For the body to function normally, blood circulation must occur continuously. The blood supply to organs and systems is ensured by the pumping function of the heart muscle, which pushes out 70 - 80 ml of blood (cardiac output) with each systole. In a minute, in an adult with a heart rate of 70 beats, the heart pumps about 5 liters of blood (and in a day - more than 7 tons!).
- Anatomical and functional features of the cardiovascular system
- Acute cardiovascular failure
- Urgent measures
- Drug therapy
- Shock
- Collapse
The main reasons for the progression of the disease under study
If collapse occurs, emergency care is indicated in the following situations:
- acute bleeding, resulting in the loss of a large amount of blood,
- serious burns,
- viral diseases,
- intoxication with certain medications,
- stressful situations; depressive mood
- acute cardiovascular failure,
- diseases in the nervous system,
- endocrine pathology.
Possible complications
- Fainting is the main complication.
- Stroke (an acutely developing disorder of cerebral circulation, accompanied by damage to brain tissue and disruption of its functions) can occur as a result of fluctuations in blood pressure.
- Fall injuries – due to dizziness and fainting
- Damage to the central nervous system, particularly the brain.
Repeated collapses lead to severe brain hypoxia (lack of oxygen supply to the brain), worsening of concomitant neurological diseases, and the development of dementia (severe intellectual disorder, manifested by deterioration of cognitive activity, attention, memory).
How does collapse occur?
The progression of the disease is quite acute. The condition is dangerous, and in the absence of timely emergency assistance in case of collapse, we can talk about serious and terrible consequences.
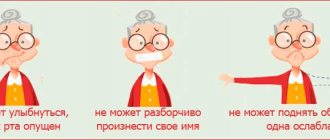
The main symptoms of the disease are:
- general weakness of the body and fatigue,
- dizziness,
- decrease in blood pressure,
- the skin becomes significantly lighter,
- decrease in temperature indicators,
- chills,
- facial features become sharper,
- dry mouth,
- loss of consciousness.
Help with collapse is urgently needed!
Anatomical and functional features of the cardiovascular system
From the left ventricle, blood enters the arterial system of the systemic circulation. Arteries contain 15% of the total circulating blood volume. These vessels carry blood to the tissues. The terminal sections of the arteries end in arterioles (resistance vessels). They perform the function of distributing blood in tissues. Thus, an increase in the tone of the arterioles (their spasm) prevents the flow of blood into the capillary pool. Tissue ischemia occurs, and blood flows into the venous system through arteriovenous anastomoses. A decrease in arteriolar tone, on the contrary, increases their lumen and enhances blood supply to tissues.
Natural vasoconstrictors (vasoconstrictors) are:
- adrenalin,
- norepinephrine,
- serotonin,
- angiotensin-2.
Under stress, the concentration of catecholamines (adrenaline, norepinephrine) in the blood increases sharply. They cause spasm of arterioles; a phenomenon of centralization of blood circulation occurs with a decrease in peripheral blood flow. The vasodilating effect is exerted by “acidic” metabolites (lactates, pyruvate, adenylic and inosinic acids), bradykinin, histamine, acetylcholine, a number of medications (neuroleptics, alpha-adrenolytics, peripheral vasodilators, ganglion blockers, etc.), some exogenous poisons, etc. Their action causes the phenomenon of decentralization of blood circulation (opening of the lumen of arterioles and redistribution of blood from the central vessels to the periphery, into the capillary bed).
Capillaries are an extensive network of the smallest vessels in the body, with a total length of 90,100,000 kilometers. About 20-25% of the capillaries function simultaneously, in which the transition of oxygen and nutrients from the blood to the tissues and the removal of “waste” metabolic products from them occurs. Periodically, with an interval of several tens of seconds, other capillaries open, where the blood is redistributed (vasomotion effect). Capillaries contain 12% of all circulating blood. However, in some pathological conditions this volume can increase several times.
The waste blood flows from the capillaries into the venous system. Veins play the role of a blood reservoir, since they contain the bulk of it (70%). They, unlike arteries, are able to change their volume, affecting the flow of blood to the heart.
