pharmachologic effect
Pharmacological action - antianginal, antihypertensive.
Blocks the flow of calcium ions through membranes into the smooth muscle cells of the myocardium and blood vessels (calcium channels). Vasodilation leads to a decrease in blood pressure. The antianginal effect is due to both a decrease in oxygen consumption, due to the dilation of arterioles and a decrease in peripheral vascular resistance (afterload), and an increase in oxygen delivery due to dilatation of the main coronary arteries and arterioles in ischemic and unchanged areas of the myocardium.
Indications for the drug Vero-Amlodipine
Arterial hypertension (first-line drug for monotherapy or in combination with other antihypertensive drugs), stable angina, vasospastic angina (Prinzmetal's angina, or variant angina), vasospasm/vasoconstriction, dilated (non-ischemic) cardiomyopathy with severe chronic heart failure (III- Stage IV), as well as patients refractory to treatment with nitrates or beta-blockers (monotherapy or in combination with other antianginal drugs).
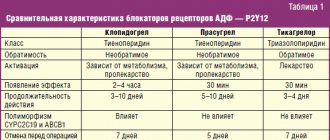
Amlodipine: review of clinical studies
Amlodipine is a third-generation dihydropyridine calcium channel antagonist that blocks slow calcium channels (L-type channels) and prevents intracellular hypercalcemia and smooth muscle cell contraction, exerting a vasodilatory effect. Amlodipine has a long-lasting effect, which allows it to be used once a day. Amlodipine effectively lowers blood pressure without affecting heart rate in patients with arterial hypertension. It is also used in the treatment of patients with angina pectoris, including effective in cases of pronounced vasospastic component of ischemia. The drug is well tolerated, causing few side effects. Used in combination with other antianginal and antihypertensive drugs.
Pharmacokinetics
When taken orally, amlodipine is slowly and almost completely absorbed from the gastrointestinal tract, regardless of food intake. The bioavailability of amlodipine is high and ranges from 60 to 80%. The volume of distribution of the drug is on average 20-21 l/kg body weight, which is significantly more than that of other representatives of the dihydropyridine series. In serum, 95-98% of the drug dose is bound to plasma proteins. The maximum concentration of amlodipine in the blood is achieved 6-12 hours after administration. The duration of action of the drug is due to its slow release from connection with receptors.
Table 1. Effect of amlodipine on blood pressure and heart rate
| Heart rate | Adverse reactions | ||||||
| Frishman WH et al., 1989 [1] | R, DS, PC | 123 | 5-10 mg | 8 weeks | ↓sBP by 12.8 ↓dBP by 10.1 | Not edited | |
| Horwitz LD et al., 1997 [2] | R, MC, PS, PG | 123 | 5-10 mg | 10 weeks | ↓sBP by 13.1 ↓dBP by 12.2 | Not edited | |
| Lorimer AR et al., 1989 [3] | DS, PC, PG | 106 | 5 mg | 12 weeks | ↓sBP by 11.9 ↓dBP | Well tolerated | |
| Lau et al., 1996 [4] | R, DS, Per | 65 | 5 mg | ↓sBP by 22.3 ↓dBP by 12.3 | Well tolerated | ||
| Habeler G. et al., 1992 [5] | Open, non-comparative | 62 | 5-10 mg | 27 months | ↓sBP by 30.5 ↓dBP by 20.7 | Not edited | Well tolerated |
| Ajayi AA et al., 1995 [6] | R, PS, PG | 20 | 5-10 mg | 2-4-6 weeks | ↓BP from 190/104 to 150/79 | Not edited | Well tolerated |
| Sethi KK et al., 1994 [7] | PS, PC | 20 | 4 weeks | ↓sBP at 32 ↓dBP at 22 | Not edited | ||
| Khokhani RC et al., 1993 [8] | Open, non-comparative | 20 | 5-10 mg | 4 weeks | ↓BP from 162/100 to 139/85 | Not edited | Well tolerated |
| Broadhurst P. et al., 1992 [9] | 11 | 5-10 mg | 6 weeks | ↓BP from 169/104 to 146/92 | Not edited | Well tolerated |
Note: R - randomized, PS - single blind, DS - 'double' blind, PC - placebo-controlled, PG - parallel groups, Per - crossover, MC - multicenter, SBP - systolic blood pressure, DBP - diastolic blood pressure.
