At the moment, there are many options for classification of coronary arteries adopted in different countries and centers of the world. But, in our opinion, there are certain terminological differences between them, which creates difficulties in the interpretation of coronary angiography data by specialists of different profiles.
We analyzed the literature on the anatomy and classification of the coronary arteries. Data from literary sources are compared with our own. A working classification of coronary arteries has been developed in accordance with the nomenclature accepted in the English-language literature.
Coronary arteries
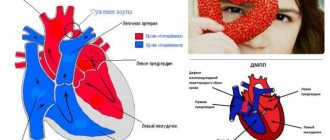
From an anatomical point of view, the coronary artery system is divided into two parts - right and left. From a surgical perspective, the coronary bed is divided into four parts: the left main coronary artery (trunk), the left anterior descending artery or anterior interventricular branch (LAD) and its branches, the left circumflex coronary artery (OC) and its branches, the right coronary artery (RCA). ) and its branches. The large coronary arteries form an arterial ring and loop around the heart. The left circumflex and right coronary arteries participate in the formation of the arterial ring, passing along the atrioventricular groove. The formation of the arterial loop of the heart involves the anterior descending artery from the left coronary artery system and the posterior descending artery from the right coronary artery system, or from the left coronary artery system - from the left circumflex artery with a left dominant type of blood supply. The arterial ring and loop are a functional device for the development of collateral circulation of the heart.
1.What is cardiac circulation and why measure it?
Blood supply or circulation of the heart (in professional parlance - perfusion) is the amount of blood in your heart. Blood flow to the heart is measured at rest and during exercise. The blood supply to the heart is often measured to determine the cause of chest pain. It can also be measured after a heart attack to determine which areas of the heart are not receiving blood.
Why measure heart circulation?
The blood supply to the heart is measured in order to:
- Find the cause of chest pain;
- Detect the location and severity of heart damage;
- Diagnose coronary heart disease or congenital heart defects;
- Monitor treatment for heart disease;
- Check the success of the operation.
A must read! Help with treatment and hospitalization!
Right coronary artery
The right coronary artery arises from the right sinus of Valsalva and runs in the coronary (atrioventricular) groove. In 50% of cases, immediately at the place of origin, it gives off the first branch - the branch of the arterial cone (conus artery, conus branch, CB), which feeds the infundibulum of the right ventricle. Its second branch is the sinoatrial node artery (SA node artery, SNA), which extends from the right coronary artery back at a right angle into the space between the aorta and the wall of the right atrium, and then along its wall to the sinoatrial node. As a branch of the right coronary artery, this artery is found in 59% of cases. In 38% of cases, the artery of the sinoatrial node is a branch of the left circumflex artery. And in 3% of cases there is blood supply to the sinoatrial node from two arteries (both from the right and from the circumflex). In the anterior part of the coronary sulcus, in the region of the acute edge of the heart, the right marginal branch (acute marginal artery, acute marginal branch, AMB), usually from one to three, departs from the right coronary artery, which in most cases reaches the apex of the heart. Then the artery turns back, lies in the back of the coronary sulcus and reaches the “cross” of the heart (the intersection of the posterior interventricular and atrioventricular sulcus of the heart). With the so-called right type of blood supply to the heart, observed in 90% of people, the right coronary artery gives off the posterior descending artery (PDA), which runs along the posterior interventricular groove at various distances, giving off branches to the septum (anastomosing with similar branches from the anterior descending artery, the latter usually longer than the first), the right ventricle and branches to the left ventricle. After the origin of the posterior descending artery (PDA), the RCA continues beyond the cross of the heart as the right posterior atrioventricular branch along the distal part of the left atrioventricular groove, ending in one or more posterolateral branches supplying the diaphragmatic surface of the left ventricle . On the posterior surface of the heart, immediately below the bifurcation, at the junction of the right coronary artery with the posterior interventricular groove, an arterial branch originates from it, which, piercing the interventricular septum, goes to the atrioventricular node - the atrioventricular node artery (AVN). The branches of the right coronary artery vascularize: the right atrium, part of the anterior wall, the entire posterior wall of the right ventricle, a small portion of the posterior wall of the left ventricle, the interatrial septum, the posterior third of the interventricular septum, the papillary muscles of the right ventricle and the posterior papillary muscle of the left ventricle.
