by regular preventive examinations of the population for the purpose of timely diagnosis and treatment of diseases that can lead to iron deficiency in the body. In this case, screening studies to identify iron deficiency conditions occupy a central place [43]. You should remember about risk groups for the development of latent iron deficiency and IDA. These include people with irreparable causes of iron deficiency (chronic blood loss, malabsorption syndrome, celiac disease, program hemodialysis, inoperable tumors, etc.), vegans and vegetarians, regular blood donors, and pregnant women. They are recommended to take additional preventive iron supplements.
Conclusion
IDA is a very serious and quite common problem, and the medical community is currently actively searching for optimal ways to solve it. Some progress has already been made in the development of effective and safe drugs for the treatment and prevention of iron deficiency conditions. Competent pharmacological correction of IDA can improve the quality of life and increase performance in the vast majority of patients with a similar diagnosis. In this case, it is advisable to use modern drugs, the production technologies of which ensure the maximum possible bioavailability of iron, and also minimize the risk of developing the most common side effects from ferrotherapy.
Aktiferrin
Oral dosage forms: drops, syrup.
Previously, there were also capsules, but now I don’t see them in the assortment of Russian pharmacies.
The composition contains ferrous sulfate, which, let me remind you, is characterized by maximum toxicity, and the amino acid serine. It improves iron absorption, since only 10-15% of ferrous iron is absorbed through the mucous membrane of the small intestine.
(And trivalent without helpers is not absorbed at all).
Pregnant and lactating women can.
Children: syrup from 2 years, drops from birth.
The dose is calculated per kg of weight.
The course of treatment is at least 8 weeks.
After hemoglobin returns to normal, you need to continue taking the drug for the same amount of time to replenish iron reserves.
What's not to like about Aktiferrin?
The manufacturer's instructions indicate the iron content in 100 ml of syrup or drops. This means that the doctor must calculate the daily dosage, taking into account the child’s weight and iron deficiency, which is determined by the formula. And if he is not good at mathematics, it is easy to make a mistake and either overdo the dose, or vice versa.
In the first case, this threatens with intoxication, in the second - too long a course of treatment.
Pharmacotherapy of anemic syndrome
Treatment should continue under the supervision of tests, and on average, oral replenishment of iron stores with medications lasts about 3-5 months, under the supervision of a doctor. In this case, of course, it is necessary to initially make sure that the loss of iron during treatment does not exceed the norm, otherwise the treatment will be useless.
In addition, it is necessary to strictly adhere to the principles of treatment of iron deficiency anemia. If iron deficiency anemia is diagnosed, and laboratory indicators indicate this, this means that diet alone is not enough. Even with the greatest saturation of it with iron, it is unlikely that more than 3 mg can be absorbed into the body. Modern medications can absorb 10 or even 20 times more iron than with the most balanced and saturated diet.
In most cases, for anemia, oral medications are sufficient, and blood transfusion, that is, blood transfusion of red blood cells, will be needed when hemoglobin decreases to 50 or 40 g per liter. Of course, this is a very severe anemia, and patients should not be subjected to it. Therefore, you need to try to prescribe iron as early as possible, and for a fairly long period of time, in order not only to eliminate the symptoms of anemia, both laboratory and clinical, but also to create a reserve of iron in the body, which was wasted in the initial, latent stages. This means that after normalizing the hemoglobin level and obtaining quite favorable tests, there is no need to stop treatment. It usually takes another two to three months, when a reserve of iron is created in the body, and half doses of drugs that managed to cure anemia are prescribed. If the growth of iron reserves in the body occurs slowly, then it is necessary to take additional medications, for example, multivitamins.
Various iron-containing drugs also, in turn, contain either ferrous or trivalent iron. Therefore, you can take both medications containing divalent and ferric iron. It is usually believed that when it comes to organic iron compounds, they are absorbed better, and iron compounds with maltose, ferrous gluconate, are still not as harsh as inorganic compounds of this metal, such as ferrous sulfate. But that is why organic iron compounds are a little more expensive.
All the drugs listed below are over-the-counter and can be purchased over the counter at pharmacies. All of them are included in national and international clinical guidelines for the treatment of anemia and sideropenic syndrome, and all are oral, that is, prescribed by mouth. That is, we will not consider medications containing iron for intravenous use, such as Venofer and Cosmofer. They are used in specialized settings, such as in patients on dialysis.
