Active ingredients in Mexidol
The main active ingredient of the drug is ethylhydropyridine succinate.
In addition to this component, there are additional elements:
- sodium metabisilfit;
- lactose monohydrate;
- Carmellose;
- talc;
- titanium oxide.
The drug is available in the form of tablets of 10 pieces per package and in ampoules of 2 and 5 ml. The solution contains purified water. The amount of active substance per tablet is 125 mg, solution concentration is 5%.
The drug belongs to the category of nootropic drugs, the action of which is aimed at normalizing metabolism in cells.
Taking the drug can protect the body from the toxic effects of harmful substances, so it is often prescribed for the treatment of alcohol and drug addiction.
Indications for the use of Mexidol
Instructions for use classify Mexidol as a universal drug. This drug is currently used in neurology, surgery and psychiatry. It can quickly eliminate headaches and dizziness, improve well-being and stabilize high blood pressure. The drug is capable of providing a rapid therapeutic effect in the event of seizures provoked by external factors in the form of medication.
The manufacturer offers a choice of solution or tablets for treatment.
This function allows you to use the following options for entering the active substance into the body:
- orally;
- intramuscularly;
- intravenously.
The drug allows you to treat the following diseases:
- disruption of the normal circulatory process;
- vegetative dystonia;
- myocardial infarction;
- purulent inflammatory processes occurring in the abdominal cavity;
- atherosclerosis;
- alcohol abuse withdrawal syndrome;
- peritonitis;
- pancreatitis in acute forms;
- overdose of neutroleptics.
The above list is not complete, since Mexidol is now actively used in the treatment of a fairly wide range of diseases. The drug is used as an addition to the complex treatment of diseases resulting from insufficient blood supply and nutrition to the tissues of internal organs.
The active substance has a beneficial effect on brain function, improving memory and the ability to concentrate. The drug is prescribed for ischemia and frequent surges in blood pressure. In the prevention and treatment of arterial hypertension, the drug is used only as a complex remedy in addition to conservative treatment.
The effect of Mexidol on blood pressure
The drug is often prescribed to normalize blood pressure. It is often used for hypotension and hypertension.
The positive effect on low and high blood pressure is due to the following effects:
- changes the composition of the blood and improves its blood flow, which helps accelerate blood circulation;
- has a strong antioxidant and anxiolytic effect;
- reduces the level of intoxication;
- cell membranes have a positive effect, functional performance is restored;
- Oxidative processes slow down;
- Reduces the content of “bad” cholesterol;
- Helps with neuroses.
Taking the drug improves the activity of neurotransmitters, which are responsible in the body for the quality of transmission of nerve impulses to brain cells. As a result of taking the drug, a person with hypertension experiences a general improvement in well-being, which is ensured by the resumption of metabolic processes and improved nutrition of internal organs. Stress is a common cause of high blood pressure. The effect of the drug reduces anxiety and relieves emotional discomfort, thereby normalizing blood pressure.
The ability to improve sleep quality and reduce psychomotor agitation also has a beneficial effect on blood pressure.
The properties of Mexidol make it possible to influence the mechanisms of formation of various types of diseases, leading to their inhibition and initiating the resumption of the body's defense reactions at the biochemical level. At the same time, the drug has a minimal number of side effects compared to drug analogues.
Mexidol tachycardia
Mexidol - 2-ethyl-6-methyl-3-hydroxypyridine succinate was synthesized at the Institute of Biochemical Physics of the Russian Academy of Sciences; studied and developed at the Research Institute of Pharmacology of the Russian Academy of Medical Sciences and the All-Russian Scientific Center for the safety of biologically active substances.
Mexidol is approved for wide medical use and is indicated for the treatment of acute cerebrovascular accidents, dyscirculatory encephalopathy, vegetative-vascular dystonia, atherosclerotic disorders of brain function, neurotic and neurosis-like disorders with anxiety, for the relief of withdrawal syndrome in alcoholism, for the treatment of acute intoxication with neuroleptics and a number of other diseases . Mexidol is a new type of drug, both in mechanism and in the spectrum of pharmacological action and has significant advantages over known neuropsychotropic drugs.
MECHANISM OF ACTION
Mexidol has an original mechanism of action, the fundamental difference of which from the mechanism of action of traditional neuropsychotropic drugs is its lack of specific binding to known receptors. Mexidol is an inhibitor of free radical processes, lipid peroxidation, it activates superoxide dismutase, affects the physicochemical properties of the membrane, increases the content of polar lipid fractions (phosphotidylserine and phosphotidylinositol, etc.) in the membrane, reduces the cholesterol/phospholipid ratio, reduces the viscosity of lipid layer and increases the fluidity of the membrane, activates the energy-synthesizing functions of mitochondria and improves energy metabolism in the cell and, thus, protects the cell apparatus and the structure of their membranes.
The change in the functional activity of the biological membrane caused by Mexidol leads to conformational changes in the protein macromolecules of synaptic membranes, as a result of which Mexidol has a modulating effect on the activity of membrane-bound enzymes, ion channels and receptor complexes, in particular, benzodiazepine, GABA, acetylcholine, enhancing their ability to bind to ligands, increasing the activity of neurotransmitters and the activation of synaptic processes.
Along with this, Mexidol has a pronounced lipid-lowering effect, reduces the level of total cholesterol and low-density lipoproteins and increases high-density lipoproteins.
Thus, the mechanism of action of Mexidol is determined primarily by its antioxidant properties, the ability to stabilize cell biomembranes, activate the energy-synthesizing functions of mitochondria, modulate the functioning of receptor complexes and the passage of ionic currents, enhance the binding of endogenous substances, improve synaptic transmission and the interconnection of brain structures. Thanks to this mechanism of action, Mexidol influences the key basic links in the pathogenesis of various diseases, has a wide range of effects, extremely few side effects and low toxicity, and has the ability to potentiate the action of other centrally active substances, especially those that act as direct receptor agonists.
PHARMACODYNAMICS
Mexidol, unlike well-known drugs, has a wide range of pharmacological effects, realized at least at two levels - neuronal and vascular.
It has cerebroprotective, anti-alcohol, nootropic, antihypoxic, tranquilizing, anticonvulsant, antiparkinsonian, anti-stress, vegetotropic effects. In addition, it has the ability to improve cerebral circulation, inhibit platelet aggregation, reduce total cholesterol levels, and have an anti-atherosclerotic effect. The therapeutic effects of Mexidol are detected in the dose range from 10 to 300 mg/kg.
Mexidol increases the body's resistance to various extreme damaging factors, such as sleep disturbance, conflict situations, stress, brain injury, electric shock, physical activity, hypoxia, ischemia, and various intoxications, including ethanol.
Mexidol has a pronounced tranquilizing and anti-stress effect, the ability to eliminate anxiety, fear, tension, restlessness, in particular in conflict situations. When administered parenterally, it has a similar depth of effect to diazepam (Seduxen) and alprazolam (Xanax). Anti-stress effect
Mexidol is expressed in the normalization of post-aggressive behavior, somatovegetative indicators, restoration of sleep-wake cycles and impaired learning and memory processes, reduction of stomach ulcers, reduction of dystrophic, morphological changes that occur after stress in various structures of the brain and in the myocardium.