Anatomy of the cardiovascular system
1. Right coronary artery 2. Anterior descending artery 3. Appendage 4. Superior vena cava 5. Inferior vena cava 6. Aorta 7. Pulmonary artery 8. Branches of the aorta 9. Right atrium 10. Right ventricle 11. Left atrium 12. Left ventricle 13. Trabeculae 14. Chordae 15. Tricuspid valve 16. Mitral valve 17. Pulmonary valve
In order to talk about diseases of the cardiovascular system, it is necessary to understand its structure. The circulatory system is divided into arterial and venous. Through the arterial system, blood flows from the heart, through the venous system it flows to the heart. There are large and small circles of blood circulation.
The great circle includes the aorta (ascending and descending, aortic arch, thoracic and abdominal sections), through which blood flows from the left side of the heart. From the aorta, blood enters the carotid arteries that supply blood to the brain, subclavian arteries, blood supply to the arms, renal arteries, arteries of the stomach, intestines, liver, spleen, pancreas, pelvic organs, iliac and femoral arteries, and blood supply to the legs. Blood flows from the internal organs through veins that drain into the superior vena cava (collects blood from the upper half of the body) and the inferior vena cava (collects blood from the lower half of the body). The vena cava drains into the right heart.
The pulmonary circulation includes the pulmonary artery (through which, however, venous blood flows). Through the pulmonary artery, blood enters the lungs, where it is enriched with oxygen and becomes arterial. Through the pulmonary veins (four), arterial blood enters the left heart.
The heart pumps blood - a hollow muscular organ consisting of four sections. These are the right atrium and right ventricle, which make up the right heart, and the left atrium and left ventricle, which make up the left heart. Oxygen-rich blood coming from the lungs through the pulmonary veins enters the left atrium, from there into the left ventricle and then into the aorta. Venous blood enters the right atrium through the superior and inferior vena cava, from there into the right ventricle and further through the pulmonary artery into the lungs, where it is enriched with oxygen and again enters the left atrium.
There are pericardium, myocardium and endocardium. The heart is located in the cardiac sac - the pericardium. Cardiac muscle - the myocardium consists of several layers of muscle fibers; there are more of them in the ventricles than in the atria. These fibers, contracting, push blood from the atria into the ventricles and from the ventricles into the vessels. The internal cavities of the heart and valves are lined by the endocardium.
Valve apparatus of the heart
Between the left atrium and the left ventricle there is a mitral (bicuspid) valve, and between the right atrium and the right ventricle there is a tricuspid (three-leaf) valve. The aortic valve is located between the left ventricle and the aorta, the pulmonary valve is between the pulmonary artery and the right ventricle.
Work of the heart
From the left and right atria, blood flows into the left and right ventricles, while the mitral and tricuspid valves are open, the aortic and pulmonary valves are closed. This phase in the work of the heart is called diastole. Then the mitral and tricuspid valves close, the ventricles contract and through the opened aortic and pulmonary valves, blood rushes into the aorta and pulmonary artery, respectively. This phase is called systole, systole is shorter than diastole.
Conduction system of the heart
We can say that the heart works autonomously - it itself generates an electrical impulse that spreads through the heart muscle, causing it to contract. The pulse must be generated at a certain frequency - normally about 50-80 pulses per minute. In the conduction system of the heart, the sinus node is distinguished (located in the right atrium), from which nerve fibers go to the atrioventricular (atrioventricular) node (located in the interventricular septum - the wall between the right and left ventricles). From the atrioventricular node, nerve fibers run in large bundles (right and left bundle branches), dividing into smaller bundles in the walls of the ventricles (Purkinje fibers). An electrical impulse is generated in the sinus node and spreads through the conduction system throughout the myocardium (heart muscle).