The most important hemodynamic indicator of the venous system is central venous pressure (CVP). This is the pressure that blood exerts on the walls of the vena cava and the right atrium. It is an integral indicator of circulating blood volume, vascular tone and pumping function of the heart. CVP is measured with a phlebotonometer. Normally it is 60-120 mm of water column.
Central venous pressure decreases when:
- blood loss;
- excessive loss of water (hypohydration);
- decreased tone of arterioles and veins.
This reduces the volume of blood flowing to the heart and, accordingly, reduces cardiac output. With negative CVP values, there is a danger of circulatory arrest. Venous pressure increases when:
• heart failure (left and right ventricular);
• excessive infusion of blood and other fluids;
• obstruction of blood flow from the right ventricle of the heart (pulmonary embolism).
When the CVP is more than 150-160 mm Hg. against the background of left ventricular failure, patients may develop pulmonary edema. An integral indicator of the hemodynamics of the arterial part of the vascular system is blood pressure (systolic, diastolic, pulse and average). Systolic and diastolic blood pressure are measured with a tonometer using the Korotkoff method. Pulse blood pressure is the difference between systolic and diastolic.
The value of blood pressure is influenced by the volume of cardiac output and the resistance of peripheral vessels (arterioles). This dependence is directly proportional. Therefore, you can increase a patient’s blood pressure in the following ways:
- introduce vasoconstrictor agents (adrenaline solution, mezaton, etc.);
- increase the volume of circulating blood (by transfusion of polyglucin, refortan, etc.);
- improve the functional ability of the myocardium (by introducing cardiac glycosides, etc.).
The total blood volume in humans is about 7% of body weight: in men 70 ml/kg, in women - 65 ml/kg. The circulating blood volume (CBV) is somewhat smaller, since part of the blood does not participate in the circulation, being in the vascular depot. BCC can be measured by injecting a known concentration of a substance into the bloodstream, for example, Evans blue or polyglucin, and determining the degree of its dilution. So, measurements of central venous pressure, blood pressure, cardiac output and blood volume in patients make it possible to identify the characteristics of circulatory disorders and carry out adequate corrective therapy.
Symptoms
The disease occurs completely unexpectedly. Initially, weakness and dizziness occur, and the patient is thirsty. The skin becomes lighter than its normal state, profuse cold sweating appears on it, characterized by chills. The pulse becomes slower, the pressure decreases significantly, and shortness of breath is also observed. Among other things, you may notice deterioration in vision, the appearance of extraneous sounds in the ears, and the person may be worried about something. As the disease progresses, a person's thoughts become confused, his pupils dilate, and his heart beats much faster.
symptoms of collapse
Diagnostics
Orthostatic hypotension is detected if, after 2-5 minutes of quiet standing, the patient has the following symptoms:
- there is a decrease in systolic pressure (this is the first heard beat of the heart during the smooth deflation of air from the inflated cuff when measured with a tonometer) by 20 mm or more;
- a decrease in diastolic pressure (this is the level of cessation of heart sounds during the smooth deflation of air from an inflated cuff when measured with a tonometer) by 10 mm or more;
- orthostatic collapse, dizziness or other symptoms of decreased blood pressure when changing body position.
Prevention and treatment
If you are wondering what is the sequence of first aid for collapse , then we offer you the following recommendations:
- The pathology in question implies a phenomenon that requires immediate intervention by specialists. People who happen to be nearby when the disease progresses should change the position of the patient during collapse and put him on the bed, raise his legs and cover him with a warm blanket to prevent him from freezing.
- In a short period of time, you need to find the cause of the decrease in pressure and get rid of it: stop heavy bleeding, give the person the necessary medications, and so on.
- At this time, it is also necessary to provide for parenteral infusion of blood components or mixtures that serve as a replacement for blood.
- In some particularly dangerous situations, it is necessary to carry out resuscitation measures to help save the patient’s life.
Prevention of this disease is reflected in properly selected treatment of those pathologies that can cause the development of collapse, in systematically undergoing a medical examination and taking into account the side effects of medications taken. Now you know the difference between collapse and fainting , and how to provide first aid.
Emergency care for collapse
To successfully relieve the syndrome, the following algorithm was developed:
- Call an ambulance.
- Place the victim on a hard surface (table, asphalt road) and raise his legs using a cushion of clothing (this will increase blood flow to the heart and brain).