The biotransformation of amlodipine to inactive metabolites occurs in the liver. The drug is excreted in the urine (about 10% unchanged and about 60% in the form of inactive metabolites) and in feces. The half-life of amlodipine is 35-50 hours. A stable equilibrium concentration (steady-state) is achieved after 7-8 days of taking the drug. With impaired liver function, the elimination time of amlodipine increases, which is also typical for other dihydropyridine calcium antagonists. When taking amlodipine, there is no impairment of glucose tolerance, so the drug can be used in patients with diabetes mellitus, as well as bronchial asthma and gout.
Pharmacodynamics Effect on blood pressure and heart rate
In table Table 1 shows the effect of amlodipine on the level of systolic and diastolic blood pressure, heart rate and the occurrence of adverse reactions when using the drug.
The effect of amlodipine (in the form of blocking slow calcium channels and reducing intracellular hypercalcemia) is 80 times more pronounced in relation to vascular smooth muscle cells compared to contractile myocardium. Thus, the decrease in blood pressure under the influence of amlodipine occurs precisely due to peripheral vasodilation. Amlodipine has a pronounced hypotensive effect on both systolic and diastolic blood pressure. However, the degree of reduction in blood pressure varies, according to different authors. Thus, in a study by Horwitz LD et al. [2] when using 5-10 mg of amlodipine for 10 weeks. the decrease in systolic pressure was 13.1 mm Hg. Art., diastolic - 12.2 mm Hg. Art., and in the study by Habeler G. et al. [5] when using the same dose of amlodipine for 27 months. systolic blood pressure decreased by 30.5 mmHg. Art., and the decrease in diastolic was 20.7 mm Hg. Art.
Amlodipine has a long-term hypotensive effect due to its long half-life (35-50 hours), which allows it to control blood pressure evenly throughout the day. This leads to a relatively greater effectiveness of the drug in controlling the early morning rise in blood pressure, regardless of the time of administration (morning or evening once a day) [10, 11, 12]. In a study by Leenen FH et al. during a break in treatment, blood pressure remained within normal limits even on the second day of drug withdrawal [13]. The maximum hypotensive effect during therapy with 5 mg of amlodipine occurs only at the 6th week. use of the drug, which makes early dose increases inappropriate in case of incomplete control of blood pressure levels [14]. The drug has a dose-dependent effect on blood pressure levels and is characterized by a linear dose-concentration relationship in the blood plasma. Thus, in a study on healthy volunteers, diastolic blood pressure decreased when measured while standing by 1.1; 4.8 and 8.0 mm Hg. Art., when using 2.5; 5 and 10 mg of amlodipine, respectively [15].
With the development of the hypotensive effect of amlodipine, there is no change in heart rate, which sets the drug apart from other representatives of the dihydropyridine series. In addition, the drug is well tolerated by patients (Table 1). Side effects include the possibility of developing swelling of the legs and hyperemia, which is typical for all drugs of the dihydropyridine series.
Effect on myocardial ischemia
The antianginal effect is determined by the peculiarity of the mechanism of action and is due to the coronary-lytic effect of the drug, which also determines the most preferable patient population. The effect of the drug is maximum in patients with a pronounced spastic component of coronary obstruction [17]. However, amlodipine is also widely used for the treatment of stable angina pectoris, significantly reducing the frequency, duration and severity of ischemic episodes [18-22]. One of the possible beneficial protective effects of amlodipine on the state of the myocardium after an episode of ischemia is considered to be its ability to reduce calcium overload of cells, which is the cause of myocardial damage [23]. An advantageous difference between amlodipine and earlier calcium antagonists is its lack of influence on heart rate, an increase in which during physical activity is one of the triggers for ischemia.
Table 2. Changes in echocardiographic parameters in groups after 12 months. treatment in the TOMHS study
| Amlodipine | Chlorthalidone | Doxazosin | Enalapril | All drugs | Placebo | ||
| MZhP, mm | -0.2 | -0.6 | -0.6 | -0.8 | -0.5 | -0.5 | -0.3 |
| ZS, mm | -1.0 | -1.0 | -0.9 | -0.7 | -0.7 | -0.9 | -0.7 |
| OLZh, mm3 | 0.5 | -0.3 | -1.6 | 0.3 | 0.1 | -0.2 | -0.2 |
| LV iML, g/m2 | -5.9 | -11.2 | -15.6 | -9.5 | -6.2 | -9.7 | -6.9 |
| LV iML, g/m | -9.5 | -15.5 | -20.6 | -12.9 | -10.2 | -13.8 | -1.6 |
| Lifespan, % | -3.0 | -2.8 | -1.7 | -3.2 | -2.7 | -2.7 | -1.6 |
| Number of patients | 103 | 100 | 111 | 113 | 105 | 532 | 186 |
Note: IVS - interventricular septum, WS - thickness of the posterior wall of the left ventricle, LV - internal volume of the left ventricle, iMLV - left ventricular myocardial mass index (based on body surface area and height), RV - right ventricle.