For medicines, the INN, that is, the international nonproprietary name, will be called first, and then the commercial name. The price is valid for the end of March 2021 for pharmacies of all forms of ownership in the Russian Federation. Almost all iron preparations are imported, and they have very few or no domestic analogues.
Sorbifer Durules
Release form: film-coated tablets.
The composition is the same ferrous sulfate (100 mg of pure iron) and ascorbic acid (60 mg).
The word “Durules” means a technology for the gradual release of the active substance, which in theory should reduce the number and frequency of adverse reactions.
The active substance is released from the tablet within 6 hours. This prevents the accumulation of high concentrations of iron on the gastrointestinal mucosa and supposedly avoids its damage. Although judging by the reviews, side effects when taking it are quite common.
Last time I asked you a question about ascorbic acid.
With its help, ferric iron turns into divalent iron, which is absorbed through the gastrointestinal mucosa. So why was it added to the ferrous iron preparation?
I told you above that ferrous iron contributes to the formation of a large number of free radicals, and I believe that ascorbic acid is added here as an antioxidant to neutralize them, although the manufacturer writes that it improves the absorption of iron.
I think that the need for ascorbic acid in the drug Sorbifer Durules is greatly exaggerated, otherwise it would be introduced into all ferrous iron preparations. But this is not the case.
Children - from 12 years old.
Pregnant and lactating women can.
How to take: 1 tablet. 1-2 times, i.e. 100-200 mg of iron per day.
Tardiferon
Release form: available in the form of film-coated tablets with prolonged release of the active substance.
The composition again contains ferrous sulfate.
Differences from the drug Sorbifer: a smaller dosage of pure iron in one tablet (80 mg versus 100 mg), so you will have to wait longer for the effect. No ascorbic acid.
Children - from 6 years old.
Pregnant and lactating women are allowed.
Standard therapeutic dosage for adults: 1-2 tablets. per day (80-160 mg of iron).
Totema
Release form: solution for oral administration. 1 ampoule - 50 mg of pure iron.
Why is the liquid form better?
The fact that the solution is more evenly distributed throughout the mucous membrane of the digestive tract, and the likelihood of irritation is reduced.
Secondly, this form is good for those who do not know how to swallow tablets, or for bedridden patients.
Another advantage of the drug Totema: it contains a safer iron salt - gluconate. The risk of side effects is less.
Fourthly, Totema contains copper and manganese, which improve iron absorption.
Children – from 3 months.
Pregnant women can.
Caution for patients with diabetes mellitus, because For taste, a lot of all sorts of chemical rubbish has been added to it. This is why I don't like liquid forms. In addition to the active and auxiliary substances necessary for stability, they contain all sorts of flavorings, dyes, sweeteners, etc., so the likelihood of allergic reactions is higher.
How to take: the contents of the ampoule should be dissolved in plain or sweetened water and drunk before meals. To treat IDA, take 1-2 ampoules 2 times a day. This is 100-200 mg of iron per day.
Fenyuls
Release form: capsules coated with a compound that forms a semi-permeable film of a certain thickness. This ensures a gradual release of iron.
If there are current instructions on the drug’s website, then it seems that this is the only iron supplement that can be dispensed without a doctor’s prescription.
But I wouldn't do it, and here's why.
Fenyuls contains ferrous sulfate and a number of vitamins (B1, B2, B6, PP, ascorbic acid, calcium pantothenate). All this, as the manufacturer claims, improves iron absorption and prevents the formation of free radicals.
But there are more side effects, since in addition to the side effects for iron, side effects for vitamins have been added: allergic reactions, dizziness, tachycardia, sweating, numbness of the extremities, an increase in the number of platelets, leukocytes, increased blood sugar levels, etc.
Maybe that's why the manufacturer is so careful with the recommended dosage? Pure iron in 1 capsule - 55 mg. Take 1-2 capsules per day. This dosage is more suitable for the prevention of anemia or the treatment of latent iron deficiency.
Contraindicated for children, allowed for pregnant and lactating women.
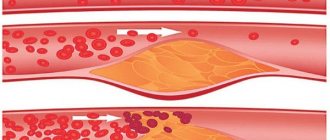
Why is there a shortage?
The most common cause is blood loss, for example due to injury or bowel disease, or due to excessive menstrual bleeding.
“Iron deficiency underlies more than half of anemia,”
says Ph.D.
cardiologist and nutritionist, GMS Clinic Natalya Polenova. “The main causes of iron deficiency: unbalanced diet, malabsorption, cyclic blood loss in women of reproductive age, donation, pregnancy, lactation, rapid growth during puberty.”