Blood supply to the heart
Like all organs, the heart must receive oxygen. Oxygen is delivered through arteries called coronary arteries. The coronary arteries (right and left) arise from the very beginning of the ascending aorta (at the origin of the aorta from the left ventricle). The trunk of the left coronary artery is divided into the descending artery (also known as the anterior interventricular) and the circumflex artery. These arteries give off branches - the artery of the obtuse edge, diagonal, etc. Sometimes the so-called median artery branches off from the trunk. The branches of the left coronary artery supply blood to the anterior wall of the left ventricle, most of the interventricular septum, the lateral wall of the left ventricle, and the left atrium. The right coronary artery supplies part of the right ventricle and the posterior wall of the left ventricle.
Now that you have become an expert in the anatomy of the cardiovascular system, let’s move on to its diseases.
Thromboembolism is blockage of blood vessels by blood clots. The most dangerous is thromboembolism of the pulmonary artery and its branches.
Peripheral arterial diseases:
- Arterial stenosis and occlusion
- Arterial aneurysms
- Raynaud's disease (syndrome)
- Peripheral venous diseases
- Peripheral vein thrombosis
- Phlebitis
- Varicose veins
Materials from the site www.cardioweb.ru
Left coronary artery
The left coronary artery starts from the left posterior surface of the aortic bulb and exits on the left side of the coronary sulcus. Its main trunk (left main coronary artery, LMCA) is usually short (0-10 mm, diameter varies from 3 to 6 mm) and is divided into the anterior interventricular (left anterior descending artery, LAD) and circumflex artery (LCx) branches . In 30-37% of cases, the third branch arises here - the intermediate artery (ramus intermedius, RI), which crosses obliquely the wall of the left ventricle. The LAD and OB form an angle between themselves that varies from 30 to 180°.
Anterior interventricular branch
The anterior interventricular branch is located in the anterior interventricular groove and goes to the apex, giving off the anterior ventricular branches (diagonal artery, D) and anterior septal branches along the way. In 90% of cases, one to three diagonal branches are determined. The septal branches depart from the anterior interventricular artery at an angle of approximately 90 degrees and pierce the interventricular septum, feeding it. The anterior interventricular branch sometimes enters the thickness of the myocardium and again lies in the groove and along it often reaches the apex of the heart, where in approximately 78% of people it turns posteriorly onto the diaphragmatic surface of the heart and at a short distance (10-15 mm) rises upward along the posterior interventricular groove. In such cases, it forms the posterior ascending branch. Here it often anastomoses with the terminal branches of the posterior interventricular artery, a branch of the right coronary artery.
2.How to prepare for measurement?
Before you have your heart's blood supply measured, tell your doctor:
- About taking any medications, including drugs to stimulate potency (Viagra);
- About allergies to any medications and anesthetics;
- About a possible or confirmed pregnancy;
- About the presence of infants.
Three hours before measuring the blood supply to the heart, you should not eat or drink. Avoid smoking, alcohol, and caffeinated drinks 24 hours before the test.
Visit our Cardiology page
Circumflex artery
The circumflex branch of the left coronary artery is located in the left part of the coronary sulcus and in 38% of cases gives the first branch to the artery of the sinoatrial node, and then the obtuse marginal artery (obtuse marginal branch, OMB), usually from one to three. These fundamentally important arteries supply the free wall of the left ventricle. In the case when there is a right type of blood supply, the circumflex branch gradually becomes thinner, giving off branches to the left ventricle. In the relatively rare left type (10% of cases), it reaches the level of the posterior interventricular groove and forms the posterior interventricular branch. In an even rarer case, the so-called mixed type, there are two posterior ventricular branches of the right coronary and circumflex arteries. The left circumflex artery forms important atrial branches, which include the left atrial circumflex artery (LAC) and the large anastomosing artery of the appendage. The branches of the left coronary artery vascularize the left atrium, the entire anterior and most of the posterior wall of the left ventricle, part of the anterior wall of the right ventricle, the anterior 2/3 of the interventricular septum and the anterior papillary muscle of the left ventricle.
