The left atrial appendage is a muscular bursa connected by a lumen to the left atrium and is part of the normal anatomy of the heart. However, in most cases, it is the left atrial appendage that is the main source of blood clots and thrombotic complications in patients with atrial fibrillation.
Atrial fibrillation (AF) is a major risk factor for the formation of blood clots (thrombi), which can block blood flow to the brain and lead to cerebral infarction (stroke).
How the left atrial appendage is associated with stroke in patients with AF
With AF, disruptions occur in the conduction system of the heart and irregular electrical impulses occur in the upper parts of the heart (atria), which leads to their trembling and irregular contraction. Irregular heartbeats lead to decreased blood flow, rapid heart rate, difficulty breathing, and shortness of breath. These irregular heartbeats lead to an increased risk of developing blood clots. The left atrial appendage has a long, tubular shape and connects to the left atrium. During AF, blood can pool in the atrial appendage and lead to the formation of blood clots. When the heart rhythm returns to normal, these blood clots can fly out of the appendage into the left atrium and then travel through the blood throughout the body, causing blockage of arteries in the brain and leading to the development of a stroke.
Uniqueness of the operation
Surgically isolated left atrial appendage has an advantage over conservative treatment methods in patients with persistent or paroxysmal atrial fibrillation. After surgery, 70% of patients maintain sinus heart rhythm during a long observation period. Clinical signs of the disease are significantly reduced, and overall well-being improves.
This operation is unique and is performed in only a few institutions in Russia. In our center, this operation is performed by the head of the department of x-ray surgical methods of diagnosis and treatment - Sergey Vladimirovich Korolev.
Specialists of the cardiac surgery department of the Federal Scientific and Clinical Center of the Federal Medical and Biological Agency successfully use advanced methods of treating cardiac arrhythmias. Our clinic performs unique minimally invasive operations, as well as high-quality diagnostics of various forms of arrhythmia, coronary heart disease and other cardiovascular diseases.
Our center provides services for mammary coronary bypass surgery, thoracoscopic isolation of the ostia of the pulmonary veins, the posterior wall of the left atrium and suturing of the appendage. As a result of these procedures, hundreds of patients annually manage to prevent a number of serious complications: such as stroke, heart attack, heart failure.
You can obtain more detailed information about other methods of treating cardiovascular diseases at the Cardiology Center of the Federal Scientific and Clinical Center of the Federal Medical and Biological Agency of Russia.
How is left atrial appendage occlusion performed?
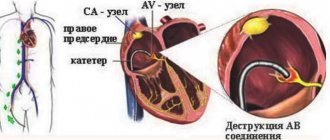
The procedure is performed using an endovascular, minimally invasive technique in a cath lab. By puncturing the femoral vein (usually on the right), the x-ray surgeon inserts a thin, flexible and long tube (catheter) into the right side of the heart. Next, puncture of the interatrial septum is performed and special instruments are carried out to the mouth of the left atrial appendage. During the entire procedure, X-ray images, as well as transesophageal echocardiography (TEE-CG) data, are used to monitor the implementation of instruments and their correct placement in the cavities of the heart.
Thoracoscopic isolation of the left atrium
This type of operation is performed in situations where traditional catheter ablation is impossible or ineffective. The impact on the heart is carried out through the inserted thoracoscope. Through 6-8 punctures in the chest area (symmetrically on the right and left), electrodes are inserted. High-frequency current destroys the source of arrhythmia. At the same time, in case of a blood clot, the left atrial appendage is sutured to prevent re-formation of clots, as well as reduce the risk of strokes and heart attacks.
The procedure is performed under anesthesia. Its distinctive features:
- high efficiency (75-96%);
- low morbidity;
- no need for artificial blood circulation and long-term hospitalization;
- short rehabilitation period, low risk of complications;
- rare relapses (less than with other methods).
A relative contraindication for treatment is severe heart disease (decompensated ischemic disease, valvular pathology), requiring more extensive surgical interventions.
Preparing for the study
Before the procedure, a consultation with a cardiologist and/or a neurologist is necessary, who will tell you in detail about all stages of the study, possible results and complications. A detailed allergy history is also collected to determine if there is an allergy to medications and/or contrast used during the procedure.
Your doctor will tell you which medications you are taking to stop taking on the day of your procedure. The patient should not independently decide to stop taking medications and can do this only after agreement with the cardiologist. It is advisable to avoid taking liquids and food several hours before the procedure.
What is the Amplatzer Cardiac Plug Occluder?
The Amplatzer Cardiac Plug is a device specifically designed for non-surgical, low-impact closure of the left atrial appendage.
The device is folded into a thin catheter (~4 mm in diameter) and delivered folded to the left atrial appendage. Next, the occluder is released from the catheter and takes on the shape as shown in the figure.