The second reason is poor absorption of iron. This can occur with medications, chronic bowel disease, inflammation, or genetic disorders.
A hematologist at the Federal State Budgetary Institution “National Medical Research Center of Hematology” of the Ministry of Health of Russia clarifies that iron deficiency conditions occur in many diseases with malabsorption, ranging from serious cancer to helminthiasis and the presence of Helicobacter pylori bacteria, which absorb iron.
Ferretab comp.
Release form: extended-release capsules.
It is interesting because each capsule contains three mini-tablets of iron (total 50 mg of pure iron) and one mini-tablet of folic acid in a good dosage (500 mcg).
See:
Abbreviation "comp." in the name of the drug means “complex”.
It is best recommended for anemia caused by deficiency of iron and folic acid, and for iron deficiency anemia in pregnant women or for the prevention of it.
Iron is represented by a safer salt than ferrous sulfate - fumarate. Gives fewer side effects.
How to take: on an empty stomach, 1 capsule (50 mg of iron) per day. If necessary, the doctor may increase the dosage to 2-3 capsules per day.
Conclusions:
ferrous preparations , I came to the following conclusions:
The safest drugs are Totema, Ferretab comp., because they do not contain ferrous sulfate, but other salts.
The most adequate dosages of iron for the treatment of IDA, in my opinion, are in the preparations Sorbifer Durules and Totema.
Ferric iron preparations
Benefits of ferric iron supplements
- Low toxicity. They cannot be overdosed.
- Better tolerated.
- They can be taken before, during, and after meals, without fear of inflammation or ulceration of the gastrointestinal mucosa.
- Fewer drug interactions.
- Fewer food interactions.
Disadvantages of ferric iron preparations
They act more slowly, so the treatment time increases.
If you need to quickly increase your iron level (surgery is coming up, severe anemia, etc.), at the beginning of treatment the doctor will most likely prescribe a ferrous iron supplement. In the future, he can transfer the patient to a ferric iron preparation if he does not tolerate divalent iron.
Let's look at the features of some popular drugs in this group.
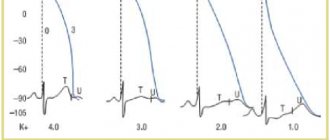
Indicators of normal iron metabolism
The most important indicator of red blood and iron levels, although indirect, but simple and important, is the concentration of hemoglobin. If it is lower than 130 g per liter for men, 120 g per liter for women, or 110 g per liter for pregnant women, then the condition is anemia. In the same case, if the hemoglobin level is less than 90 g/l, then the person should “automatically” go on sick leave, since he cannot work, especially hard work, physically, with such a hemoglobin concentration.
- Other direct indicators of iron metabolism are:
- ferritin blood plasma,
- transferrin,
- percentage of transferrin saturation with iron;
- free serum iron concentration.
We deliberately do not provide standards for men and women in order to save the reader from the temptation to replace seeing a doctor with various types of self-diagnosis. What are the symptoms and signs of iron deficiency anemia that can alarm a person and force him to go get tested?
Maltofer
Release forms for oral administration: drops, syrup, chewable tablets.
Main feature: iron hydroxide is combined with carbohydrates. This complex is called: “Iron hydroxide polymaltosate.” In articles and instructions it is referred to by the abbreviation HPC (hydroxide-polymaltose complex).
Its structure is similar to that of the natural iron compound ferritin. Thanks to this, it can connect with the transport protein, which delivers iron from the intestines to the blood.
GPC is stable. “pure” iron is not released into the gastrointestinal tract, and therefore there are significantly fewer adverse reactions when using it.
Pregnant and breastfeeding women can. Maltofer Fol will be optimal , which contains folic acid necessary for normal growth and development of the fetus.
Children: Maltofer drops, syrup - from birth, tablets - from 12 years.
Adverse reactions: nausea, constipation, diarrhea, dark stool, rash, itching, discoloration of tooth enamel.
Drug interactions - no.
There are no food interactions.
How to take: for the treatment of IDA, adults take 40-120 drops or 10-30 ml of syrup or 1-3 tablets per day. (100-300 mg pure iron) during or after meals. Chewable tablets can be swallowed as usual.
Maltofer in the form of drops or syrup can be mixed with fruit juice, vegetable puree, and milk mixture.
