There are many reasons for the development of pancreatitis, and more often it is caused by a whole range of different reasons. The inflammatory process can develop with destruction, sclerosis and disruption of the trophism of pancreatic tissue, the appearance of pseudocysts, and calcification, which ultimately leads to disruption of its function. The severity of these disorders varies. The difficulty of diagnosing chronic pancreatitis is due to the frequent combination of damage to the pancreas and other digestive organs. Many patients with chronic pancreatitis are regarded as suffering from chronic alcohol intoxication, cholelithiasis, gastroduodenitis, duodenostasis, etc. The appearance of the classic “diagnostic triad” of symptoms: gland calcification, steatorrhea (fat in the stool) and diabetes mellitus is typical for advanced stages of the disease and therefore helps little in solving the problems of its early detection.
Statistical studies in recent decades indicate a clear increase in the number of patients with chronic pancreatitis in all countries of the world. The disease is most often detected in people aged 40 to 60 years. In Western European countries, the incidence of chronic pancreatitis ranges from 2 to 10 patients per 100 thousand population annually. In Russia, the authors show a wide range of statistical data: from 27.4 to 50 people per 100,000. It is important that everywhere in the world there is an increase in the incidence of acute and chronic pancreatitis, while the age of those who first became ill has decreased from 50 years to 39, and the number of sick women has increased by 30%. Up to 15-20% of patients die from acute pancreatitis or during exacerbation of chronic pancreatitis. In the United States, the mortality rate has doubled compared to the 90s of the last century.
Causes of development of chronic pancreatitis
Depending on the causes, primary
and
secondary
.
To understand the mechanism of development of pancreatitis, it should be noted that the pancreas constantly produces enzymes for better absorption of protein, fatty and carbohydrate foods (proteases, nucleases, lipase, amylase) - the excretory function of the gland. In total, about 1.5 liters of pancreatic juice are secreted per day. The enzymes produced in the gland are in an inactive state until they leave the pancreatic ducts and enter the duodenum. There, under the influence of food and bile, they become active and participate in the absorption of food.
Under some pathological conditions, enzyme activation occurs in the tissues of the pancreas itself. Its “self-digestion” begins, resulting in areas of necrosis and hemorrhage. Inflammation and swelling of the gland tissue occurs. Tissue breakdown products and enzymes enter the blood, poisoning the body. Intoxication affects all systems: cardiovascular, nervous, excretory, liver. Swelling of the small intestine, mesentery, etc. appears.
Beginning of primary
Pancreatitis is usually associated with processes in the pancreas itself, for example, after injury, alcohol abuse, impaired blood supply to the gland, some viral diseases, and narrowing of the main pancreatic duct, which impedes the outflow of enzymes that the gland excretes. It is also believed that primary pancreatitis can develop with a chronic lack of protein nutrition.
In diseases such as cholelithiasis, ulcerative, and diverticular diseases, the pancreas suffers secondarily. At the same time, joint coordinated work on food processing is disrupted. Swelling of the large duodenal papilla, duodenal dyskinesia and duodenostasis, stones in the bile ducts or inflammation in them contribute to the entry of bile, bacteria, emulsified fat into the pancreatic duct, or form a mechanical obstacle to the outflow of pancreatic juice, which leads to increased pressure and destruction walls of the pancreatic ducts. Both factors create conditions for premature activation of enzymes in its tissues, the development of inflammation, necrosis, and hemorrhages.
Chronic pancreatitis is considered to be a polyetiological disease.
The main etiological factors are:
- chronic alcoholism;
- cholelithiasis, choledocholithiasis;
- post-traumatic narrowing or obstruction of the pancreatic ducts;
- exposure to chemicals, including some medications;
- hyperlipidemia;
- insufficient protein nutrition (malnutrition);
- hereditary predisposition (L-antitrypsin deficiency and other genetic factors);
- hyperparathyroidism (hypercalcemia),
- cystic fibrosis (the most common factor in children),
- idiopathic factors.
Alcoholism is recognized as the most common cause of chronic pancreatitis. However, it is known that it occurs only in every 10th person who abuses alcohol. The average period for the development of chronic pancreatitis due to alcohol abuse is 18 years for men and 11 years for women. A typical combination of conditions in which its development actually occurs is good socio-economic living conditions of the patient (Western European countries, Japan, USA), male gender, age over 35 years, high level of daily fat intake, consumption of more than 20 g of alcoholic beverages daily ( in terms of pure ethyl alcohol).
Factors contributing to pancreatic damage include an unbalanced diet. Hereditary (familial) chronic pancreatitis is very rare. The first signs of it appear in children aged 10-12 years. Signs of congenital chronic pancreatitis, in addition to family history, are:
- the occurrence of pain in the upper abdomen in early childhood in the absence of other etiological factors;
- detection of pancreatic calcification;
- a sharp expansion of its ducts with the presence of stones in them.
A more frequent combination of chronic pancreatitis with blood group 0 (I) was noted.