Mexidol has a distinct anticonvulsant effect, influencing both primary generalized seizures, caused primarily by the administration of GABAergic substances, and the epileptiform activity of the brain with a chronic epileptogenic focus.
The nootropic properties of Mexidol are expressed in the ability to improve learning and memory, promote the preservation of a memorable trace and counteract the process of extinction of acquired skills and reflexes. Mexidol has a pronounced anti-amnestic effect, eliminating memory impairment caused by various influences (electric shock, brain injury, sleep deprivation, administration of scopolamine, ethanol, benzodiazepines, etc.).
Mexidol has a clear antihypoxic and antiischemic effect, which is expressed in the ability of the drug to increase life expectancy and the number of surviving animals under various hypoxic conditions: hypobaric hypoxia, hypoxia with hypercapnia in a hermetic volume and hemic hypoxia. In terms of antihypoxic activity, Mexidol is significantly superior to pyritinol and piracetam, which at doses of 300 and even 500 mg/kg have weak antihypoxic activity under conditions of acute hypobaric hypoxia and hypoxia with hypercapnia. In addition, Mexidol has a pronounced antihypoxic effect on the myocardium in experiments on an isolated, perforated, contracting heart. According to the mechanism for the implementation of these effects, Mexidol is an antihypoxant with a direct energizing effect, the effect of which is associated with the influence on the endogenous respiration of mitochondria, with the activation of the energy-synthesizing function of mitochondria. The antihypoxic effect of Mexidol is due not only to its own antioxidant properties, but also to its constituent succinate, which, under hypoxic conditions, entering the intracellular space, can be oxidized by the respiratory chain.
Mexidol has a pronounced anti-alcohol effect. It eliminates the neurological and neurotoxic manifestations of acute alcohol intoxication caused by a single injection of high doses of ethanol, and also restores behavioral disorders of the vegetative and emotional status, deterioration of cognitive functions, learning and memory processes caused by long-term (5 months) administration of ethanol and its withdrawal, and prevents accumulation of lipofuscin in the brain of alcoholized animals.
Mexidol has a pronounced geroprotective effect, has a clear corrective effect on learning and memory processes impaired during aging, improving the process of fixation, storage and reproduction of information, helps restore emotional and vegetative status, reduces manifestations of neurological deficits, reduces the level of aging markers - lipofuscin - in the brain and blood , malonaldehyde, cholesterol. The mechanism of the geroprotective action of Mexidol is associated with its antioxidant properties, the ability to inhibit lipid peroxidation processes, its direct membranotropic effect, the ability to restore ultrastructural changes in the granular endoplasmic reticulum and mitochondria, and modulate the functioning of receptor complexes. Mexidol has an antiatherogenic effect. The drug inhibits the humoral manifestations of atheroarteriosclerosis: reduces hyperlipidemia, prevents the activation of lipid peroxidation, increases the activity of the antioxidant system, prevents the development of pathological changes in the vascular wall and reduces the degree of damage to the aorta.
Mexidol reduces the content of atherogenic lipoproteins and triglycerides, increases the level of high-density lipoproteins in the blood serum, and prevents deficiency of highly unsaturated phospholipids.
Mexidol not only causes regression of atherosclerotic changes in the main arteries and restores lipid homeostasis, but also corrects disturbances in the regulatory and microcirculatory systems, which is expressed in the fact that there is no structure of arterioles and precapillaries, and their diameter differs little from the control, only focal ones are determined in venules aggregates, and complete elimination of spasm of afferent microvessels is observed.
In addition, 2-ethyl-6-methyl-3-hydroxypyridine derivatives, which include Mexidol, suppress platelet aggregation caused by collagen, thrombin, ADP and arachidonic acid, inhibit platelet cyclic nucleotide phosphodiesterase, and also protect blood cells during mechanical injury . In particular, stabilizing resistance of erythrocyte membranes to hemolysis is observed and the process of hematopoiesis (restoration of the number of erythrocytes) after acute blood loss or chemical hemolysis is accelerated.
The hepatoprotective effect of Mexidol was established in three models of acute toxic liver damage, in which hepatocyte cytolysis syndrome was caused by various hepatotoxins.
In conditions of liver damage caused by carbon tetrachloride, Mexidol reduces areas of liver tissue necrosis and the volume of fatty degeneration of hepatocytes, normalizes the energy balance of hepatocytes, and has a protective effect on the nuclear and cytoplasmic pool of nucleic acids. In case of alcoholic liver damage, the effect of Mexidol is expressed in a decrease in the number of hepatocytes with lysis of nuclei and chromatin, acceleration of restoration of the total genome of hepatocytes and an increase in the content of nucleic acids in the liver tissue and nuclei of hepatocytes. 3-hydroxypyridine derivatives have a protective effect against the toxic effect on the liver of the strong hepatotropic carcinogen diethylnitrosoamine (DENA), since they form complexes with cytochrome P-450 and thereby prevent its complex formation with DENA.
Mexidol has a pronounced ability to have a potentiating effect on the effects of other neuropsychotropic drugs. Under the influence of Mexidol, the effect of tranquilizing, neuroleptic, antidepressant, hypnotics and anticonvulsants is enhanced, which makes it possible to reduce their doses and reduce side effects. In particular, when Mexidol is combined with carbamazepine, the dose of the anticonvulsant can be reduced by 2 times without reducing its therapeutic effect. The combined use of Mexidol with carbamazepine allows for adequate pathogenetic therapy of partial epilepsy, reduces the side effects of carbamazepine with long-term use without reducing its therapeutic effectiveness, and thereby optimizes the treatment of patients with epilepsy.
Side effects and toxicity
A significant advantage of Mexidol is that it has minor side effects and low toxicity. When studying the side effects of Mexidol, it was found that even in the upper range of therapeutic doses it has neither a depressing nor a stimulating effect on spontaneous motor activity, does not change the coordination of movements, the exploratory behavior of animals, rectal temperature, corneal and pineal reflexes, and does not cause drowsiness . The drug maintains the adequacy of the animals' response to the stimuli provoking the test, and simple reflexes are not impaired. With an increase in the average therapeutic dose by 4-5.5 times, Mexidol does not have a muscle relaxant effect. Along with this, Mexidol, even in extremely high doses, does not impair memory and does not cause amnesia, but, on the contrary, has an anti-amnestic effect in case of memory impairment.
Mexidol does not have a negative effect on the liver, but on the contrary, has a hepatoprotective effect. The drug does not change the heart rate, does not change blood pressure, ECG, hemodynamics and breathing rhythm, does not cause changes in the composition of the blood, skin color and mucous membranes, urination, bowel movements and salivation.
Side effects
Mexidol is expressed mainly in inhibition of motor activity and impaired coordination of movements and begins to appear in individual animals when doses are increased to 300 mg/kg and higher when administered intraperitoneally and in doses of 400 mg/kg and higher when Mexidol is administered orally.
Long-term administration
Mexidol (2-3 months) does not cause a decrease in its therapeutic effect or the appearance of additional undesirable manifestations. After stopping long-term administration of Mexidol, no withdrawal syndrome is observed.
Acute toxicity
Mexidol was determined by recording the death of animals 24 hours after administration of the drug.