Table 3. Changes in selected parameters in groups after treatment in the TOMHS study
Indicators
| Acebutolol | Amlodipine | Chlorthalidone | Doxazosin | Enalapril | All drugs | Placebo | |
| Na excretion in urine, mmol/8 h | -10.5 | -9.4 | -11.6 | -6.1 | -12.8 | -10.1 | -10.6 |
| Physical activity points | +111 | +99 | +92 | +116 | +88 | +101 | +73 |
| ↓dBP, mm Hg. Art. | -13.1 | -12.9 | -12.3 | -11.7 | -11.5 | -12.3 | -8.6 |
| ↓sBP, mm Hg. Art. | 17.0 | -15.6 | -17.7 | -14.2 | -14.7 | -15.9 | -9.1 |
| Change Heart rate, beats/min | -9.8 | -1.8 | -2.9 | -1.8 | -2.9 | -3.9 | -2.3 |
The CAPE study [16] assessed the effect of amlodipine on the duration and frequency of myocardial ischemic episodes in patients with coronary artery disease. During the control 48-hour ECG monitoring, a decrease in the number of ischemic episodes was observed. When assessing the possible proarrhythmogenic effect of the drug in patients with stable angina pectoris, when amlodipine was added to traditional therapy with β-blockers and nitrates, no increase in episodes of arrhythmia was observed.
Effect on the autonomic nervous system
Activation of the sympathetic component of the autonomic nervous system is an undesirable side effect of dihydropyridine calcium antagonists due to their mechanism of action (reflex activation). At the same time, a study of norepinephrine in the blood of patients taking amlodipine did not show changes in its level compared to the baseline [24-26]. During spectral analysis, no increase in LF/HF was observed [27]. Thus, a feature of the action of amlodipine is the absence of activation of the sympathetic nervous system and the development of reflex tachycardia.
Effect on plasma renin activity
Susaguri et al. [28] studied plasma renin activity and norepinephrine levels in patients with arterial hypertension when prescribed amlodipine. The study was conducted 1, 4 and 7 days after the start of therapy. As a result, in response to a decrease in blood pressure when prescribing amlodipine, no activation of the sympathetic nervous and renin-angiotensin systems was observed, and the levels of norepinephrine and plasma renin remained unchanged.
Effect on left ventricular myocardial mass
The randomized, double-blind, placebo-controlled TOMHS (Treatment of mild hypertension study) study compared 5 antihypertensive drugs: a diuretic (chlorthalidone), a β-blocker (acebutolol), a calcium channel antagonist (amlodipine), an angiotensin-converting enzyme inhibitor (enalapril maleate) , an α-adrenergic receptor antagonist (doxazosin) and their possible effect on the mass of the left ventricular myocardium. The study was based on a proven connection between an increase in the size of the left ventricle and an increased risk of developing cardiovascular complications. The study followed 902 patients with mild hypertension over a period of more than four years. At the first stage, patients were offered one of 5 antihypertensive drugs (including amlodipine at a dose of 5 mg/day) or placebo, and then at the second stage, if blood pressure control was inadequate, a second drug was added (chlorthalidone in 5 groups of patients and enalapril in the group previously receiving chlorthalidone). All drugs were prescribed once a day in the morning. Control echocardiographic studies were carried out at baseline, 3, 12, 24, 36 and 48 months. During the study, a significant decrease in blood pressure levels was observed, and in the acebutolol and amlodipine groups the percentage of changes in therapy was the smallest, i.e. Adequate blood pressure control was observed throughout the entire four-year observation period at doses of drugs not exceeding the initial ones. When studying the dynamics of changes in left ventricular myocardial mass, it turned out that the most pronounced decrease was observed in the amlodipine and chlorthalidone groups, compared with the acebutolol and placebo groups. During the entire observation, it turned out that amlodipine reduces the mass of the left ventricular myocardium, which may reduce the risk of developing cardiovascular complications in patients with arterial hypertension and left ventricular hypertrophy (Tables 2, 3).