Bile duct stones are a fairly common cause of pancreatitis in the population, mainly in women in Western Europe and North America. CP is combined with cholelithiasis very often, and the disease, caused by the presence of a chronic infection in the biliary tract, occurs in approximately 25% of patients with cholelithiasis. The main reason for the development of chronic pancreatitis in cholelithiasis is the emergence of conditions for the reflux of bile into the pancreatic duct:
- strangulation of a stone in the major papilla of the duodenum;
- trauma and prolonged spasm of the sphincter;
- papillitis or papillostenosis due to frequent injury to the papilla by small stones.
Sometimes the inflammatory process passes from the gallbladder and hepatic ducts directly to the pancreas through the venous and lymphatic vessels.
In diseases that occur with impaired liver function (cirrhosis or chronic hepatitis), bile is secreted, containing a large amount of free radicals and peroxide compounds, which, when entering the pancreatic ducts, themselves can cause an inflammatory reaction, but also stimulate pancreatic enzymes, promoting its “self-digestion”.
In addition, the cause of the development of secondary pancreatitis can be diseases of the duodenum, such as duodenitis, its diverticula and ulcerative deformity. In these diseases, as a result of inflammation or deformation in the duodenum, pressure increases, the function of the sphincter apparatus of the major papilla is disrupted, which is aggravated if a papillotomy was previously performed. Under such conditions, duodenal contents are thrown into the pancreas and bile ducts, pancreatic enzymes inside the gland tissue are activated, and the process of tissue destruction begins.
The development of chronic pancreatitis may be a direct consequence of perforation (penetration) of a gastroduodenal ulcer in the pancreas.
A number of drugs can have a damaging effect on the pancreas:
- corticosteroid drugs (“steroid pancreatitis”, “steroid diabetes”);
- ACTH;
- estrogens and estrogen-containing contraceptives;
- diuretics, etc. when taken for a long time.
Pancreatitis also develops with an overdose of drugs containing calcium and vitamin D. The use of chemotherapy drugs, metronidazole, nitrofurans in some cases leads to the development of chronic pancreatitis.
Disruption of arterial blood supply creates conditions for the formation of some forms of CP. If it develops in a young person aged 19 to 20 years and the cause cannot be determined, then this variant of the disease is called idiopathic.
Pathogenesis of the disease
Inflammatory phenomena in the pancreas gradually lead to degenerative changes in its structure, tissue sclerosis and obliteration of the ductal system. This process usually occurs in waves. The exacerbation is replaced by remission, instead of the glandular tissue that produces enzymes, connective tissue appears. Gradually, enzymes become insufficient; first of all, the exocrine function of the pancreas (production of digestive enzymes) decreases, and then the endocrine function (decreased insulin production).
Symptoms of pancreatic enzymatic insufficiency appear when normal pancreatic tissue is damaged by 90%.
Triad of symptoms of chronic pancreatitis
- pancreatic calcification;
- diabetes;
- steatorrhea is characteristic of an advanced stage of the disease. Steatorrhea occurs when lipase production by the pancreas falls below 16% of its normal level.
Impaired processing and absorption of nutrients in chronic pancreatitis leads to poor absorption of proteins, fats and vitamins. As a result, exhaustion, asthenia, and metabolic disorders of bone tissue and the blood coagulation system may develop.
Lack of secretion
Exocrine insufficiency is a decrease in the production of pancreatic juice. It is manifested by digestive disorders with “fatty” stools - steatorrhea. The stool volume is larger than the standard 200 grams, mushy or watery, almost like diarrhea. The surface of the feces is shiny, such stool is called “greasy.” There is not enough pancreatic juice for the normal processing of dietary fats, they are not absorbed, and this causes a person to lose weight, although the appetite does not suffer from insufficiency. All this may be accompanied by nausea, flatulence, and a feeling of rapid satiety with a small portion of food.
A quarter of patients in the late stages of CP develop endocrine insufficiency—a decrease in insulin production. A normal amount of insulin may be produced, but the gland's production of the hormone glucagon is greatly reduced, which causes hyperglycemia, when blood sugar levels rise sharply with tremors, profuse sweats, and even loss of consciousness. Another variant of insulin inadequacy may develop - pancreatic diabetes. This type of diabetes progresses aggressively, like type 1 diabetes in children.
In a third of patients, during an exacerbation of CP, the level of bilirubin increases, since the enlarged head of the pancreas compresses the bile duct, blocking bile in the liver, and there may even be obstructive jaundice.
Clinical manifestations of chronic pancreatitis
Manifestations of chronic pancreatitis depend on its form, stage, duration of development, complications encountered, and concomitant diseases.
The leading clinical symptom is pain. It occurs due to the development of increased pressure in the pancreatic ducts, or due to the development of pancreatitis-associated neuritis. The mechanisms of pain are described above, but it is worth noting that the spread of pain is associated with the involvement of the nerve plexuses, which are located between the lobules of the gland, in the inflammatory process, as well as pressure on them from the enlarged inflamed gland or pseudocysts.