The lethal dose of Mexidol, causing the death of 50% of animals (LD50) is 820 (625 - 1025) mg/kg for rats and 475 (365 -617) mg/kg for mice, and when administered orally - more than 3000 mg/kg in rats and 2010 (1608 - 2513) mg/kg in mice. A study of the chronic toxicity
of Mexidol with long-term oral and parenteral use in experimental animals did not reveal significant changes in the organs and tissues of the body.
A comparison of effective therapeutic doses of Mexidol with doses that cause side effects (sedation, incoordination, LD50) or toxic, lethal doses (LD50) shows the significant therapeutic breadth of Mexidol. The therapeutic index calculated from the LD50/ED50 ratio is 6.2, and from the LD50/ED50 ratio is 16.4, which indicates the harmlessness and safety of the drug.
PHARMACOKINETICS AND METABOLISM
Mexidol has high bioavailability. When administered parenterally to rats, it is rapidly absorbed from the abdominal cavity with a half-absorption period of 0.94 hours and maximum concentrations in plasma are reached after 3 hours, and in the brain and liver of animals - after 2-3 hours. A study of the binding ability of the membranes of the endoplasmic reticulum of the liver and brain of rats with Mexidol showed that the substance is determined in significant quantities in the membranes for 72 hours, which indicates the membranotropic properties of Mexidol. After intravenous administration of Mexidol to rabbits, the substance is eliminated from the blood plasma bioexponentially and can be determined according to theoretical calculations in fairly high concentrations for 6-12 hours. The high lipophilicity of Mexidol, its ability to bind to blood plasma proteins and endoplasmic reticulum membranes suggest the formation of tissue and blood depots of Mexidol in the body of animals.
An analysis of the pharmacokinetic parameters of Mexidol in patients in the clinic showed that, both with single and course use, the concentration of Mexidol in the blood increases quite quickly, reaching a maximum after an average of 0.58 hours. At the same time, Mexidol is quickly eliminated from the blood and after 4 hours it is practically not registered. The pharmacokinetic profiles of the drug did not differ significantly between single and chronic administration. A study of the excretion of Mexidol in the urine showed that it is excreted both unchanged and in the form of a glucuronoconjugate, which constitutes a significant amount. When studying the metabolism of Mexidol in rats, 5 metabolites were identified.
Metabolite I is phosphate (at the hydroxy group) of 3-hydroxypyridine, the formation of which occurs in the liver. In the blood, under the influence of alkaline phosphatase, 3-hydroxypyridine phosphate is split into phosphoric acid and 3-hydroxypyridine.
Metabolite II - 2-methyl-6-methyl-3-hydroxypyridine - is formed in large quantities and is found in the urine on the first and second days after Mexidol administration; this metabolite has a spectrum of pharmacological activity close to Mexidol.
Metabolite III - 6-methyl-3-hydroxypyridine is contained and excreted in large quantities in the urine.
Metabolite IV is a glucuronic conjugate with 2-ethyl-6-methyl-3-hydroxypyridine.
Metabolite V is a glucuronic conjugate with 2-ethyl-6-methyl-3-hydroxypyridine phosphate.
APPLICATION OF MEXIDOL IN NEUROLOGY AND PSYCHIATRY
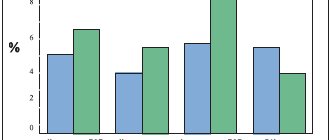
Mexidol is an effective means of anti-ischemic protection of the brain in cerebral strokes. The drug has a pronounced therapeutic effect in patients with acute cerebrovascular accidents, including patients with ischemic and hemorrhagic stroke located in the circulation zone of the internal carotid artery and its branches, as well as in the vertebrobasilar system. Mexidol, as a rule, is administered to patients in the first hours of admission to the clinic intravenously in a stream or intravenously drip and intramuscularly, in doses of 50 mg. up to 400 mg. once, from 50 mg. up to 900 mg. per day with a frequency of administration of 3. The duration of action of the drug is about 4 hours. During the same time, the drug is detected in the blood of patients. One of the most significant manifestations of the effect of Mexidol when included in the complex therapy of cerebral stroke is a significant decrease in the daily mortality of patients in the acute period of stroke, as well as a tendency to an overall decrease in mortality in this disease. In the acute period of cerebral stroke, the mortality rate of patients was -31.5% for those taking Mexidol, and -52.5% without it; The bed days also decreased significantly: 38.2±2.7 with Mexidol and 45.2±4.0 days without Mexidol (B.A. Spasennikov). When using Mexidol in the treatment of cerebral stroke, first of all, a more rapid regression of neurological symptoms, assessed on the Matthew scale, is observed. Thus, in patients who were in serious condition at the time of admission to the clinic, the Matthew index at the end of the acute period (21 days) was 51.5 ± 2.1, and after treatment with Mexidol it significantly increased to 59.7 ± 1.0. When treating patients with Mexidol, the dynamics of improvement in motor functions, revealed when using the ADL index, was also indicative. So, after 21 days this indicator was 76.6±3.1 in patients using Mexidol, and in the group of patients without using Mexidol it was 63.2±4.6 (the difference is significant at P
Echopulsography of intracranial arteries and veins after intravenous administration of Mexidol showed that already 30 minutes after the injection and for 4-6 hours, there is an increase in the amplitude (on average by 25.5%) of pulse oscillations of the cerebral vessels and the outflow of blood into the cerebral veins is facilitated. Under the influence of Mexidol, an increase in linear and volumetric blood flow is observed in the extracranial sections of the main arteries of the head, which is recorded within 6 hours after administration of the drug.
Registration of rheoencephalography after a course of treatment with Mexidol revealed normalization of waveforms in 67% of patients, and improvement in venous outflow in 38%. There is an increase in pulse blood supply in the external carotid artery system and in the vertebrobasilar system, with its initially low level, and normalization of the tone of small arteries and veins in both vascular systems. Mexidol causes normalization of the EEG of patients with DE, which is expressed in an increase in the total power of the spectrum due to the alpha and beta ranges without a significant change in the slow wave part of the spectrum. In patients receiving Mexidol, the increased content of hemoglobin and leukocytes decreases, blood viscosity decreases, cholesterol levels decrease, and the lecithin-cholesterol ratio increases.
Thus, Mexidol has a pronounced therapeutic effect in patients with dyscirculatory encephalopathy of stages 1, 2 and 3. Under the influence of Mexidol, remission or regression of neurological syndromic deficit is observed. As a result of treatment with Mexidol, 64% of patients showed a marked improvement in their condition, 32% had a moderate improvement, 20% had a slight improvement, and 16% had no effect. A comparison of the clinical effectiveness of Mexidol and known drugs showed that the index of overall effectiveness in the treatment of DE was 2.05 for Mexidol. for Cavinton, Trental and Sermion -2.1, Arsdergin -1.8. Mexidol is effective in patients with vegetative-vascular dystopia with symptoms of autonomic crises of a sympatho-adrenal nature, in whom improvement occurred within 5-14 days after the start of treatment. The intensity and frequency of headaches decreased, vasoactive imbalance and excitability decreased, and sleep improved. In 13% of patients, vegetative crises completely stopped and did not reappear over the next 2-3 months. Mexidol has a positive effect in patients with mental pathology of late age, especially with atherosclerotic dementia, in whom Mexidol was administered intramuscularly (patients received 100 mg for the first 5 days, and 300 mg daily for the remaining days, course - 3 weeks). Mexidol had a positive effect on memory, especially on current events, improved concentration, learning instructions, caused a decrease in headaches and symptoms of anxiety and depression. The degree of dysarthria and tearfulness in patients decreased. In some patients, dizziness completely disappeared, a confident gait appeared, and asthenia decreased. In some patients with initial manifestations of the senile-atrophic process and in patients with atherosclerotic dementia, after treatment with Mexidol, there is an increase in activity and an improvement in mood in the head. Thus, the use of Mexidol improves intellectual-mnestic activity in patients with age-related organic weakening processes, mainly in patients with atherosclerotic dementia, helping to improve concentration, follow instructions, memory for the present, reduce headaches, dizziness, tearfulness, dysarthria, and increase activity .