- Unbutton the collar of a tight-fitting shirt/blouse to facilitate breathing.
- Open the windows and door to ventilate the room.
- Since during collapse there is a decrease in body temperature, it is very important to warm the patient. If he is conscious, give him hot tea or coffee to drink; if not, wrap it in a warm blanket and put a heating pad on it.
- Wet a cotton swab with ammonia and bring it to the nose, rub the patient’s temples and earlobes.
- If possible, administer a solution of adrenaline and ephedrine.
NotaBene! In a collaptoid state, it is strictly prohibited:
- bring the patient to his senses by patting the cheeks;
- place a pill in the victim’s mouth or pour water into it if he is unconscious;
- giving heart medications - the popular nitroglycerin or validol, on the contrary, dilates blood vessels.
Reasons leading to the development of a collaptoid state
To date, the etiology of collapse has been well studied, which allows us to identify the main causes of its occurrence as a result of exposure to the body:
- infectious agents (causative agents of dysentery, botulism, meningoencephalitis, typhoid fever, influenza, and so on);
- massive blood loss (for example, as a result of injury, bleeding from a gastric or duodenal ulcer, from esophageal varices);
- severe burns;
- severe dehydration;
- toxins, poisons (especially cyanide, carbon monoxide, organophosphorus compounds);
- medications (most often antihypertensive, antiarrhythmic, b-blockers, as well as local anesthetics when released into the general bloodstream);
- various physical factors (too high or too low temperature, electric current, radioactive radiation):
- allergens (in case of development of an anaphylactic reaction);
- a decrease in venous tone, which leads to the development of orthostatic collapse (occurs after prolonged bed rest, a long-term serious illness, certain diseases of the endocrine system, and sometimes occurs in the postoperative period).
Almost everyone has encountered a condition (if not personally, then seen something similar in a film or read in literature) when a person who stood up quickly suddenly falls, “settles,” and becomes weaker. This is the so-called orthostatic collapse, which develops as a result of redistribution of blood flow, an increase in the vascular venous bed (due to decreased tone of the vein walls) and a significant decrease in the return of blood back to the heart.
Photo: https://pixabay.com/photos/medications-money-cure-tablets-257336/
In addition to the listed pathological factors, various acute diseases or chronic diseases in the deteriorating stage play an important role:
- cardiovascular - acute myocardial infarction, pulmonary embolism, severe heart rhythm disturbances (including pacemaker dysfunction), dissecting aortic aneurysm, artificial heart valve dysfunction, acute myocarditis, pericarditis and others;
- severe pneumonia;
- acute pancreatitis and so on.
Orthostatic collapse: should it be treated or will it outgrow?
A wait-and-see attitude with regular fainting is not justified. Sooner or later, the teenager will grow up and all regulatory functions will return to normal. But fainting significantly complicates life and deprives the child of the opportunity to play sports and be active. Poor blood circulation leads to oxygen starvation of the brain, which has a bad effect on learning. With vegetative-vascular dystonia, prolonged absence of treatment perpetuates distorted regulatory mechanisms and subsequently negatively affects overall health and brain function.
Treatment of orthostatic collapse includes physical therapy and medications that improve autonomic regulation. Intense physical activity is not recommended, since after unusually high stress there may be overcompensation, which will lead to an even greater decrease in blood pressure.
Long-term intake of the amino acids cystine, glycine, and glutamic acid helps improve tissue metabolism and gently establish autonomic regulation. During the process of active growth, amino acid support facilitates the body’s adaptation to new conditions. Cystine, glycine and glutamic acid are part of the drug Eltacin®, which is recommended from 12 years of age to correct vegetative-vascular dystonia and ease the transition period in adolescents.
How does hypovolemic hypotension develop?
Hypovolemic hypotension is possible in subacute and acute forms. The development of the subacute form occurs due to an imbalance and lack of compensation for fluid loss.
- With blood (bleeding, heavy periods in women) there is a loss of formed elements and plasma. The human body must constantly maintain a circulating blood volume of 66–70 ml per kg of body weight. Plasma accounts for about 40 ml/kg. If a moderate loss of red blood cells and other cells does not affect health over a long period of time, then the liquid portion should be compensated only by drinking.