The occluder is securely fixed to the delivery cable and, if necessary, the x-ray surgeon can repeatedly remove the occluder again into the lumen of the catheter until he is sure that the occluder is securely fixed in the cavity of the ear. Only after this is the occluder disconnected from the delivery device.
Amplatzer Cardiac Plug is manufactured at the plant in Minnesota (USA) from a special alloy Nitinol (nickel-titanium alloy). Nitinol is absolutely not susceptible to corrosion, its strength exceeds both titanium and steel, and also has a special property of “shape memory”, when, when straightened, it acquires its original shape as shown in the figure.
Medical Internet conferences
Relevance
There is a huge number of works devoted to the morphological structure of the heart, but only a small part of them concerns the cardiac ears. The appendages are an additional cavity at the top of the atria. The cardiac ears have morphological features. For example, the inner surface of the left ear has a predominantly trabecular structure, while the relief of the right ear is formed mainly by bundles of pectineal muscles, and therefore its division into lobes is more pronounced. The right appendage extends from the right atrium, adjacent with its concave surface to the aortic bulb, and the left appendage of the heart extends from the anterior-superior wall of the left atrium, bends anteriorly, covering the initial part of the pulmonary trunk. In addition, in 80% of cases, the left ear is separated from the atrium cavity by a pronounced narrowing - a “neck”. The works of G.N. Borodina indicate that the ears differ in shape and size: the right ear is wider than the left, has a larger and simpler cavity, and the left ear is longer and narrower, delimited from the atrium by a well-defined interception [1]. At the moment, the exact function and biological role of the ears in the human body is not clear; there are only some assumptions about this.
Purpose: to determine the morphofunctional significance of the cardiac ears.
Tasks:
- Consider literary sources that contain information about the atrial appendages.
- Identify the functions of the cardiac ears indicated in modern scientific literature.
Materials and methods: a review of modern scientific medical literature and Internet resources devoted to the morphological structure of the heart was conducted.
results
The cardiac ears are an additional cavity in the atria, so they perform a reservoir function. For example, the systolic capacity of the left auricle is 40% of the entire atrium. A direct reference to the work of E. P. Panchenko and co-authors “Prevention of thromboembolism in patients with atrial fibrillation” shows that when the heart rhythm is disturbed, small blood clots - thrombi (especially in the left ear) can accumulate in the ears, which, under unfavorable conditions, are carried through the bloodstream , can thrombose blood vessels in various organs and cause a heart attack or stroke [2]. At the same time, NM Al-Saady in his study (1998) notes that the likelihood of thrombosis and stroke is higher with such morphological types of ears as cactus (cactus), windsock (windsock), cauliflower (cauliflower), and with this type of ears, like chicken wing, the likelihood of a blood clot is minimal. He also pointed out that the size of the ear can also serve as a kind of prognostic sign (predictor) of stroke [3]. JA Sallach also spoke about this in his monograph, additionally noting that the larger and deeper the ear, the greater the chance of thrombosis and stroke [4].
In addition, an interesting discovery was made by a team of scientists led by A. J. De Bold in 1981. During an experiment on laboratory rats, they discovered that in the right atrium and ears of the heart there are secretory cardiomyocytes that synthesize a peptide hormone - atrial natriuretic factor (ANF). When the atria are stretched, the secretion enters the blood and affects the kidneys, adrenal glands, the heart itself and even adipose tissue. PNF causes stimulation of diuresis and natriuresis, inhibition of the secretion of aldosterone and cortisol, vasodilation, and a decrease in blood pressure [5]. Also, A. J. De Bold found that increased production of this hormone is a harbinger of chronic heart failure [6].
E. A. Adyshirin-Zade and co-authors found that the ears are involved in the regulation of blood pressure in the corresponding parts of the heart due to the reservoir function of the cardiac ears and the action of natriuretic peptide, which dilates peripheral vessels and reduces the volume of circulating fluid (through diuresis) in arterial hypertension [ 7].
G. N. Borodina and co-authors in the book “The role of the ears of the heart in the diastolic blood filling of the atria” write that the ears play an integral role in ensuring the diastolic and systolic phases of heart contraction [8]. At the moment when the left ventricle contracts, the left atrium and its appendage are in diastole. Towards the end of ventricular systole, the left auricle begins to contract, but the atrium itself is still in the diastolic phase of the cardiac cycle. Due to the systole of the ear, the pressure in its cavity decreases to a negative (“suction” effect), due to which a “suction” effect also occurs in the atrium. Due to this, more blood enters the left atrium during diastole, which means that during atrial systole and ventricular diastole, more blood enters the left ventricle from the atrium.