Mexidol has a pronounced positive effect in the treatment of chronic neuroleptic syndrome with symptoms of tardive dyskinesia and subacute neuroleptic syndrome. Before treatment with Mexidol, all patients received active therapy for neuroleptic syndrome with the drugs cyclodol, norparkin, midantan, tiapride, cerucal, tremblex, detoxification therapy with intravenous administration of nootropil, vitamins B and C, which was assessed as ineffective.
Mexidol had a pronounced antiparkinsonian and vegetotropic effect in these patients who were difficult to treat. The effect of Mexidol began to manifest itself already from the 2-3rd day of therapy and consisted of a decrease in the severity of oral-lingual hyperkinesis, which completely disappeared by the 7-14th day of treatment, then, under the influence of the drug, a decrease in limb tremor, stiffness, hypokinesia and hypomimia was noted, it improved, became more confident, free gait of patients, which ceased to be shuffling and mincing. The phenomena of orthogatism and dizziness decreased and disappeared, there was a tendency to normalize blood pressure with drug-induced hypotension, and Mexidol had no effect on normal blood pressure, weakness, lethargy, and dizziness decreased. The antiparkinsonian effect of Mexidol persisted for another 3-5 days after its discontinuation. Mexidol also has the ability to overcome the body's resistance to the effects of psychotropic drugs. Mexidol for this pathology was used at a dose of 300-500 mg per day with a treatment duration of 2-4 weeks. The effect of Mexidol began to appear already on the 3rd day of administration. Patients noted an improvement in the appearance, color and turgor of the skin, appetite, a decrease in lethargy, weakness, dizziness, dry mouth, and they became less lethargic. Against the background of Mexidol, it was possible to increase the doses of antidepressants and antipsychotics by 1.5-2 times without the occurrence of side effects. In a number of cases, the administration of previously ineffective drugs against the background of Mexidol made it possible to overcome the body's resistance and caused a significant decrease in depressive disorders and improvement in condition. In neurotic and neurosis-like conditions, Mexidol has a distinct tranquilizing effect, combined with a vegeto-normalizing effect. The therapeutic effect of Mexidol was most fully manifested in patients with neuroses and organic damage to the central nervous system with asthenic and astheno-vegetative disorders. The drug was effective and well tolerated by elderly patients. In 6 patients with asthenic disorders, the reverse development of anxiety and emotional tension against the background of Mexidol was accompanied by a peculiar activation with an increase in the background mood, a reduction in asthenic symptoms themselves. The tranquilizing effect of Mexidol is comparable in power to the effect of uxepam. Mexidol has a positive effect on sleep, restoring its duration and depth. The effect of Mexidol appears after 3-7 days of therapy. According to its spectrum of action, Mexidol can be classified as a daytime tranquilizer, which is effective both in hospital and outpatient settings, as well as in the elderly.
Mexidol has shown high effectiveness in the treatment of alcohol withdrawal syndrome with somato-neurological and mental symptoms. The dose of Mexidol was 100-400 mg per day intramuscularly with a course duration of 5-7 days (against the background of conventional detoxification agents). Mexidol is an effective remedy for the rapid relief of alcohol withdrawal syndrome with a wide range of effects, both on its psychopathological components and on vegetative-vascular manifestations.
The effect of Mexidol is observed within 1-1.5 hours after administration of the drug, and a persistent improvement in the condition occurs after 2-3 days. Patients experience a feeling of enlightenment, clarity in the head, headaches disappear, the process of concentration and comprehension when reading literature improves, anxiety, unaccountable fear, internal tension decrease, relaxation and a comfortable state appear, nightmares disappear, hypnotic hallucinations disappear, dreams become alcohol-free topics, sleep disorders disappear. Patients note the appearance of vigor and activity. Along with this, under the influence of Mexidol, alcohol motivation was significantly suppressed. Side effects. Comparison with cerebroprotective and psychotropic drugs. Mexidol is well tolerated by patients and causes only isolated side effects, which quickly disappear on their own or when the drug is discontinued.
Of the hundreds of patients treated with Mexidol, side effects occurred in exceptional cases. Two patients with discirculatory encephalopathy experienced nausea and dizziness a few minutes after the intramuscular injection of Mexidol, which went away on their own. Two patients with alcoholism experienced bitterness and dry mouth, dizziness, and weakness, which quickly disappeared when the drug was discontinued. In three patients with resistant depression combined with manifestations of chronic neuroleptic syndrome, after the first two or three injections a slight drowsiness appeared, which then disappeared on its own. One patient with neurosis, at the beginning of therapy, had a pinpoint rash on the skin of the forearms, not accompanied by itching and peeling, which self-reduced within three days with continued therapy. The insignificance of side effects makes Mexidol stand out among the known neuroprotective, nootropic and tranquilizing agents. The arsenal of drugs used in modern medicine that improve cerebral circulation and are used in injection form is quite limited and includes pentoxifylline (Trental), vinpocetine (Cavinton), nicergoline (Sermion), dihydroergotoxin (Redergan). Cinnarizine (stugeron), flunarizine, nimodipine are used in the form of tablets and capsules. A significant drawback of these known drugs, which in many cases limits their use, is the significant number and frequency of side effects. Pentoxifylline (trental) causes headache, dizziness, tachycardia, facial flushing, palpitations, angina pectoris, arterial hypotension, nervousness, drowsiness or insomnia, bleeding from the vessels of the skin and mucous membranes, urticaria, skin rashes, itching, nausea, vomiting, a feeling of heaviness in the epigastrium, increased fragility of nails, changes in body weight, swelling, and in case of an overdose of the drug, convulsions, loss of consciousness, and fever may occur. In this regard, contraindications to the use of trental are acute myocardial infarction, massive bleeding, cerebral hemorrhage, retinal hemorrhage, severe atherosclerotic damage to the blood vessels of the brain and heart, severe heart rhythm disturbances, pregnancy, lactation. Characteristic side effects of vinpocetine (Cavinton) are a decrease in blood pressure and tachycardia, and contraindications to the use of the drug are coronary heart disease and severe forms of arrhythmias. Nicergoline (sermion) causes arterial hypotension, dizziness, a feeling of heat and flushing, drowsiness and sleep disturbance. Side effects of dihydroergotoxin (redergin) are nausea, vomiting, a feeling of heaviness in the stomach, loss of appetite, blurred vision, hyperemia of the nasal mucosa, skin rash, orthostatic hypotension, and contraindications to the use of the drug are severe coronary heart disease, severe bradycardia and arterial hypotension .