- Fluid losses during breathing and sweating are considered “hidden” because they are constant and relatively small (500 ml/day) in comparison with circulating plasma. But with fever, increased sweating (in hot climates, when working near stoves, in a steam room, in the case of heavy physical activity), this volume increases significantly and affects blood circulation. A similar mechanism of fluid loss through the skin and respiratory tract is observed with massive burns and artificial ventilation.
- Water leaves with urine when there is a high content of glucose, protein, and nitrogenous substances, which are caused by excessive consumption of protein foods, changes in the filtration properties of the kidney tissue in kidney disease, and diabetes mellitus. In this situation, in addition to impaired protein and glucose metabolism, the fluid balance changes negatively, since water is also lost with high concentration urine.
- With vomiting and diarrhea in case of frequent repetitions and insufficient fluid intake, this is especially true for the child’s body. During the day, up to 7.5 liters of liquid are formed in the gastrointestinal structures, up to 2 liters are supplied with food, and only 200 ml are lost through emptying.
- Redistribution of the liquid part of the blood due to insufficient content of electrolytes, potassium salts, calcium, sodium, iron, phosphorus occurs with damage to the adrenal glands and impaired hormone synthesis. This picture develops in a state of shock, in sensitive people against a background of stress and anxiety.
All of the above forms of hypovolemia reduce the total amount of blood. The brain is one of the first to respond to deficiency with symptoms of orthostatic hypotension.
Other factors
There is compelling evidence supporting attenuation of the baroreflex response as a mechanism responsible for ON and FCI. It is noted that heat stress may promote this response. However, several other factors have been studied that could also aggravate the reaction.
A weakening of the sensitivity of the baroreflex during hypoglycemia was found. This is important because serum glucose levels decrease with increasing exercise duration, which may increase the susceptibility of endurance and ultra-endurance athletes to CPT (36). Striving for a target time or a high pace is also associated with CF (30). When trying to achieve a final or temporary goal, the breathing rate increases, as a result, the athletes' carbon dioxide concentration decreases. Studies show a protective effect of hypercapnia (37) and the resulting hypocapnia further impairs the baroreflex (38).
Taking medications may influence the response to LBCI: taking antidepressants is a possible factor in CFN because it significantly impairs the reflex cardiovascular response to exercise by altering neurochemical reactions (39). In addition, in two independent randomized controlled clinical trials, H1 and H2 receptor antagonists blunted post-exercise hypotension, suggesting that histamine may also play a role in CEF (40, 41) (Table 4).
Table 4. Other factors
| Source | Author/journal | Year | Type of study | Patients | results | UD |
| 36 | Adler et al Diabetes | 2009 | Clinical trial | 20 men | Previous hypoglycemia impairs baroreflex sensitivity and hypotensive stress response | 2 |
| 37 | Howden et al Exp Physiol | 2004 | Case-control | 9 subjects | Increased arterial CO2 is associated with increased cerebral blood flow | 3 |
| 38 | Lucas et al J Appl Physiol | 2008 | Cross | 9 men | Postural hypotension and hypocapnia exacerbate cerebral hypoperfusion during prolonged exercise | 3 |
| 39 | Middleton et al Eur J Clin Pharmacol | 1987 | Case-control | 7 women and 7 control group | Significant impairment of the cardiovascular reflex response when taking antidepressants | 3 |
| 40 | Lockwood et al J Physiol | 2005 | Randomized controlled trial | 14 healthy men and women | H1 receptor antagonists reduce post-exercise vasodilation and blunt post-exercise hypotension | 1 |
| 41 | McCord et al J Appl Physiol | 2006 | Randomized controlled trial | 10 healthy men and women | H2 receptor antagonists reduce post-exercise vasodilation and blunt post-exercise hypotension | 1 |
| LE - level of evidence | ||||||
Baroreflex modulation
Blood retention in the lower extremities after cessation of physical activity is a proposed mechanism for CFN. If, after cessation of exercise with an intact baroreflex, the systemic vascular resistance reduced by exercise does not increase, lower body negative pressure (LBNP) may develop and postural hypotension may occur. Many studies of the effects of LBNT have shown baroreflex impairment as a major mechanism of ON after exercise. Decreased baroreflex control is associated with a decrease in orthostatic response after exercise (31). A controlled trial with exercising men showed impaired baroreflex control after dynamic exercise (32). Additionally, a clinical trial of 51 people who completed a mountain marathon found that decreased orthostatic resistance vascular response was a likely etiology of ON in these runners after exercise (33). In a clinical trial with experienced runners, systolic blood pressure decreased after exercise secondary to a decrease in peripheral vascular resistance, which resulted in a decrease in filling volume (34). However, women may have different reactions than men. A controlled clinical trial in women and men showed that the mechanism of ON in women is likely due to decreased cardiac filling rather than an abnormal baroreflex (35) (Table 3).