It has long been believed that right atrial tachycardia is inappropriate sinus tachycardia because the right atrial appendage is a rare site of ectopic atrial tachycardia. However, MA Allessie, together with her colleagues, conducted a study in 2011, proving that ectopic atrial tachycardia from the right atrial appendage also exists as a disease [9]. On an ECG of an eight-year-old child with a rapid heartbeat, it was found that the P wave in the V1 and V2 branches with ectopic atrial tachycardia from the right atrial appendage is negative, and in sinus rhythm the P wave in V1 is usually biphasic and in V2 is almost always positive. It is this sign that is distinctive when making a diagnosis.
In addition, the auricles are involved in the nervous activity of the heart. Thus, R.B. Smith in 1971 indicated in his work that large accumulations of nerve cells were found on the inner walls of the cardiac ears [10]. Also, DH Pauza et al (1999) managed to localize large parasympathetic ganglia adjacent to the right vena pulmonalis superior and vena cava superior. Invading the underlying layers of the heart, they form a wide plexus, growing into the root and walls of the superior vena cava and spreading into the walls of the right atrium and its appendage. This large network innervates predominantly the sinoatrial node [11]. The role of the cardiac ears was also studied by D. Morman together with L. Heller. They found that in the left atrial appendage there are many dominant pathways, such as the intersection of the Bachmann bundle and the ligament of Marshall, and many sympathetic and vagus nerves that are involved in maintaining the normal physiological activity of the body [12].
DE Haines suggests that in the case of hypovolemia (decrease in circulating blood volume), specific receptors of the left auricle of the heart play an important role in regulating thirst, but there is no confirmed evidence on this yet [13].
According to the results of studies conducted in 2010, CP Chan, WS Wong, S. Pumprueg found that the atrial appendages are also used as optimal access to the cavity of the corresponding atrium during valve surgery, but at the same time, the position of the left appendage can partially close the entrance to left coronary artery, which is why the left appendage is sometimes removed [14]. The left ear may also be removed or its entrance closed for people at high risk of blood clots. VY Reddy, S. Mobius-Winkler, MA Miller write in their work that in modern times, closure of the left ear is carried out using special, recently created devices Watchman Device and Amplatzer Cardiac Plug, which are implants that isolate the left ear from the cavity left atrium [15].
Conclusion
Based on the above, we can conclude that the atrial appendages are an important and integral part of the heart and perform a number of important functions, namely: they perform an auxiliary hydrodynamic function in relation to the atria, endocrine function, the function of nervous regulation of blood pressure, and the feeling of thirst. But at the same time, the left atrial appendage is the main source of blood clots and thrombotic complications in patients with atrial fibrillation.
What happens after the occluder installation procedure
Because the occluder procedure is minimally invasive, recovery is likely to be quick and easy. Many patients are discharged from the hospital within the next 48 hours, with subsequent medication recommendations to continue treatment and recovery in an outpatient setting. It is necessary to conduct a control TEE-CG 3 and 6 months after installation of the occluder to monitor the process of endothelialization of the installed device. Endothelialization is the growth of the occluder with connective tissue and, in fact, its ingrowth into the wall of the heart. This is a normal and desirable process. In 99% of cases, complete endothelialization of the occluder occurs within several months. The patient returns to his normal lifestyle within the first month.
Is it possible to travel with an implanted device? Will there be problems going through the metal detector at airport security?
The metal parts of the Amplatzer Cardiac Plug are very small and will not normally trigger an alarm in an airport metal detector frame. However, for your comfort and peace of mind, you will be given a special card confirming the fact that the occluder has been installed.
Will an MRI interfere with or disrupt the occluder?
Most modern devices do not in any way affect the operation of the occluder, and the presence of an occluder does not affect the operation of the devices. However, it is best to alert staff to the presence of implanted devices before undergoing any medical procedure. Magnetic resonance imaging (MRI) is acceptable and the Amplatzer Cardiac Plug will not affect the performance of an MRI in any way, even at 3 Tesla. It is necessary to inform the staff of the MRI department about the presence of an implant.
Is the procedure possible for pregnant women and nursing mothers?
The risk of exposure of a child to X-ray radiation and the benefits of treatment must be weighed, and the correct and most effective tactics must be adopted. If it is necessary to implant a device during pregnancy, all possible measures will be taken to minimize radiation exposure to the fetus and mother.
There is no evidence of the effect of installing an occluder on the lactation process in nursing mothers.
Material and methods
The study is based on the treatment of 94 patients with non-paroxysmal forms of atrial fibrillation without other cardiac pathology.
What these patients had in common was that they were scheduled to undergo thoracoscopic radiofrequency fragmentation of the left atrium to treat atrial fibrillation.