Thus, all drugs currently used to treat cerebrovascular accidents are associated with significant side effects. In conditions of oxygen and energy deficiency that occurs with cerebrovascular lesions of the brain, Mexidol, which has a normalizing effect on cerebral metabolism, on fine neurochemical regulation and has minimal side effects, is of particular value. Cerebroprotective therapy with Mexidol differs from traditional effects on homeostasis and hemodynamics in its safety of use, the possibility of long-term use, and the ability to influence various levels and types of neurological and mental disorders. In contrast to traditional drugs, Mexidol does not cause a decrease in blood pressure, hemodynamic or ECG disturbances, and does not affect the heart rate. The positive effects of Mexidol in comparison with well-known drugs are its therapeutic effect on vasomotor instability, reduction of autonomic dysfunction, reduction of tachycardia, hyperemia, sweating, etc. In addition, Mexidol has a restorative effect on the functions of the motor sphere, improving coordination of movements and reducing psychomotor agitation, improves sleep, eliminates nervousness. Thus, having a high therapeutic effect, Mexidol does not have the side effects characteristic of other neuroprotective drugs. In contrast to sodium hydroxybutyrate and seduxen, Mexidol does not change the rhythm and frequency of breathing, i.e. does not cause the cardiorespiratory depression inherent in these drugs.
In contrast to noopropic drugs, when using Mexidol, there is no activating effect, sleep disturbances or increased convulsive readiness. In addition, Mexidol is significantly more effective than piracetam (nootropil). In comparison with benzodiazepine tranquilizers (seduxen, elenium, oxazepam, lorazepam, phenazepam, etc.), Mexidol does not have a muscle relaxant effect even in doses exceeding the average therapeutic anxiolytic dose by 4-5.5 times and does not cause such manifestations as impaired coordination movements, decreased muscle tone and muscle strength. Mexidol, in contrast to anxiolytics, does not have a sedative or amnesic effect, but, on the contrary, has a positive effect on memory, especially in conditions of impaired cognitive functions. With long-term administration of Mexidol and cessation of its use, there are no signs of withdrawal syndrome characteristic of benzodiazepine tranquilizers. Thus, Mexidol is a selective tranquilizer of “daytime” action, in which the anxiolytic and anti-stress effects are carried out without the layering of sedative, muscle relaxant and amnesic effects.
Possessing a high therapeutic effect, Mexidol does not cause side effects characteristic of known neuroprotective, nootropic and tranquilizing drugs, which indicates its safety and significantly expands the possibilities of use.
Directions for use and doses
Mexidol is prescribed intravenously (stream or drip), intramuscularly and orally. When administered intravenously, the drug should be diluted with water for injection or in physiological sodium chloride solution. For infusion administration, physiological NaCl solution should be used. Mexidol is administered in a stream over 1.5-3.0 minutes, and dropwise at a rate of 80-120 drops per minute. The duration of treatment and the daily dose of the drug depend on the nosology of the disease and the severity of the patient’s condition. For the treatment of acute cerebrovascular accident, Mexidol is prescribed intravenously by drip of 400 mg (8 ml) in isotonic sodium chloride solution (100-150 ml) twice a day for the first 15 days in intensive care or a specialized neurological department (maximum daily dose 1600 mg) . Then 400 mg (8 ml) 1 time per day intravenously in physiological NaCl solution daily for 15 days.
In the future, it is recommended to administer Mexidol intramuscularly at a dose of 200 mg (4 ml) once a day for 10-15 days. In subsequent complex drug therapy, it is advisable to include a tablet form of the drug, 0.25-0.5 g/day for 4-6 weeks. The daily dose is distributed into 2-3 doses during the day.
For the treatment of dyscirculatory encephalopathy (both against the background of cerebral atherosclerosis and against the background of hypertension):
Mexidol increases or decreases blood pressure
Mexidol indirectly affects blood pressure. The result of using the drug depends on the characteristics of the disease and the patient’s body. Mexidol belongs to a group of drugs that have a complex effect on the body, improving the functioning of all internal organs. It is thanks to this action that normalization of pressure occurs.
The drug is effective with minor deviations from the norm, and the effect can be both downward and upward.
Therefore, treatment with Mexidol begins with small doses, adjusting the amount of the drug depending on the effect obtained.
With an increased level of pressure, negative processes occur in the patient’s body, resulting in significant oxygen starvation. The hypoxic state causes a sharp deterioration in health and malaise. With high blood pressure, Mexidol improves blood flow, which helps stabilize the situation.
In case of arterial hypotension, Mexidol should be taken with caution, as the drug can lower blood pressure. For problems with blood pressure, drug therapy can provide significant improvement, but the length and duration of medication should be determined by the attending physician. It is worth remembering that the drug for low or high blood pressure should complement traditional treatment, and not be a complete replacement for antihypertensive drugs.
History of creation
Mexidol is an original domestic drug that has proven its effectiveness and safety in numerous clinical studies and successful twenty-year use in real clinical practice [1, 2].
Mexidol interrupts the ischemic cascade, affecting its most important stages: energy synthesis disorder, glutamate excitotoxicity and oxidative stress. Thanks to the universal mechanism of action, the drug can be used for all nosologies accompanied by ischemia and hypoxia, but primarily for ischemia of the most energy-consuming organs and systems of the body - nervous and cardiovascular [1]. Mexidol was synthesized in the early 1980s. at the State Institution "Research Institute of Pharmacology" RAMS L.D. Smirnov and V.I. Kuzmin. Under the leadership of Academician of the Russian Academy of Medical Sciences A.V. Waldman conducted its preclinical studies, established its pharmacological action and safety (B.I. Lyubimov) and studied the pharmacokinetics of the drug (A.K. Sariev, V.P. Zherdev) [1]. Having successfully completed clinical trials (G.G. Neznamov, E.S. Teleshova, S.A. Syunyakov, A.I. Fedin, Z.A. Suslina), on December 31, 1996 Mexidol was registered in the Russian Federation [3]. Thus, 2021 marks 20 years of successful use of Mexidol in clinical practice. For the study of the properties and introduction of Mexidol into clinical practice to a group of scientists (K.M. Dyumaev, E.B. Burlakova, L.D. Smirnov, T.A. Voronina, T.L. Garibova, V.P. Zhestkov, L. N. Sernov, N.V. Vereshchagin, Z.A. Suslina, N.V. Mironov, V.I. Shmyrev, A.I. Fedin, B.A. Knyazev, E.A. Avakyan, E.Yu. Lopatukhin) in 2003 was awarded the Russian Government Prize in the field of science and technology “For the creation and introduction into medical practice of antioxidant drugs for the treatment and prevention of cerebrovascular diseases” [4].
Modern ideas about pharmacokinetics
The pharmacokinetics of Mexidol have been studied in detail in experimental studies. It was shown in Chinchilla rabbits that when administered intragastrically at a dose of 100 mg/kg, Mexidol is rapidly absorbed from the gastrointestinal tract. The maximum concentration of the drug is achieved on average 30 minutes after oral administration, the half-life is 2.3 hours, and the average retention time is 3.2 hours. 5 hours after oral administration, Mexidol is not detected in the blood plasma of experimental animals [5]. Similar results were obtained when studying the pharmacokinetics of Mexidol in Wistar rats with intragastric administration at a dose of 200 mg/kg: the time to reach Cmax is on average 1 hour, and 5 hours after administration the drug concentration is below the detection limit [6].