Table 3. Baroreflex modulation
| Source | Author\magazine | Year | Type of research | Patients | results | UD |
| 31 | Murrell et al J Appl Physiol | 2007 | Clinical trial | 7 athletes | Post-exercise hypotension and postural decline in autonomic function or baroreflex control puts the brain at risk of hypoperfusion | 2 |
| 32 | Halliwill et al J Physiol | 1996 | Controlled test | 9 men | Baroreflex control of vascular resistance from sympathetic activity is impaired after exercise | 2 |
| 33 | Gratze et al Eur Heart J | 2008 | Clinical trial | 51 men | Post-exercise OH is associated with high baseline sympathetic modulation of vasomotor tone coupled with a decrease in the orthostatic response of resistive vessels | 2 |
| 34 | Privett et al Br J Sports Med | 2010 | Clinical trial | 10 experienced runners | After prolonged exercise, as a result of insufficient compensation for the decrease in stroke volume, SBP decreases and filling volume falls. | 2 |
| 35 | Fu et al Am J Phsiol Heart Circ Physiol | 2004 | Controlled | 10 women and 13 men | A decrease in OH in women is associated with a decrease in heart filling, and not with a decrease in vascular resistance, as in men | 2 |
| LE – level of evidence; OH – orthostatic intolerance; SBP is systolic blood pressure. | ||||||
How does orthostatic hypotension manifest?
Patients with orthostatic hypotension complain of the following symptoms:
- general weakness;
- dizziness even when sitting;
- blurred vision;
- cramps in the limbs;
- tendency to faint;
- hearing loss;
- increased sweating.
Particularly poor health occurs against the background of prolonged standing or sitting in one position, trying to get up, or getting out of bed.
Tightening the corset at one time made it possible for ladies to look pale and sensitive due to the orthostatic mechanism of hypotension
The role of heat and dehydration
Dehydration causing hyperthermia has been implicated as a major contributor to CFI (5–7), but there is no evidence to support its overall responsibility for ON or CFI in endurance athletes (25). However, existing evidence supports that heat stress and elevated skin temperature are contributing factors to ON. Heat stress leads to decreased baroreflex control of the response to orthostatic stress (26). Heat stress is also thought to impair aerobic exercise performance, primarily by increasing cardiovascular strain (27). In addition, an increase in body temperature may increase cerebral vascular resistance, lowering the cerebral threshold for neurogenic collapse (28).