Types of blood supply to the heart
The type of blood supply to the heart refers to the predominant distribution of the right and left coronary arteries on the posterior surface of the heart. The anatomical criterion for assessing the predominant type of distribution of the coronary arteries is the avascular zone on the posterior surface of the heart, formed by the intersection of the coronary and interventricular grooves - crux. Depending on which artery - right or left - reaches this zone, the predominant right or left type of blood supply to the heart is distinguished. The artery reaching this zone always gives off the posterior interventricular branch, which runs along the posterior interventricular groove towards the apex of the heart and supplies the posterior part of the interventricular septum. Another anatomical sign is described to determine the predominant type of blood supply. It has been noted that the branch to the atrioventricular node always arises from the predominant artery, i.e. from the artery that is most important in supplying blood to the posterior surface of the heart. Thus, with a predominant right type of blood supply to the heart, the right coronary artery supplies the right atrium, right ventricle, posterior part of the interventricular septum and posterior surface of the left ventricle. The right coronary artery is represented by a large trunk, and the left circumflex artery is poorly expressed. With the predominant left type of blood supply to the heart, the right coronary artery is narrow and ends in short branches on the diaphragmatic surface of the right ventricle, and the posterior surface of the left ventricle, the posterior part of the interventricular septum, the atrioventricular node and most of the posterior surface of the ventricle receive blood from the well-defined large left circumflex artery. In addition, a balanced type of blood supply is also distinguished, in which the right and left coronary arteries make approximately equal contributions to the blood supply to the posterior surface of the heart. The concept of “predominant type of blood supply to the heart,” although conditional, is based on the anatomical structure and distribution of the coronary arteries in the heart. Since the mass of the left ventricle is significantly greater than the right, and the left coronary artery always supplies most of the left ventricle, 2/3 of the interventricular septum and the wall of the right ventricle, it is clear that the left coronary artery is the predominant one in all normal hearts. Thus, with any type of coronary blood supply, the left coronary artery is predominant in a physiological sense. Nevertheless, the concept of “predominant type of blood supply to the heart” is valid, is used to assess anatomical findings during coronary angiography and is of great practical importance in determining indications for myocardial revascularization. For topical indication of lesion sites, it is proposed to divide the coronary bed into segments
The dotted lines in this diagram highlight the segments of the coronary arteries. Thus, in the left coronary artery in the anterior interventricular branch it is divided into three segments:
1. proximal - from the place of origin of the LAD from the trunk to the first septal perforator or 1DV. 2. average – from 1DV to 2DV. 3. distal – after departure of the 2DV.
It is also customary to distinguish three segments in the circumflex artery:
1. proximal - from the mouth of the OB to 1 VTK. 2. average - from 1 VTK to 3 VTK. 3. distal - after separation of the 3rd VTC.
The right coronary artery is divided into the following main segments:
1. proximal – from the mouth to 1 VOK 2. middle – from 1 VOK to the acute edge of the heart 3. distal – to the bifurcation of the RCA into the posterior descending and posterolateral arteries.
National Society for the Study of Atherosclerosis
In order to talk about diseases of the cardiovascular system, it is necessary to understand its structure. The circulatory system is divided into arterial and venous. Through the arterial system, blood flows from the heart, through the venous system it flows to the heart. There are large and small circles of blood circulation. The great circle includes the aorta (ascending and descending, aortic arch, thoracic and abdominal sections), through which blood flows from the left side of the heart. From the aorta, blood enters the carotid arteries that supply blood to the brain, subclavian arteries, blood supply to the arms, renal arteries, arteries of the stomach, intestines, liver, spleen, pancreas, pelvic organs, iliac and femoral arteries, and blood supply to the legs. Blood flows from the internal organs through veins that drain into the superior vena cava (collects blood from the upper half of the body) and the inferior vena cava (collects blood from the lower half of the body). The vena cava drains into the right heart. The pulmonary circulation includes the pulmonary artery (through which, however, venous blood flows). Through the pulmonary artery, blood enters the lungs, where it is enriched with oxygen and becomes arterial. Through the pulmonary veins (four), arterial blood enters the left heart.