Effect on the progression of vascular atherosclerosis
Due to the presence of a number of reports on the possible beneficial effects of calcium antagonists on the condition of the vascular endothelium, a multicenter, prospective, randomized, double-blind, placebo-controlled PREVENT study was conducted [48]. This study assessed changes in the degree of atherosclerotic lesions of the coronary arteries and the thickness of the intimomedial layer of the carotid arteries during the administration of amlodipine. The study was conducted on 825 patients with coronary artery disease confirmed by coronary angiography. Patients received amlodipine at a dose of 5 mg, which, if well tolerated, was increased to 10 mg. As a result of the study, no significant differences were obtained in both study groups - active treatment and control - in relation to the progression of atherosclerotic stenosis of the coronary vessels. On the contrary, there was a pronounced effect of amlodipine on the progression of atherosclerosis in the carotid arteries, detected using ultrasonography. At the same time, in the amlodipine group, regression of the intima-medial layer was observed by 0.046 mm, and in the control group, thickening by 0.011 mm. Currently, a correlation has been proven between the degree of thickening of the intima-medial layer of the carotid arteries and the incidence of myocardial infarction and cerebral stroke. Also, the PREVENT study showed good tolerability of the drug, which was previously noted by other researchers, with the frequency of adverse reactions comparable to the placebo group (79% for amlodipine and 83% for placebo). Additional prescription of angiotensin-converting enzyme inhibitors in the amlodipine group was observed half as often as in the placebo group.
Clinical application Arterial hypertension
Amlodipine effectively reduces systolic and diastolic blood pressure levels both in monotherapy and as part of combination therapy (Table 1). Amlodipine is a competitive drug when compared with other calcium antagonists and drugs from other classes of antihypertensive drugs (Table 4).
When comparing the effect of amlodipine with the effect of other calcium antagonists, its greater effectiveness in relation to blood pressure levels is shown in comparison with verapamil and diltiazem. Thus, in a study by Watts RW et al. [35] compared amlodipine (5-10 mg) and controlled-release diltiazem (180-360 mg), and mean daily blood pressure decreased with amlodipine to 137/84 mmHg. Art., and when using diltiazem - up to 143/86 mm Hg. Art. According to Lorimer AR et al. When compared with verapamil, amlodipine controlled blood pressure better within 24 hours after the last dose than verapamil within 12 hours after the last dose [39]. In numerous comparisons of amlodipine with other dihydropyridine calcium antagonists, it had a comparable in magnitude, but significantly longer antihypertensive effect [5, 10, 40]. At the same time, the advantageous advantage of the drug over other dihydropyridine calcium antagonists is the lack of its effect on heart rate, which allows it to be prescribed to patients with tachysystole. Only the latest generation calcium antagonists, lacidipine and mibefradil, have a similar effect on blood pressure as amlodipine.
The Amlodipine Cardiovascular Community Trial (ACT) [41] examined the comparative effectiveness of amlodipine in patients of different ages, gender and race. It has been established that the drug is equally effective in hypertensive patients of black and white races and is more effective among the female population. The ease of use of the drug also consists in long-term 24-hour control of blood pressure levels and a small number of adverse reactions.
Angina pectoris
Amlodipine has a pronounced coronary effect due to its high selectivity for smooth muscle cells of arterioles. The steal syndrome that occurs when using calcium antagonists is much less pronounced in long-acting drugs, including amlodipine. Amlodipine has the most beneficial effect when used in patients with a pronounced dynamic component of coronary obstruction. In a study by Chahine RA et al. [17] patients with proven vasospastic angina showed a significant reduction in episodes of angina and the frequency of additional use of nitroglycerin.