Table 1. Mechanisms
| Source | Author/magazine | Year | Type of study | Patients | Result | UD |
| 16 | Morikawa et al Med Sci Sports Exerc | 2001 | Controlled test | 26 runners, 23 peers, control | Trained women with a high level of orthostatic intolerance in ADNT. Increasing vascular compliance plays an important role | 2 |
| 17 | Levine et al Circulation | 1991 | Controlled test | 7 athletes and 6 control group | Endurance athletes have greater diastolic chamber compliance and distensibility than non-athletes | 2 |
| 18 | Levine et al J Appl Physiol | 1991 | Controlled test | 8 high trained, 8 moderate trained and 8 low trained | Calf vascular compliance and carotid baroreflex response contribute to individual response to LBNT | 2 |
| 19 | Esch et al Am J Physiol Heart Circ Physiol | 2007 | Controlled test | 8 athletes and 8 control group | Endurance athletes have a greater increase in end-diastolic volume than non-athletes, with a similar area of the right ventricular cavity | 2 |
| 20 | Esch et al J Appl Physiol | 2010 | Controlled test | 8 athletes and 8 control group | Endurance athletes have a reduced rate of left ventricular untwisting compared to non-athletes | 2 |
| 21 | Convertino Med Sci Sports Exerc | 2003 | Controlled test | 8 men | Vascular expansion is associated with a decrease in heart rate response to baroreflex stimulation | 2 |
| 22 | Ogoh et al J Appl Physiol | 2006 | Controlled test | 8 men | The cardiopulmonary baroreflex is readjusted to a new operating point associated with the exercise-induced change in ventricular filling volume | 2 |
| 23 | Ogoh et al J Physiol | 2003 | Controlled test | 14 men | Highly trained individuals rely more on maintaining venous return to maintain an upright body position | 2 |
| 24 | Convertino Med Sci Sports Exerc | 1993 | Critical review | — | Increasing stroke volume is the primary compensation mechanism in endurance-trained individuals. | 3 |
| NPLP – negative pressure in the lower part of the body; LE – level of evidence. | ||||||
Two small studies have found changes in baroreflex control of blood pressure in individual subjects from laboratory-induced hypovolemia, which increases sensitivity to CFP (22, 29). However, a larger body composition-controlled clinical study of 31 ultra-marathon runners did not find higher temperatures in subjects with collapse compared to those without collapse. All runners were dehydrated, but the amount of dehydration was not related to the degree of postural hypotension after the event (30) (Table 2). Therefore, heat and dehydration have not been recognized as the true causes of CFI or ON in endurance events, but they may be risk factors for CFI or contribute to impaired peripheral vasoconstriction leading to an orthostatic state.
Table 2. Dehydration/heat
| Source | Author\magazine | Year | Type of study | Patients | Result | UD |
| 23 | Ogoh et al J Physiol | 2003 | Clinical trial | 14 men | During endurance training, the baroreflex is weakened in response to a progressive decrease in central blood volume. | 2 |
| 26 | Crandall Am J Physiol Heart Circ Physiol | 2000 | Controlled test | 12 people | Decreased baroreflex, along with decreased ability to increase heart rate, increases sensitivity to OH | 2 |
| 27 | Cheuvront et al J Appl Physiol | 2010 | Critical review | — | Dehydration increases hyperthermia and decreases plasma volume, which increases cardiovascular stress | 3 |
| 28 | Wilson et al Am J Physiol Regul Integr Com Physiol | 2006 | Controlled test | 15 men | Heat stress reduces cerebral blood flow velocity and increases cerebral vascular resistance | 2 |
| 29 | Charkoudian et al J Physiol | 2003 | Controlled test | 13 healthy people | Exercise-induced dehydration leads to changes in baroreflex control of blood pressure | 2 |
| 30 | Holtzhausen et al Med Sci Sports Exerc | 1995 | Clinical trial | 31 runners | All runners had a decrease in fluid volume (on average by 4.6%), 68% developed asymptomatic PHFN, dehydration did not worsen the condition of the cardiovascular system | 2 |
| PPHH – postural exercise hypotension; LE – level of evidence; ON – orthostatic intolerance | ||||||
The role of medications
It is necessary to treat heart and vascular diseases with medications taking into account concomitant pathology. It determines individual sensitivity and requires a gradual selection of dosage.
Ambulances make daily calls to respond to calls regarding negative reactions to medications in hypertensive patients. The most common drop in blood pressure is observed when taking:
- large doses of fast-acting diuretics (Lasix, Furosemide);
- nitro drugs prescribed for angina pectoris (Nitroglycerin, Erinit);
- centrally acting antihypertensive drugs (Clonidine);
- any drugs prescribed for the treatment of hypertension in high dosages or in inappropriate combinations;
- Dopamine in patients with parkinsonism.
You should carefully read the instructions for taking the drug and do not exceed the prescribed dosage. If negative effects occur, consult a doctor.
This tea should not be drunk unless specifically indicated.
Unfortunately, some women try to lose weight using diuretics. It should be remembered that all tablets and teas recommended for this purpose necessarily include diuretics and laxatives. A thoughtless attitude towards your body contributes to the development of dysregulation of cerebral vascular tone.
Orthostatic hypotension accompanies other symptoms of marijuana-derived drug use.
We recommend that you learn more about orthostatic hypotension and its differences from fainting from this article.