The heart pumps blood - a hollow muscular organ consisting of four sections. These are the right atrium and right ventricle, which make up the right heart, and the left atrium and left ventricle, which make up the left heart. Oxygen-rich blood coming from the lungs through the pulmonary veins enters the left atrium, from there into the left ventricle and then into the aorta. Venous blood enters the right atrium through the superior and inferior vena cava, from there into the right ventricle and further through the pulmonary artery into the lungs, where it is enriched with oxygen and again enters the left atrium.
There are pericardium, myocardium and endocardium. The heart is located in the cardiac sac - the pericardium. Cardiac muscle - the myocardium consists of several layers of muscle fibers; there are more of them in the ventricles than in the atria. These fibers, contracting, push blood from the atria into the ventricles and from the ventricles into the vessels. The internal cavities of the heart and valves are lined by the endocardium.
- Right coronary artery
- Anterior descending artery
- Ear
- Superior vena cava
- Inferior vena cava
- Aorta
- Pulmonary artery
- Branches of the aorta
- Right atrium
- Right ventricle
- Left atrium
- Left ventricle
- Trabeculae
- Chords
- Tricuspid valve
- Mitral valve
- Pulmonary valve
Valve apparatus of the heart
Between the left atrium and the left ventricle there is a mitral (bicuspid) valve, and between the right atrium and the right ventricle there is a tricuspid (three-leaf) valve. The aortic valve is located between the left ventricle and the aorta, the pulmonary valve is between the pulmonary artery and the right ventricle.
Work of the heart
From the left and right atria, blood flows into the left and right ventricles, while the mitral and tricuspid valves are open, the aortic and pulmonary valves are closed. This phase in the work of the heart is called diastole. Then the mitral and tricuspid valves close, the ventricles contract and through the opened aortic and pulmonary valves, blood rushes into the aorta and pulmonary artery, respectively. This phase is called systole, systole is shorter than diastole.
Conduction system of the heart
We can say that the heart works autonomously - it itself generates an electrical impulse that spreads through the heart muscle, causing it to contract. The pulse must be generated at a certain frequency - normally about 50-80 pulses per minute. In the conduction system of the heart, the sinus node is distinguished (located in the right atrium), from which nerve fibers go to the atrioventricular (atrioventricular) node (located in the interventricular septum - the wall between the right and left ventricles). From the atrioventricular node, nerve fibers run in large bundles (right and left bundle branches), dividing into smaller bundles in the walls of the ventricles (Purkinje fibers). An electrical impulse is generated in the sinus node and spreads through the conduction system throughout the myocardium (heart muscle).
Blood supply to the heart.
Like all organs, the heart must receive oxygen. Oxygen is delivered through arteries called coronary arteries. The coronary arteries (right and left) arise from the very beginning of the ascending aorta (at the origin of the aorta from the left ventricle). The trunk of the left coronary artery is divided into the descending artery (also known as the anterior interventricular) and the circumflex artery. These arteries give off branches - the artery of the obtuse edge, diagonal, etc. Sometimes the so-called median artery branches off from the trunk. The branches of the left coronary artery supply blood to the anterior wall of the left ventricle, most of the interventricular septum, the lateral wall of the left ventricle, and the left atrium. The right coronary artery supplies part of the right ventricle and the posterior wall of the left ventricle.
Now that you have become an expert in the anatomy of the cardiovascular system, let’s move on to its diseases.