Table 4. Comparative antihypertensive effect of amlodipine with drugs from other groups
Authors
| Comparators | Duration of treatment | Number of patients | Results, ↓BP, mm Hg. Art. | |
| Frishman WH et al., 1994 [29] | Amlodipine 2.5-10 mg Atenolol 50-100 mg | 8 weeks | 125 | Aml ↓s/dBP lying at 12.8/10.1, standing at 11.5/9.8 mm Hg. Art. Athen ↓s/dBP lying at 11.3/11.7 standing at 12.3/12.3 mm Hg. Art. |
| Ding YA et al., 1995 [30] | Amlodipine 5-10 mg Quinapril 10-40 mg | 28 weeks | Both do not affect heart rate Aml ↓BP from 145/94 to 130/85 Quinn ↓BP from 144/94 to 134/88 | |
| Errico M. et al., 1997 [31] | Amlodipine 5-10 mg Captopril 50-100 mg + Hypothiazide 25-50 mg | 12 weeks | AML ↓BP within 24 hours, as opposed to a combination of drugs | |
| Viscoper RJ et al., 1997 [32] | Amlodipine 5-10 mg Mibefradil 50-100 mg | 12 weeks | 239 | Aml ↓dBP by 13.2 in 19.5%, does not affect heart rate Mib ↓dBP by 11.5 in 23.3%, vHR by 5.5 beats/min |
| Lorimer AR et al., 1998 [33] | Amlodipine up to 10 mg Lisinopril up to 20 mg | 12 weeks | 60 | Aml ↓BP lying down at 20 (syst.) and 14 (diast.), effect 24 hours Lys ↓BP lying down at 11 (syst.) and 7 (diast.), effect more during the day |
| Lefebre J. et al., 1998 [34] | Amlodipine 5-10 mg Nifedipine GITS 30-60 mg Felodipine ER 5-10 mg | 8 weeks | 89 | By ↓AD: Aml=Fel>Nif T/R for syst. and diast. Blood pressure: for Fel 5 mg - 0.07 and 0.1, Fel 10 mg - 0.23 and 0.31, Aml 5 mg - 0.22 and 0.31, Aml 10 mg - 0.45 and 0.58 , Nif 30 mg - 0.27 and 0.31, Nif 60 mg - 0.24 and 0.40 |
| Watts RW et al., 1998 [35] | Amlodipine 5-10 mg Diltiazem 180-360 mg | 30 | ↓BP with 24-hour monitoring up to: Aml 137/84, Dilt 143/86 mm Hg. Art. | |
| Zannad F. et al., 1999 [36] | Amlodipine 5-10 mg Perindopril 4-8 mg | 60 days | 96 | T/R for DBP: Aml 0.8, Per 0.81 T/R for SBP: Aml 0.83, Per 0.68 Blood pressure 24 hours after discontinuation of the drug is lower for Amlodipine |
| Videbaek LM et al., 1997 [37] | Amlodipine 5 mg Felodipine ER 5 mg | 2 weeks | 28 | R/T for AML 1.58, for Fel 4.43 |
Note: sBP - systolic blood pressure, dBP - diastolic blood pressure, T/P - through-to-peak coefficient, P/T - peak-to-through coefficient.
However, amlodipine is also widely used for the treatment of stable angina pectoris, both as monotherapy and (more often) as part of combination therapy.
In a study by Van Der Vring JA et al. [42] studied the effectiveness of calcium antagonists when added to β-blocker therapy in the treatment of patients with angina pectoris. The assessment was made based on changes in the performance of the bicycle ergometer test. As a result, although calcium antagonists (including amlodipine at a dose of 5-10 mg) did not increase the duration of exercise, they significantly delayed the onset of ischemic depression of the ST segment, and mibefradil was more effective than amlodipine, and amlodipine - diltiazem. At the same time, the use of mibefradil was limited by a higher incidence of side effects such as dizziness.
The effectiveness of amlodipine monotherapy at a dose of 2.5-10 mg in comparison with the b-blocker nadolol was assessed in a study by Singh S. [43]. At the same time, amlodipine delayed the development of an attack of angina pectoris much longer in comparison with nadolol (+21 and +8%, respectively). When comparing amlodipine with dinitrates, it turned out [19] that amlodipine was significantly more effective in reducing the duration of ischemic episodes, increasing the time to the onset of ST segment depression and angina, and had fewer side effects compared to isosorbide dinitrate. Similarly, a comparison of isosorbide mononitrate with amlodipine in patients with angina pectoris showed a greater protective effect of amlodipine compared with mononitrates in relation to myocardial damage in response to stress ischemia. Such damage occurs in 82% of cases when using mononitrates and only in 48% of cases when using amlodipine [23].
The multicenter CAPE study, conducted in 10 European countries, included patients with at least four episodes of ischemia, as determined by 48-hour ECG monitoring, with a total ischemic duration of more than 20 minutes [49]. Amlodipine significantly reduced the incidence of ST segment depression and total ischemic time (as measured by ECG), as well as the incidence of painful ischemic episodes and the frequency of additional use of short-acting nitrates [50].