When Mexidol is administered intramuscularly at a dose of 400–500 mg, its Cmax in human blood plasma is reached on average after 0.58 hours and amounts to 3.5–4.0 mcg/ml. The average retention time of the drug is 0.7–1.3 hours, and already 4 hours after intramuscular administration, Mexidol is practically not recorded in the blood plasma of volunteers. Taking into account the rapid elimination of the drug (when administered both in injection and tablet dosage forms) from the body of humans and animals, in order to achieve an optimal therapeutic effect, it is necessary to prescribe the drug at least 3 times a day. An alternative to this approach is the creation of new retarded dosage forms of Mexidol, which ensure a stable concentration of the drug in the blood plasma for 24 hours.
Mexidol is quickly distributed into organs and tissues, incl. and into the brain, penetrating the blood-brain barrier. With intragastric administration of Mexidol to Wistar rats at a dose of 200 mg/kg body weight, the peak of its concentration in the homogenate of the cerebral cortex and medulla oblongata of rats is observed 1.0–1.5 hours after oral administration of the drug, and then gradually decreases by the 4th hour. The highest level of Mexidol in the homogenate of the cerebellum and thalamus of rats is recorded 30 minutes after oral administration of the drug, and subsequently its content gradually decreases. Moreover, its maximum concentration is determined in the homogenate of the cerebral cortex [6].
When studying the correlation between the concentration of Mexidol in homogenates of different parts of the rat brain and its content in the blood plasma, a significant directly proportional relationship was revealed [6]. It has also been shown that Mexidol is not a substrate of the protein transporter glycoprotein-P, which regulates the penetration of a number of drugs through the blood-brain barrier [7]. Taken together, these facts suggest that penetration of the drug into the brain through the blood-brain barrier is most likely simple diffusion.
It has also been shown that Mexidol is able to penetrate into mitochondria, where its antihypoxic effect is realized, with a maximum concentration 1.5 hours after oral administration of the drug [6]. When studying the metabolism of Mexidol in rats, 5 metabolites were identified. The first is 3-hydroxypyridine phosphate (found only in animal liver). The second, 2-methyl-6-methyl-3-hydroxypyridine, formed in large quantities, has a spectrum of psychotropic activity close to Mexidol. The third metabolite was identified as 6-methyl-3-hydroxypyridine. The fourth metabolite is a glucuronic conjugate with 2-ethyl-6-methyl-3-hydroxypyridine. The fifth metabolite is a glucuronic conjugate with 2-ethyl-6-methyl-3-hydroxypyridine phosphate [8].
Mexidol is excreted primarily by the kidneys in the form of a glucuronic conjugate. On average, 12 hours after oral administration of the drug in humans, 0.31 ± 0.03% of the unchanged drug and 49.6 ± 4.65% of its glucuronoconjugate are excreted in the urine. In this case, excretion is most intense during the first 4 hours [9].
Since Mexidol is metabolized in the liver and excreted mainly by the kidneys, acute renal and liver failure are contraindications to the use of this drug. Mexidol has been shown to be an inducer of cytochrome P450 isoform 3A4 [10] and an inhibitor of the drug transporter protein glycoprotein-P [7]. This information must be taken into account when predicting the development of drug-drug interactions involving Mexidol. For example, since this drug is a P-glycoprotein inhibitor, it is better to combine it with rivaroxaban (an oral anticoagulant, a factor Xa inhibitor) rather than with dabigatran ethoxylate (an oral anticoagulant, a direct inhibitor of coagulation factor II). Dabigatran ethoxylate is a substrate of glycoprotein-P, so its combination with Mexidol can lead to the accumulation of an anticoagulant in the body, and accordingly, increase the risk of bleeding.
Modern ideas about the pharmacodynamics of the drug
The Mexidol molecule consists of two components: 2-ethyl-6-methyl-3-hydroxypyridine and a succinic acid residue. When creating its molecule, the researchers assumed that the drug would have antioxidant (due to the presence of 2-ethyl-6-methyl-3-hydroxypyridine) and antihypoxic (due to the succinic acid residue) activity, which was later confirmed in numerous experimental studies [ 12].
The direct antioxidant activity of 2-ethyl-6-methyl-3-hydroxypyridine is due to the presence in its molecule of a mobile hydrogen atom bound to oxygen, i.e. According to its mechanism of action, it is a proton donor. 2-ethyl-6-methyl-3-hydroxypyridine interacts with peroxy- (ROO•) and alkoxy-radicals (RO•) formed during lipid peroxidation processes according to the following mechanism [11]: AH + X*→A* + XH , where AN is Mexidol with a mobile hydrogen atom, X* is a radical initiator or intermediate radical product of free radical oxidation.
The antihypoxic activity of succinate (a succinic acid residue) is associated with the maintenance of the activity of the succinate oxidase unit under hypoxic conditions. This is a FAD-dependent link of the Krebs cycle, which under hypoxic conditions is inhibited later than NAD-dependent oxidases, which makes it possible to maintain energy production in the cell for a certain time, provided that the oxidation substrate in this link, succinate (succinic acid), is present in the mitochondria.
In recent years, it has been established that succinic acid can realize its effects, as well as the ligand of the orphan receptor GPR91 (encoded by the SUCNR1 gene), located on the cytoplasmic membrane of cells and coupled with G-proteins. This receptor is found in the kidneys (epithelium of the proximal tubules, cells of the juxtaglomerular apparatus), as well as in the liver, spleen, and blood vessels. Activation of the receptor by succinate present in the vascular bed increases the reabsorption of phosphate and glucose, stimulates gluconeogenesis, and can increase blood pressure (through an indirect increase in renin formation) [12, 13].
Subsequently, it was found that Mexidol is also capable of modulating receptor complexes of brain membranes, in particular benzodiazepine, GABA, and acetylcholine, enhancing their ability to bind to specific ligands [14].
It has been revealed that Mexidol increases the content of polar lipid fractions (phosphatidylserine and phosphatidylinositol) and reduces the cholesterol/phospholipid ratio in biomembranes, reduces their viscosity and increases fluidity, which indicates its lipid-regulating properties [15]. It has been shown that the drug can modulate the activity of membrane-bound enzymes: calcium-independent phosphodiesterase, adenylate cyclase, aldoreductase, acetylcholinesterase [16].
In vitro studies have established that Mexidol reliably suppresses both ascorbate-dependent (non-enzymatic) and NADPH2-dependent (enzymatic) iron-induced lipid peroxidation in brain homogenates, does not affect the activity of the 1-isoenzyme glutathione-S-transferase and catalase, but significantly increases activity of Se-dependent glutathione peroxidase. When studying the effect of Mexidol on the activity of NO synthases, it was revealed that the drug under study does not affect the neuronal activity, but moderately suppresses the activity of the inducible isoform [17].