Coronary heart disease (CHD)
The basis of coronary heart disease is an insufficient supply of oxygen to the heart muscle. That is, there is a discrepancy between demand and delivery. The most common cause of IHD is atherosclerosis of the coronary arteries. An atherosclerotic plaque forms inside the coronary artery, which closes its lumen. With increased stress (physical, psychological stress), the heart requires more oxygen, but its delivery is limited due to partial stenosis (blockage) of the coronary artery. Therefore, the main symptom of angina pectoris is retrosternal (squeezing, pressing) pain during physical activity. The duration of pain is from seconds to minutes (no more than 30 minutes). The pain is usually relieved with nitrates (nitroglycerin). To make a diagnosis of angina, an ECG, stress tests, ECHO CG, 24-hour ECG monitoring, myocardial perfusion scintigraphy, and coronary ventriculography are performed. Angina is divided into stable (angina pectoris, angina at rest) and unstable (progressive, first occurring). A special form of angina is vasospastic (Prince-Menthol), which occurs due to spasm of the coronary arteries. There are three main ways to treat angina - medications (nitrates, b-blockers, angiotensin converting enzyme inhibitors, etc.), balloon angioplasty and coronary artery bypass surgery.
Myocardial infarction
- necrosis (death) of a section of the heart muscle. The causes of myocardial infarction are the same as angina pectoris. The main symptom is prolonged chest pain (more than 30 minutes), which is not relieved by nitrates. The diagnosis of myocardial infarction is made based on the clinical picture, characteristic ECG changes and elevated blood enzyme levels. Treatment is medication (aimed at relieving pain, reducing blood oxygen demand, dilating the coronary arteries); in some cases, within a few hours of the development of a heart attack, it is possible to dissolve a blood clot by administering special drugs (streptokinase, urokinase, etc.). Emergency balloon angioplasty is sometimes performed.
As a result of a myocardial infarction, or due to other diseases (myocarditis), the muscle tissue of the heart is replaced by connective tissue, that is, a scar is formed. Scar changes in the myocardium are called cardiosclerosis .
Disorders of cardiac rhythm and conduction.
Classification
Change in sinus node automaticity:
- sinus bradycardia (slow heart rate),
- sinus tachycardia (accelerated rhythm),
- sinus arrhythmia (irregular rhythm)
Escape rhythms Atrioventricular dissociation Atrial tachycardias Atrioventricular reciprocal tachycardias Ventricular tachycardia Ventricular fibrillation Ventricular preexcitation Sinus node weakness Blocks:
- Sinoatrial
- Atrioventricular
- Bundle branch blocks
Atrial fibrillation and flutter Parasystole
Since it is quite difficult to explain to a non-specialist the essence of these violations, we will decipher only the basic concepts. Extrasystole is an extraordinary contraction of the heart. A distinction is made between atrial extrasystoles (“incorrect” impulse occurs in the atria) and ventricular extrasystoles (“incorrect” impulse occurs in the ventricles). The patient perceives extrasystoles as pauses in the work of the heart. In healthy people, a small amount of extrasitol is recorded per day. Atrial fibrillation (atrial fibrillation) is frequent, chaotic, irregular contraction of the atria and irregular ventricular rhythm. The main causes of atrial fibrillation are damage to the mitral valve, thyrotoxicosis (pathology of the thyroid gland), and cardiosclerosis.
To treat rhythm disturbances, there are several groups of antiarrhythmic drugs; in some cases, pathological foci or nerve pathways are destroyed.
Conduction disorders - delay in the conduction of impulses through the conduction system of the heart - blockade, or vice versa, accelerated conduction of the impulse along additional conduction pathways. Conduction delay is a block; there are sinoauricular, atrioventricular, and bundle branch blocks. Accelerated conduction - WPW (Wolf-Parkinson-White) syndrome is more common.
Hypertonic disease.