The effect of amlodipine therapy on the prognosis of patients with coronary artery disease was assessed in the PREVENT study. There was a decrease in the number of hospitalizations due to destabilization of angina pectoris and chronic heart failure (61 in the amlodipine group and 88 in the placebo group). Also, with the use of amlodipine, a decrease in the number of myocardial revascularization operations was observed (53 compared with 85 in the placebo group), regardless of the use of b-blockers, nitrates or lipid-lowering therapy. The frequency of anginal attacks decreased from 85 to 60.
A comparative assessment of the effect on cardiovascular mortality of the angiotensin receptor antagonist valsartan and the calcium antagonist amlodipine is carried out in the VALUE (Valsartan Antihypertensive Long-tern Use Evaluation) study, which is currently not completed. 14,400 patients with arterial hypertension and additional risk factors (hypercholesteremia >6.5 mmol/l, serum creatinine >1.2 mg/dl, ECG signs of left ventricular hypertrophy, type II diabetes mellitus, coronary artery disease or stroke in history) were randomized. The ALLHAT (Antihypertensive Lipid Lowering Heart Attack Trial) study [44] has also not yet been completed, one of the directions of which is a comparative assessment of the effect of amlodipine on the incidence of non-fatal myocardial infarction and coronary death. The study compares four classes of antihypertensive drugs: diuretic, calcium antagonist, α-blocker, and ACE inhibitor in reducing cardiovascular morbidity and mortality in hypertensive patients with hypercholesterolemia.
In a meta-analysis, Kloner RA et al. [51] assessed the safety of calcium channel antagonists. Comparative and non-comparative studies of amlodipine and nifedipine GITS were included. It was shown that in patients receiving amlodipine, overall cardiovascular mortality, the incidence of acute myocardial infarction and progression of coronary artery disease were significantly lower than similar indicators for other calcium antagonists.
Chronic heart failure
The randomized, double-blind, placebo-controlled PRAISE I (Prospective Randomized Amlodipine Survival Evaluation Study) study [45] assessed the effect of the new calcium antagonist amlodipine in patients with chronic heart failure. The study included 1153 patients with an ejection fraction of less than 30% and chronic heart failure of ischemic and non-ischemic origin. The result showed a reduction in the total number of cardiovascular complications by 9%, a reduction in the risk of sudden death by 16% in the amlodipine group compared to placebo. Moreover, the change concerned exclusively patients with non-ischemic heart failure, who experienced a 31% reduction in the total number of cardiovascular complications and a 46% reduction in the risk of sudden death when using amlodipine.
The PRAISE II trial is currently being conducted to evaluate the role of amlodipine in the treatment of chronic non-ischemic heart failure (dilated cardiomyopathy). A decrease in clinical symptoms and plasma norepinephrine levels has been shown with the use of amlodipine in patients with dilated cardiomyopathy. A number of authors associate this effect of amlodipine with inhibition of NO hyperproduction and a decrease in myocardial damage.
Directions for use and dosage
Amlodipine is taken once daily due to its long half-life and long-term adequate blood pressure control. For arterial hypertension and angina pectoris, the usual initial dose of the drug is 5 mg once a day. Most patients do not require a dose increase, but the maximum dose is 10 mg/day. You should not increase the dose of the drug during the first week of use if blood pressure levels are insufficiently controlled, since the maximum effect of the drug develops later.
Drug interactions
No adjustment of the drug dose is required with the simultaneous use of thiazide diuretics, β-blockers, and ACE inhibitors. A beneficial effect on blood pressure levels has been shown with simultaneous administration of amlodipine with α-blockers [46].
The study by Schwartz JB [47] assessed the effect of amlodipine on the pharmacological profile of digoxin in healthy volunteers. There is no change in the steady-state concentration of digoxin (steady-state), as well as blood pressure or heart rate when the drugs are used together.
Conclusion
Amlodipine, an antagonist of slow L-type calcium channels from the group of dihydropyridines, is effective in mono- and combination therapy of arterial hypertension, treatment of coronary heart disease with severe coronary spasm, and is also used in the treatment of chronic heart failure of non-ischemic origin. Amlodipine is a long-acting drug, which eliminates the sharp hemodynamic changes characteristic of the initial period of absorption of short-acting calcium antagonists. Another important distinguishing feature of amlodipine from other dihydropyridine calcium antagonists is the lack of effect on heart rate, which expands the possibilities of use of the drug. In numerous studies, amlodipine was well tolerated, and the percentage of adverse reactions when using it did not significantly exceed that in the control group.