Ferrum Lek
Ferrum Lek used to be almost the only iron preparation for parenteral administration. There were no oral forms of it.
And now they are: syrup and chewable tablets.
Ferrum Lek is an analogue of the drug Maltofer in the form of syrup and chewable tablets. So, if something happens, they can replace Maltofer.
How to take: for adults to treat IDA, 10-30 ml of syrup (100-300 mg of iron) or 1-3 tablets per day during or after meals. After hemoglobin returns to normal, continue taking the drug 1 tablet until ferritin (iron reserves) normalizes.
Anemia risk groups
We have already indirectly mentioned some of the reasons for the development of anemia syndrome, such as bleeding, diseases of the stomach and intestines, and helminthic infestations. It should especially be remembered that children and pregnant women who have an increased need for iron form a risk group. Pregnant women need excess iron due to its high consumption for the construction of the baby's blood, children are actively growing, and women themselves, even those who are not pregnant, are also at risk, and specifically in reproductive age. After all, even normal menstrual bleeding is nothing more than “planned loss of iron.”
As soon as a newborn is born, the mother spends about 300 mg of iron during her pregnancy to build his body and synthesize his blood, using up her own reserves. And then, after birth, the baby's only source of iron will be mother's milk. Therefore, the lactation period, which begins immediately after pregnancy, is a continuation of the increased load on the woman’s body and increased iron consumption. If a child is fed on artificial formulas, then they must contain a certain amount of easily digestible iron.
The active period of construction of the child’s skeleton, elongation of the body requires an increase in its mass, and therefore the volume of circulating blood. And some mild signs of anemia, both laboratory and clinical, can occur in half of all children, but they are especially pronounced in girls. After all, in girls, during the period of active growth, the first menstruation, or menarche, begins, and then the loss of iron with menstruation becomes planned.
Ferlatum
Release form: solution for oral administration. 1 bottle contains 40 mg of pure iron.
Features of the composition: this is also a complex, only iron is in a complex not with carbohydrates, as in the previous case, but with protein. This prevents damage to the gastric mucosa.
Iron from this complex enters the blood from the intestines only thanks to carrier proteins, so an overdose is impossible. This means that there will be significantly fewer side effects than with treatment with ferrous iron preparations.
Adverse reactions: rarely - diarrhea, constipation, nausea, epigastric pain.
Drug interactions
- Reduces the absorption of tetracyclines.
- The absorption of iron increases if the drug is taken simultaneously with 200 mg of ascorbic acid. Keep it up! They ask Ferlatum, and you ask the buyer: “Did your doctor recommend you take ascorbic acid with it?” To be more convincing, you can show the instructions.
- Antacids reduce iron absorption.
Children, pregnant and lactating women are allowed. But it is better for pregnant women to take Ferlatum Fol , which contains a folic acid compound in the dispenser cap.
You need to remove the white cap from the bottle, press the red dispenser cap with your finger, and the powder with folic acid will pour into the bottle, and now the drug is ready for use.
How to take: standard dosage: 1-2 bottles per day before or after meals. This is 40-80 mg of pure iron. In my opinion, not enough.
The manufacturer does not say anything about its dilution, which means it is usually taken: drink it and wash it down with water. Has a cherry taste.
Friends, I draw your attention: I have indicated here the MEDICAL dosages of drugs. But they will be different if the drug is prescribed for latent iron deficiency or for prophylactic purposes.
Important to remember
- The causes of iron deficiency are blood loss, malabsorption, unbalanced diet, pregnancy, and helminthiasis.
- To identify a deficiency, you need to take a blood test for hemoglobin level, hematocrit, mean erythrocyte volume (MCV) and mean erythrocyte hemoglobin content (MCH).
- If there is no deficiency, then you should not take iron supplements. It may be dangerous.
- It is best to obtain iron from animal foods, in which it is in heme form.
- If you do not eat animal foods, you will need foods high in vitamin C to absorb plant non-heme iron.
How do iron supplements affect teeth?
Iron supplements can cause darkening of tooth enamel. This applies mainly to liquid forms (drops, syrup, oral solution) and chewable tablets.
Even if the instructions say that this drug does not stain tooth enamel, judging by the reviews of those who have taken iron supplements, sometimes it does.
Apparently, this is due to some characteristics of the microflora of the oral cavity or tooth enamel, because this does not happen to everyone.
Is it possible to avoid darkening of teeth while taking iron supplements?