The main manifestation of hypertension (HD) is increased blood pressure (BP). This is often manifested by headaches, tinnitus, and flickering of “spots” before the eyes. Hypertension is divided into two large groups - essential (primary) and symptomatic (secondary) hypertension. Essential hypertension is a disease at the level of the whole organism. With secondary hypertension, there is damage to one or another organ, which leads to an increase in blood pressure. Secondary hypertension is divided into renal (glomerulonephritis, pyelonephritis, renovascular hypertension, etc.), endocrine (pheochromocytoma, paraganglioma, Cohn syndrome, Itsenko-Cushing syndrome), vascular (coarthation of the aorta), hypertension with damage to the central nervous system.
When blood pressure increases, changes occur in various organs. The organs most susceptible to the effects of high blood pressure are called target organs. These are the brain, heart, blood vessels, retina, kidneys.
When treating symptomatic hypertension, it is important to eliminate the cause of the increase in blood pressure. The main antihypertensive drugs are b-blockers, angiotensin converting enzyme inhibitors (ACEIs), calcium antagonists, and diuretics.
Heart defects
Heart defects are divided into congenital and acquired. There are quite a large number of names that are congenital; we will not list them all; we will pay attention to the most common ones. These are patent oval window (ventricular septal defect), atrial septal defect, tetralogy and Fallot's triad. Treatment is surgical. Mitral valve prolapse is insufficiency of the mitral valve caused by the “bending” of its valves into the cavity of the left atrium during contraction (systole) of the left ventricle. The reason is connective tissue disorders.
Acquired defects include stenosis (incomplete opening) or insufficiency (incomplete closure) of the heart valves. Stenosis or insufficiency of the mitral and tricuspid valves are more common. The cause of the lesion is rheumatism, endocarditis, atherosclerosis, etc. Treatment is surgical, in the acute phase - antibiotic therapy, hormones, cytostatics, etc.
Primary damage to the heart muscle
Myocarditis Endocarditis Pericarditis Cardiomyopathies
- Dilatational
- Hypertrophic
- Restrictive
Myocarditis is an inflammation of the heart muscle, it can be bacterial, viral, or allergic. This is a rather “complex” disease, since an autoimmune reaction is triggered - antibodies are produced to one’s own muscle. Treatment: antibiotics, hormonal drugs, hydroxyquinolines. Endocarditis is inflammation of the endocardium, often bacterial. Ultimately leads to damage to the heart valves. Treatment: antibiotics, hormones.
Dilated cardiomyopathy is a lesion of the heart muscle, which causes expansion of the heart (enlargement of cavities) and thinning of its walls. The heart's ability to pump blood decreases. The reason is not fully understood. The main manifestation is the occurrence of circulatory failure - shortness of breath, swelling, enlarged liver, attacks of suffocation. Weakness, cardiac arrhythmias, and thromboembolism are common.
Hypertrophic cardiomyopathy is a thickening of the heart muscle, resulting in difficulty ejecting blood from the left ventricle. The reason is not fully understood. The main manifestation is rhythm and conduction disturbances, pain in the heart, weakness.
Restrictive cardiomyopathy is a reduction in the chambers of the heart.
Cor pulmonale is an overload of the heart that occurs due to increased resistance in the vessels of the lungs. The reason for this is primary pulmonary hypertension (primary damage to the blood vessels of the lungs), chronic pulmonary diseases (pneumosclerosis, emphysema, bronchiectasis, bronchitis, etc.) and anatomical changes in the chest. Thromboembolism is blockage of blood vessels by blood clots. The most dangerous is thromboembolism of the pulmonary artery and its branches.