Biochemical rationale for the use of Mexidol for cerebral hypoxia
The main source of energy in neurons is normally (85–90%) glucose, and the main process during which adenosine triphosphate (ATP) molecules are formed is oxidative phosphorylation, which occurs in the mitochondrial respiratory chain.
When one glucose molecule is oxidized under aerobic conditions, 38 ATP molecules are formed: 10 molecules as a result of aerobic glycolysis (4 molecules as a result of substrate phosphorylation reactions, 6 molecules in the mitochondrial electron transport chain as a result of oxidative phosphorylation during the transfer of protons and electrons from 2 molecules NADH2, formed during glycolysis); 6 ATP molecules - as a result of oxidative decarboxylation of pyruvate in the pyruvate dehydrogenase complex (ATP molecules are synthesized in the mitochondrial electron transport chain as a result of oxidative phosphorylation during the transfer of protons and electrons from 2 NADH2 molecules); 24 ATP molecules - as a result of the citrate cycle (Krebs cycle, tricarboxylic acids) (2 ATP molecules are formed from 2 glutamine triphosphate molecules, which in turn arise during the reaction of converting succinyl-CoA into succinate, 22 ATP molecules are synthesized in the mitochondrial electron transport chain as a result oxidative phosphorylation during the transfer of protons and electrons from 6 molecules of NADH2, 2 molecules of FADH2); in this case, 2 ATP molecules are spent on the phosphorylation of glucose and fructose-1-phosphate during glycolysis reactions [18].
Under normoxic conditions, the functioning of the respiratory chain, as a rule, depends on the oxidation of NAD-dependent substrates, the main supplier of reducing equivalents for the respiratory chain through the first mitochondrial enzyme complex. The contribution of this pathway in intact cells, assessed by oxygen consumption, can be up to 55–65%. However, 25–30% of mitochondrial respiration under these conditions is associated with mitochondrial enzyme complex II and succinate oxidation.
Under hypoxic conditions, there is a reversible suppression of the electron transport function of mitochondrial enzyme complex I and compensatory activation of mitochondrial enzyme complex II. At the same time, the content of succinate in the blood and tissues and the contribution of succinate oxidase to overall respiration sharply increase. The latter can reach 70–80% [13].
The binding of succinate to its specific receptors (GPR91) can trigger a cascade of biochemical reactions that also increase the body’s resistance to oxygen deficiency [13]. Increased amounts of succinate can be formed during a number of chemical reactions. For example, the aminobutyrate shunt (Roberts cycle) is activated in the brain, during which succinic acid is formed from glutamate [19]. In addition, the possibility of the formation of succinate from fumarate as a result of a reversible reaction of the Krebs cycle has been described [20], however, since this reaction consumes the FADH2 molecule, apparently, the significance of this reaction as a source of succinate under hypoxic conditions is small. It is assumed that to maintain energy processes in cells under anoxia and hypoxia, it is advisable to use substrates that can participate in the anaerobic formation of succinate, whereas under hypoxic conditions it is preferable to use succinate itself [21].
With the development of severe and prolonged hypoxia, the rate of endogenous succinate formation, apparently, may be insufficient to optimally compensate for the energy deficit. Therefore, the use of Mexidol, the molecule of which includes a succinic acid residue, to increase cell resistance to oxygen deficiency is biochemically justified, and the binding of succinic acid with 2-ethyl-6-methyl-3-hydroxypyridine increases its penetration into mitochondria [2].
As hypoxia increases, the functioning of the respiratory chain is suppressed and the main source of ATP synthesis becomes anaerobic glycolysis, the energy value of which is 2 ATP molecules [18]. Under physiological conditions, mitochondria are the main producers of reactive oxygen species. Potentially, any component of the respiratory chain under aerobic conditions, as a result of side chemical reactions, can be a donor of one-electron oxygen reduction. However, it is believed that the main sites for the generation of superoxide anion radical in the electron transport chain of mitochondria are flavoprotein, cytochrome B566 and semiubiquinone, and the most significant part of mitochondrial H2O2 is produced during O2 dismutation [22]. In this case, the number of free radicals formed is limited by the endogenous antioxidant system and is maintained at a stationary level.
Under conditions of oxygen deficiency, with an increase in the degree of reduction of respiratory chain transporters, the generation of superoxide anion radical and hydrogen peroxide increases with the participation of flavoproteins and in the ubiquinone–cytochrome C section of the electron transport chain.
During the autoxidation of coenzyme Q and the interaction of its radical with polyunsaturated fatty acids, lipid peroxidation is also activated [23]. The endogenous antioxidant system cannot cope with the increased amount of free radicals generated, which leads to the development of oxidative stress and damage to lipids, proteins, and nucleic acids.
Penetrating into mitochondria, Mexidol is able to directly bind the resulting reactive oxygen species, thus preventing the development of oxidative stress. An important role in the pathogenesis of most neurological diseases, incl. accompanied by the development of hypoxia, plays a role in the dysfunction of neurotransmitter and neuromodulatory systems, in particular the release of the excitatory mediator glutamate, which underlies the so-called. death from overexcitation or the phenomenon of excitotoxicity. When nerve cells are hypoxic, glutamate is released from the endings of neurons into the intercellular space. Its excessive accumulation activates the ionotropic NMDA and AMPA receptor subtypes, causing a massive influx of Ca2+ ions into the cytoplasm of the postsynaptic neuron. Calcium, in turn, triggers a number of processes: activation of the mitochondrial respiratory chain with increased leakage of superoxide anion radical and hydroxyl radical; activation of NADPH2 oxidase, resulting in an increase in the content of superoxide anion radical; activation of NO synthase (NOS), which leads to the accumulation of NO; activation of heme oxygenase, which converts Fe3+ to Fe2+. All of these processes intensify lipid peroxidation, and in response, the cell’s antioxidant defense system is activated. With prolonged hypoxia, its depletion is observed, which contributes to the development of oxidative stress and death of nerve cells through apoptosis or necrosis, depending on the degree of their damage [24].
In vitro studies showed that Mexidol at a final concentration in a solution of 10 to 0.1 mM reduced the level of MDA in brain homogenates exposed to L-glutamate. Since free radical reactions play a leading role in the pathogenesis of glutamate neurotoxicity, this effect can be considered as the drug’s ability to suppress glutamate excitotoxicity [17].
Generics Mexidol
Recently, the domestic pharmaceutical market has seen a significant increase in the number of generic drugs. According to statistics, their share is 77% and only 23% are original medicines. At the same time, in the USA the share of generics is only 12%, in Japan – 30%, in Germany – 35% [25]. Mexidol, according to the State Register of Medicines (https://grls.rosminzdrav.ru) for 2021, has 11 generics registered in Russia.
In a study on 14 mature male chinchilla rabbits, we studied the pharmacokinetic parameters of Mexidol and its generic mexiprim (“STADA CIS”) after their oral administration at a dose of 100 mg/kg (3 tablets/rabbit, without compromising the integrity of the tablet shell) [ 5]. It was shown that Mexidol, compared to Mexiprim, is absorbed more completely and quickly from the gastrointestinal tract, which is manifested by a significantly higher (26.1%) maximum concentration of ethylmethylhydroxypyridine succinate and a 50% shorter time to reach it (Mexidol - 30 minutes, mexiprim – 1 hour). The total clearance, half-life and average retention time of ethylmethylhydroxypyridine succinate did not differ significantly after administration of Mexidol and Mexiprim, which indicates similar elimination of the studied drugs from the body of animals.