Can. To do this, you need to follow several rules:
- Do not bite, dissolve, coated tablets, or keep them in your mouth.
- If a person has difficulty swallowing tablets or capsules and purchases chewable tablets, they should thoroughly rinse their mouth and brush their teeth after each dose.
- It is better to take drops, syrup, or oral solution through a straw and rinse your mouth after taking it.
- It is impossible to accomplish the previous point in small children, therefore you need to let the child drink the drug, preferably with a large amount of water, and then wrap a bandage around his finger, moisten it with clean boiled water and wipe his teeth.
Some of you asked:
“How do you solve the problem of teeth staining in chewable tablets?”
Please note that only complex iron preparations have the form of chewable tablets, because They are less likely than ordinary iron salts to cause staining of tooth enamel. Most likely, it is due to the different structure of the active substance, when iron is surrounded by either polysaccharides or protein.
Reviews for all iron preparations that we are talking about today, and almost all liquid forms or chewable tablets, in some cases cause staining of tooth enamel, with the exception of Ferlatum. If you heard that it also caused darkening of teeth in some of your customers, write about it in the comments.
You may also be asked:
“Do iron supplements destroy teeth?”
Judging by the reviews, children’s teeth sometimes get damaged from them, but I haven’t found any scientific evidence for this.
Perhaps it's all about the sweeteners that are included in the liquid forms, and not about the iron itself.
What questions should a buyer ask when selling iron supplements?
-Do you have any stomach or intestinal diseases? (and specify: gastritis, colitis, peptic ulcer?)
If there is, but the doctor still prescribed the drug, recommend taking it during or after meals, and if abdominal pain occurs, advise initially reducing the dosage and increasing it gradually. If the pain persists, let him see a doctor.
-What other medications are you taking?
We talked about drug interactions above, but it’s difficult to remember all this, so use the cheat sheets, which I hope you will download (download link at the end of the article).
These two questions are especially important to ask if the customer is prescribed ferrous iron.
I remind you once again that the iron supplement is taken until hemoglobin normalizes, plus another 1-3 months. The course of treatment for iron deficiency anemia is usually 3-6 months. The duration of the course depends on the severity of anemia, compliance with dosage recommendations, the presence or absence of diseases of the digestive tract, which may reduce the absorption of iron, and if we are talking about a ferrous iron preparation, on how the drug is taken: on an empty stomach or with food. Taking the drug during or after meals slows down the absorption of iron.
Basic principles of treating anemic syndrome without drugs
Naturally, the intensity of treatment for anemic syndrome, as we have already understood, depends on the causes. If this is bleeding and decay of tumor tissue, then emergency surgery is needed; if it is helminthiasis, then this is the prescription of anthelmintic drugs, but we will leave difficult situations for specialists. Let's consider a classic example of increased iron consumption in a pregnant woman, which must first be compensated for by dietary correction.
And if there are clinical, or even more so laboratory, signs of anemia, then you can no longer do without medications, but a diet can compensate for low-level iron deficiency, if we are simply talking about depletion of reserve reserves. On average, we receive about 20 mg of elemental iron every day with food, and about 10 times less is absorbed: 2 mg. And if you modify the diet, you can improve not only the supply of iron from food, but also its absorption, but not by more than 30%.
- Non-medicinal principles for treating iron deficiency using diet therapy and balanced nutrition are as follows:
- it is necessary to increase the intake of beef and fish liver, eggs and meat, natural products. Boiled, dietary meat is preferable rather than refined sausages;
- you should not rely on fresh apples as a legendary “source of iron”: no more than 5% of iron is absorbed from them,
- the presence of folic acid, vitamin C, or ascorbic acid, as well as copper in the diet increases the absorption of iron. This is precisely what the effect of complex iron-containing preparations, for example, Totems, which will be discussed later, is based on.
- Various tannins, such as tea tannin, oxalates, phosphates and calcium, reduce the availability of iron to the intestines and reduce its absorption. Therefore, regular consumption of strong tea can contribute to the occurrence of iron deficiency;
- If dairy products are consumed, they must be consumed separately from meat products, since milk contains calcium.
Which iron valence should you prefer? Both divalent and trivalent iron enter our body. But our body itself is well versed with these types of iron atoms, and oxidation and reduction processes occur with them in the body. As a result, the valency of the iron atoms changes. So, in order for iron to contact ferritin, it must have a valence of 3 plus, and hemoglobin contains divalent iron.