Peripheral arterial diseases:
- Arterial stenosis and occlusion
- Arterial aneurysms
- Raynaud's disease (syndrome)
- Peripheral venous diseases
- Peripheral vein thrombosis
- Phlebitis
- Varicose veins
Coronary angiography
Coronary angiography (coronary angiography) is x-ray visualization of the coronary vessels after the injection of a radiopaque contrast agent. The X-ray image is simultaneously recorded on 35 mm film or digital media for subsequent analysis. At the moment, coronary angiography is the “gold standard” for determining the presence or absence of stenoses in coronary disease. The purpose of coronary angiography is to determine the coronary anatomy and the degree of narrowing of the lumen of the coronary arteries. Information obtained during the procedure includes determination of the location, extent, diameter and contours of the coronary arteries, the presence and degree of coronary obstruction, characterization of the nature of the obstruction (including the presence of atherosclerotic plaque, thrombus, dissection, spasm or myocardial bridge). The data obtained determine the further tactics of treating the patient: coronary bypass surgery, intervention, drug therapy. To conduct high-quality angiography, selective catheterization of the right and left coronary arteries is necessary, for which a large variety of diagnostic catheters of various modifications have been created. The examination is carried out under local anesthesia and NLA through arterial access. The following arterial approaches are generally accepted: femoral arteries, brachial arteries, radial arteries. Transradial access has recently gained a strong position and has become widely used due to its low morbidity and convenience. After puncture of the artery, diagnostic catheters are inserted through the introducer, followed by selective catheterization of the coronary vessels. The contrast agent is administered in doses using an automatic injector. Filming is performed in standard projections, the catheters and intravener are removed, and a compression bandage is applied.
4.What are the risks and what could interfere with the test?
What are the risks of the test?
Measuring cardiac circulation is a safe procedure. Possible problems may arise due to physical activity and depend on the general condition of the body. Complications after the test:
- Fainting;
- Arrhythmia;
- Chest pain;
- Heart attack.
What can interfere with the test?
Measurement of cardiac circulation may be interfered with by:
- Recently suffered a severe heart attack;
- Inflammation of the heart - sarcoidosis and myocarditis;
- Cardiac contusion;
- Weakening of the heart muscles;
- Myocardial fibrosis;
- Severely narrowed heart valve;
- Pacemakers and other implanted devices;
- Diseases that do not allow the body to be exposed to physical activity: arthritis, lung diseases and others;
- Taking such drugs as dipyridamole or pentoxifylline;
- Serious electrolyte imbalance;
- Pregnancy or breastfeeding.
Basic angiographic projections
When carrying out the procedure, the goal is to obtain the most complete information about the anatomy of the coronary arteries, their morphological characteristics, the presence of changes in the vessels with an accurate determination of the location and nature of the lesions. To achieve this goal, coronary angiography of the right and left coronary arteries is performed in standard projections. (They are described below). If it is necessary to conduct a more detailed study, shooting is carried out in special projections. This or that projection is optimal for analyzing a certain section of the coronary bed and allows the most accurate identification of morphological features and the presence of pathology of a given segment. Below are the main angiographic projections indicating the arteries for which these projections are optimal for visualization. For the left coronary artery, the following standard projections exist. 1. Right anterior oblique with caudal angulation. RAO 30, caudal 25. OV, VTK,
2. Right anterior oblique projection with cranial angulation. RAO 30, cranial 20 LAD, its septal and diagonal branches
3. Left anterior oblique with cranial angulation. LAO 60, cranial 20. The mouth and distal portion of the LCA trunk, the middle and distal segment of the LAD, septal and diagonal branches, the proximal segment of the OB, the VTK.
4. Left anterior oblique with caudal angulation (spider). LAO 60, caudal 25. LCA trunk and proximal segments of the LAD and OB.
5. To determine the anatomical relationships, a left lateral projection is performed. For the right coronary artery, surveys are performed in the following standard projections. 1. Left oblique projection without angulation. LAO 60, stright. Proximal and middle segment of the RCA, VOC.
2. Left oblique with cranial angulation. LAO 60, cranial 25. The middle segment of the RCA and the posterior descending artery.
3. Right oblique without angulation. RAO 30, stright. Middle segment of the RCA, branch of the conus arteriosus, posterior descending artery.
Professor, Doctor of Medicine. Sciences Yu.P. Ostrovsky