The results obtained are consistent with the information specified in the instructions for the drugs Mexidol and Mexiprim. Thus, the maximum concentration of ethylmethylhydroxypyridine succinate in blood plasma when taking Mexidol orally in doses of 400-500 mg is 3.5-4.0 μg/ml, and when taking Mexiprim - 50-100 ng/ml.
The identified differences may be associated with differences in the production technology of the drugs (degree of grinding, level of compression pressure when pressing tablets), as well as with the presence of different excipients both in the composition of the tablet core and in their shell.
The film shell of Mexiprim tablets contains most of the components of the Mexidol shell, but it does not contain a water-soluble film-forming polymer with high adhesive and emulsifying properties - polyvinyl alcohol. This may probably be one of the reasons for the lower bioavailability of Mexiprim compared to Mexidol.
A significant difference is observed in the composition of the tablet cores of the studied drugs. For example, the core of Mexiprim tablets includes a water-insoluble filler, kaolin, which can reduce the bioavailability of the active substance due to its physical adsorption or ion exchange [26]. In the injection dosage form of Mexidol, sodium metabisulfite (sodium pyrosulfite, sodium pyrosulphite, Na2S2O5) is used as an excipient - one of the most effective and safe stabilizers [27].
Safety
Currently available clinical and preclinical data indicate a favorable tolerability and safety profile of the drug and allow Mexidol to be classified as a non-toxic or low-toxic drug. Thus, interim data from a multicenter, randomized, double-blind, placebo-controlled study of the effectiveness and safety of Mexidol (solution for intravenous and intramuscular administration/coated tablets) in parallel groups during long-term sequential therapy of patients with hemispheric ischemic stroke in the acute and early recovery periods (EPICA) indicate a favorable safety profile and good tolerability of the drug, comparable to placebo.
Data obtained during the entire period of post-registration observation confirm that the drug Mexidol - film-coated tablets and solution for intravenous and intramuscular administration, is well tolerated and safe, and when used correctly, a favorable balance between benefit and risk is maintained.
"Mexidol" in the treatment of hypertension
Simply take 1 or 2 tablets orally, monitoring the result in the form of obtaining the desired pressure readings. The therapeutic effect occurs on average within 10 minutes. The maximum daily dose should not exceed 6 tablets, which is 800 mg. Frequency of use: 2 or 3 times a day. Taking the drug in tablet form should be combined with meals.
The substance is retained in the body for 5 hours; it is metabolized in liver cells and excreted by the kidneys.
Mexidol is administered intravenously by drip, at a rate of 40 to 60 drops per minute. The total duration of the procedure is 5-7 minutes. The content of the drug in plasma is measured after 4 hours, excretion occurs by the kidneys.
For injection, the drug is used in capsules with a 5% solution of the active substance in a volume of 2 ml. By injection, the drug is administered slowly, while the liquid from the ampoule is first diluted with saline solution. The course of therapy includes a course of the drug per day of no more than 1200 mg.
The advantage of Mexidol is the possibility of using it with other drugs that have a psychotropic effect.
Taking it together with sedatives and painkillers will enhance their effect. The dosage and duration of therapy is determined by the attending physician depending on the stage of the disease.
Mexidol injection solution 5% 2ml amp 10 pcs
IM or IV (stream or drip). When administered by infusion, the drug should be diluted in 0.9% sodium chloride solution. Mexidol® is administered slowly over 5–7 minutes in a stream, and dropwise at a rate of 40–60 drops per minute. The maximum daily dose should not exceed 1200 mg.
For acute cerebrovascular accidents, Mexidol® is used in the first 10–14 days - 200–500 mg IV drip 2–4 times a day, then 200–250 mg IM 2–3 times a day for 2 weeks .
For traumatic brain injury and the consequences of traumatic brain injuries, Mexidol® is used for 10-15 days intravenously at a dose of 200–500 mg 2–4 times a day.
For dyscirculatory encephalopathy in the decompensation phase, Mexidol® should be prescribed intravenously in a stream or drip at a dose of 200–500 mg 1–2 times a day for 14 days. Then IM 100–250 mg/day over the next 2 weeks.
For a course of prophylaxis of discirculatory encephalopathy, the drug is administered intramuscularly at a dose of 200–250 mg 2 times a day for 10–14 days.
For mild cognitive impairment in elderly patients and anxiety disorders, the drug is used intramuscularly at a daily dose of 100–300 mg/day for 14–30 days.
In case of acute myocardial infarction, as part of complex therapy, Mexidol® is administered intravenously or intramuscularly for 14 days, against the background of traditional therapy for myocardial infarction, including nitrates, beta-blockers, angiotensin-converting enzyme (ACE) inhibitors, thrombolytics, anticoagulant and antiplatelet agents, as well as symptomatic means according to indications.
In the first 5 days, to achieve maximum effect, it is advisable to administer the drug intravenously; in the next 9 days, Mexidol® can be administered intramuscularly.
Intravenous administration of the drug is carried out by drip infusion, slowly (to avoid side effects) in a 0.9% sodium chloride solution or 5% dextrose (glucose) solution in a volume of 100–150 ml for 30–90 minutes. If necessary, a slow jet injection of the drug, lasting at least 5 minutes, is possible.
The drug is administered (intravenous or intramuscular) 3 times a day, every 8 hours. The daily therapeutic dose is 6-9 mg/kg body weight per day, a single dose is 2-3 mg/kg body weight. The maximum daily dose should not exceed 800 mg, single dose - 250 mg.
For open-angle glaucoma of various stages, as part of complex therapy, Mexidol® is administered intramuscularly at 100–300 mg/day, 1–3 times a day for 14 days.
For alcohol withdrawal syndrome, Mexidol® is administered in a dose of 200–500 mg intravenously or intramuscularly 2–3 times a day for 5–7 days.
In case of acute intoxication with antipsychotic drugs, the drug is administered intravenously at a dose of 200-500 mg/day for 7-14 days. In acute purulent-inflammatory processes of the abdominal cavity (acute necrotizing pancreatitis, peritonitis), the drug is prescribed on the first day both in the preoperative and postoperative periods. The administered doses depend on the form and severity of the disease, the prevalence of the process, and variants of the clinical course. The drug should be discontinued gradually only after a stable positive clinical and laboratory effect.
For acute edematous (interstitial) pancreatitis, Mexidol® is prescribed 200–500 mg 3 times a day, intravenously (in 0.9% sodium chloride solution) and intramuscularly. Mild severity of necrotizing pancreatitis - 100-200 mg 3 times a day intravenously (in 0.9% sodium chloride solution) and intramuscularly. Moderate severity - 200 mg 3 times a day intravenously (in 0.9% sodium chloride solution). Severe course - in a pulse dosage of 800 mg on the first day with a double dose regimen; then 200–500 mg 2 times a day with a gradual reduction in the daily dose. Extremely severe course - at an initial dosage of 800 mg/day until the manifestations of pancreatogenic shock are persistently relieved, after stabilization of the condition, 300-500 mg 2 times a day intravenously (in 0.9% sodium chloride solution) with a gradual decrease in the daily dosage.