Initially, all patients were under the supervision of arrhythmologists. Experts stated the ineffectiveness of further antiarrhythmic therapy and the futility of endovascular surgical treatment.
Nine patients (9.6%) were denied thoracoscopic radiofrequency ablation of the left atrium after further evaluation.
Refusal was due to a body mass index ≥35 kg/m2 (4 patients), chronic alcoholism (1 patient), manifestation of atrial fibrillation during antitumor chemotherapy with cardiotoxic drugs (2 patients), hypertrophic cardiomyopathy (1 patient), encephalopathy and non-compliance with the prescribed treatment ( 1 patient). The common characteristics of these 9 patients were symptoms not exceeding EHRA functional class II and the absence of clinical manifestations of chronic heart failure.
During the examination, a high risk of thromboembolic complications was confirmed in all nine patients:
— median risk of thromboembolic complications CHA2DS2-VASc 4 points (2; 6);
— a history of thrombosis of the left atrial appendage diagnosed by visualization methods (6 people);
— history of thromboembolic events that developed while taking anticoagulant drugs (2 people);
— contraindications to taking anticoagulant drugs (1 person).
Thus, given the impossibility or futility of restoring sinus rhythm, these patients were offered isolated thoracoscopic resection of the left atrial appendage in order to reduce the risk of thromboembolic complications.
Seven patients agreed to this operation, two patients refused.
Seven consenting patients underwent surgery between January 2021 and January 2021.
The sample included 3 men and 4 women, the average age was 67 years (from 45 to 71), the median risk of bleeding according to HAS-BLED was 3 (min 1, max 4).
Surgical technique
The surgery was performed under general anesthesia. A prerequisite was the possibility of right-sided one-lung ventilation.
The patient was placed on the operating table on his back. The arms are extended along the body. For ease of manipulation, thoracoscopic instruments provided free access to the patient's left hemithorax. For this purpose, the patient's left arm was positioned and fixed in such a way that the forearm was below the level of the operating table.
The operation began with “exhalation” of the left lung. Three thoracoports were installed in the left pleural cavity:
— IV intercostal space along the mid-axillary line — thoracoport with a diameter of 10 mm for optics;
— III intercostal space along the anterior axillary line — thoracoport with a diameter of 5 mm for the instrument;
- V or VI intercostal space along the anterior axillary line - a thoracoport with a diameter of 5 mm for an instrument or equipped with an adapter for a 5 mm thoracoport with a diameter of 15 mm for a stapler.
After installing the thoracoport for optics into the pleural cavity, carbon dioxide insufflation began at a flow rate of 8–10 l/min until an intrapleural pressure of 8–13 mmHg was achieved.
Using a coagulator (or other instrument), the pericardial cavity was opened along a line parallel to the phrenic nerve, 1.5-2 cm posterior to it. The pericardium was opened immediately in front of the pulmonary veins (Fig. 1) .
Rice. 1. Pericardotomy. Access to the left atrial appendage. 1 - pulmonary artery;
2 - left atrial appendage; 3 - phrenic nerve; 4 - root of the lung; 5 - blunt edge of the heart. After revision of the left atrial appendage, a stapler, for example, Covidien ENDO GIA™ (Medtronic), was inserted into the left pleural cavity. The stapler was inserted through a 15 mm thoracoport pre-installed into the counteraperture in the V-VI intercostal space or directly without the use of thoracoports.
For resection of the left atrial appendage in all patients, cassettes 60 mm long with staples 4.2 mm high were used (green cassette).
After revision of the left atrial appendage resection line, drainage of the left pleural cavity was performed through a counter-aperture for the stapler, followed by removal of the thoracoports and suturing of postoperative wounds.
Possible complications associated with the Amplatzer Cardiac Plug installation procedure
There are some potential risks associated with the placement of an occluder, as well as additional risks associated with the vein puncture procedure itself. It is necessary to consult with a radiologist about the possible risks of implanting the device.
Potential risks include, but are not limited to the following:
- air embolism (an air bubble that can move through the vessels and block the work of some of them);
- allergic reactions to contrast;
- allergic reaction to anesthetic drugs;
- cardiac arrhythmias (the occurrence of irregular heart rhythms);
- bleeding;
- heart failure;
- cardiac tamponade (rupture of the heart muscle);
- death;
- fever;
- hypertensive or hypotensive reactions of the body;
- infections;
- multiple organ failure;
- myocardial infarction (heart attack);
- perforation of the heart cavity or vessel;
- pericarditis (excess fluid in the pericardial sac);
- renal failure/renal dysfunction;
- cerebrovascular accidents (temporary or permanent);
- arterial thrombosis;
- valvular regurgitation or insufficiency.