Most often, at the beginning of the disease, the only complaint is pain above the navel
, it may bother you for several years. The pain is of a girdling nature, it can be debilitating, constant, or it can be paroxysmal and recurring. It can radiate to the back, to the left shoulder blade and shoulder, to the left side of the chest, and less often to the right. However, cases of pain radiating to the iliac and groin region, as well as to the genitals, have been described. The connection with food is of particular importance - pain appears after every meal, especially sour, spicy, salty, as well as those that stimulate bile secretion, for example, yolk, fat. Patients do not tolerate alcohol well.
Much later, digestion is disrupted: various dyspeptic disorders, steatorrhea, pancreatogenic diarrhea, insufficiency of intestinal absorption, malabsorption syndrome appear, which occurs due to insufficient production of enzymes in the pancreas. A person loses weight, becomes weaker, and calcifications appear in the pancreas. Little insulin is produced, which leads to secondary diabetes mellitus.
Our services
The administration of CELT JSC regularly updates the price list posted on the clinic’s website. However, in order to avoid possible misunderstandings, we ask you to clarify the cost of services by phone: +7
| Service name | Price in rubles |
| Ultrasound of the abdominal organs (liver, gall bladder, pancreas, spleen) | 3 800 |
| Pancreatocholangiography | 4 500 |
| MSCT of the abdominal cavity and retroperitoneal space of the abdomen | 6 000 |
All services
Make an appointment through the application or by calling +7 +7 We work every day:
- Monday—Friday: 8.00—20.00
- Saturday: 8.00–18.00
- Sunday is a day off
The nearest metro and MCC stations to the clinic:
- Highway of Enthusiasts or Perovo
- Partisan
- Enthusiast Highway
Driving directions
Diagnosis of chronic pancreatitis
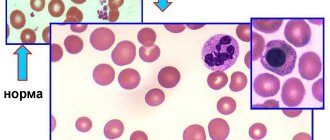
There is no need to rely on routine clinical laboratory tests for diagnosis. During the exacerbation phase of the disease, the number of leukocytes in the peripheral blood, as well as ESR, may be moderately increased, the level of albumin may be reduced and the level of gamma globulins may be slightly increased. However, this is not specific.
Comprehensive instrumental and laboratory studies are required. There are three stages during the examination:
- 1. Determination of signs of disease specifically in the pancreas, and not in other organs.
- 2. Exclusion of other pancreatic diseases, for example, malignant ones.
- 3. Search for the reasons that led to pancreatitis.
Laboratory extensive research:
- Blood test for the level of ALT, AST, alkaline phosphatase, bilirubin in the presence of jaundice.
- Blood and duodenal contents - to determine the level of pancreatic enzymes - amylase, trypsin, lipase.
- Coprological studies to determine creatorrhoea, steatorrhea, amilorrhea.
Study of exocrine function of the pancreas
There are direct and indirect methods. For the first, it is necessary to cannulate the main duct of the pancreas to obtain gland juice. However, its use is limited in medical practice, as it has many complications.
Indirect ones are preferable in this regard. This:
- The secretion of the gland is studied at rest and after physiological stimulants.
- It is important to study its digestive ability.
- Enzymes are studied in blood and urine.
An increase in amylase levels in the blood and urine indicates the presence of inflammatory phenomena in the pancreas. The increase in amylase levels in urine is more significant because the blood contains more salivary amylase, and the urine contains more pancreatic amylase, which has a smaller molecule than salivary amylase.
The method for determining pancreatic elastase in feces has high specificity and sensitivity. In chronic pancreatitis, the level of this enzyme decreases to 150 mcg/g, which is not observed in other diseases.
Radioimmunological testing of insulin, C-peptide, and glucagon is used.
It is important to determine blood and urine sugar - both on an empty stomach and during a carbohydrate load.
Instrumental diagnostic methods
Fibrogastroduodenoscopy
This study makes it possible to determine not only the condition of the gastric and intestinal mucosa, the condition of the duodenum and the areas of the major and minor papillae, to exclude erosions and ulcers, as well as tumors. Signs of papillitis or the presence of a parafaternal diverticulum and indirect symptoms of chronic pancreatitis, such as bulging and rigidity of the posterior wall of the stomach due to compacted enlarged PANCREAS, may be detected. Of particular value is the performance of targeted video duodenoscopy, an endoscopic examination that uses a special endoscope with lateral optics, which allows a good examination of the area of the large duodenal papilla.
Endosonography
A modern study that combines the capabilities of endoscopy and ultrasound diagnostics. This technique is most valuable for the differential diagnosis of pseudotumor pancreatitis and pancreatic cancer. In addition to visual examination with endosonography, it becomes possible to perform targeted fine-needle aspiration biopsy from the affected area.
Preventive measures
To avoid increased blood pressure during pancreatitis, it is recommended:
- Compliance with a dietary diet (exclusion from the menu of high-calorie, spicy and salty foods).
- Regularly engage in accessible sports and breathing exercises.
- Stay in the fresh air every day (at least 1 hour a day).
For patients with symptoms of pathology, it is equally important to quit smoking and get enough sleep. Avoid stress, minimize the consumption of alcohol, strong tonic drinks - coffee and black tea.