If an attack (paroxysm) of atrial fibrillation lasts longer than two days, the risk of blood clots and the development of ischemic stroke increases sharply. With a constant form of arrhythmia, chronic circulatory failure can progress.
According to statistics, atrial fibrillation accounts for 30% of all hospitalizations associated with arrhythmia. The disease occurs more often in elderly patients over 60 years of age.
Classification of atrial fibrillation
Taking into account the characteristics of the clinical course, electrophysiological mechanisms and etiological factors, cardiologists classify the disease as follows:
- chronic or permanent form of atrial fibrillation (symptoms remain pronounced, electrical cardioversion is ineffective);
- persistent form of atrial fibrillation (lasts more than a week);
- transient or paroxysmal form of atrial fibrillation (the attack lasts from 1 to 7 days).
Persistent and paroxysmal forms of atrial fibrillation are often recurrent. They also distinguish between a newly diagnosed attack of atrial fibrillation and a recurrent one.
Atrial fibrillation and flutter
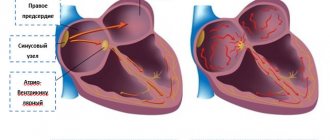
The disease can occur in two different types of atrial disorders - fibrillation and atrial flutter. During fibrillation, only individual groups of muscle fibers contract, resulting in no coordinated contraction. As a result, a large number of electrical impulses are concentrated in the atrioventricular connection. Some of them spread to the ventricular myocardium, others are delayed.
Based on the frequency of ventricular contractions, atrial fibrillation comes in three forms:
- bradysystolic (less than 60 ventricular contractions per minute);
- normosystolic (from 60 to 90 contractions);
- tachysystolic (more than 90 ventricular contractions per minute).
In paroxysmal atrial fibrillation, blood is not pumped into the ventricles. The atria do not contract effectively enough, which is why at the moment of relaxation (diastole), the ventricles are only partially filled with blood. Consequently, the release of blood into the aortic system does not always occur.
With flutter, rapid atrial contraction is noted (200 - 400 per minute), the correct coordinated atrial rhythm is maintained. In this case, myocardial contractions follow each other almost without interruption, the diastolic pause practically does not occur, the atria cannot relax and are in a state of systole most of the time. They are not completely filled with blood, and its flow into the ventricles decreases.
Causes
The main cause of atrial fibrillation is a malfunction of the conduction system of the heart, which causes a disturbance in the order of heart contractions. In such a situation, muscle fibers do not contract synchronously, but in discord; the atria cannot make one powerful push every second and instead tremble, not pushing the required amount of blood into the ventricles.
The causes of atrial fibrillation are conventionally divided into cardiac and non-cardiac. The first group includes:
- High blood pressure. With hypertension, the heart works harder and pushes out a lot of blood. The heart muscle cannot cope with the increased load, stretches and weakens significantly. Disturbances also affect the sinus node and conduction bundles.
- Valvular heart defects, heart diseases (cardiosclerosis, myocardial infarction, myocarditis, rheumatic heart disease, severe heart failure).
- Congenital heart defects (insufficient development of blood vessels feeding the heart, poor formation of the heart muscle are noted).
- Heart tumors (cause disturbances in the structure of the conduction system and do not allow impulses to pass through).
- Previous heart surgery. In the postoperative period, scar tissue may form, which replaces the unique cells of the cardiac conduction system. Because of this, the nerve impulse begins to travel along other paths.
The group of non-cardiac causes includes:
- physical fatigue;
- bad habits, alcohol;
- stress;
- large doses of caffeine;
- viruses;
- thyroid diseases;
- taking certain medications (diuretics, adrenaline, Atropine);
- chronic lung diseases;
- diabetes;
- electric shock;
- sleep apnea syndrome;
- electrolytic disturbances.
Symptoms of atrial fibrillation
Symptoms of atrial fibrillation depend on:
- myocardial conditions;
- forms of the disease;
- features of the valve apparatus.
The worst case for patients is the tachysystolic form of atrial fibrillation. They experience:
- dyspnea;
- cardiopalmus;
- heartache;
- feeling of a sinking heart;
- pulsation of neck veins.
Typical cases of the disease are characterized by:
- sweating;
- randomness of heartbeats;
- unreasonable fear;
- shiver;
- polyuria.
If the heart rate is very high, Morgagni-Adams-Stokes attacks and fainting appear. As soon as sinus heart rhythm is restored, these symptoms disappear.
Over the years, those suffering from a chronic (permanent) form of atrial fibrillation generally cease to notice it.
If you experience similar symptoms,
consult your doctor . It is easier to prevent a disease than to deal with the consequences.
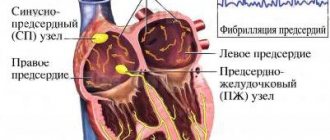
What causes atrial fibrillation?
What causes atrial fibrillation?
Normally, the upper chambers of the heart (atria) and lower chambers (ventricles) work in sequence due to the action of the sinus node. The master pacemaker produces electrical signals that cause the heart to contract and pump blood. It is the sinus node that provides the correct and regular rhythm with a heart rate of 50–100 beats per minute. In atrial fibrillation, the sinus node does not participate in the excitation of the myocardium, and multiple foci of chaotic electrical activity cause electrical chaos in the heart, causing the atria to beat at a frequency of 350 to 600, and the ventricles up to 200 beats per minute. It can be characterized as chaotic atrial activity.
Diagnostics
Diagnosis of atrial fibrillation includes:
- Analysis of patient complaints and anamnesis. It is determined when the interruptions in heart function began, whether chest pain occurs, or whether fainting occurred.
- Life history analysis. The doctor examines whether the patient has undergone any operations, whether he has chronic diseases or bad habits. It is also clarified whether any of the relatives suffered from heart disease.
- General blood test, urine test, biochemistry.
- Physical examination. The condition of the skin and its color are assessed. It is determined whether there are heart murmurs or wheezing in the lungs.
- Hormonal profile (carried out to study the level of thyroid hormones).
- Electrocardiography. The main ECG sign of atrial fibrillation is the absence of a wave, which reflects the normal synchronous contraction of the atria. Irregular heart rhythm is also detected.
- Holter monitoring of the electrocardiogram. The cardiogram is recorded over 1-3 days. As a result, the presence of asymptomatic episodes, the form of the disease, and the conditions contributing to the onset and termination of the attack are determined.
- Echocardiography. Aimed at studying structural cardiac and pulmonary changes.
- Chest X-ray. Shows increased size of the heart, changes that have occurred in the lungs.
- Treadmill test or bicycle ergometry. Assumes the use of stepwise increasing load.
- Transesophageal echocardiography. A probe with a special ultrasound sensor is inserted into the patient's esophagus. The method makes it possible to detect blood clots in the atria and their appendages.
How is atrial fibrillation diagnosed?
How is atrial fibrillation diagnosed?
Atrial fibrillation can be detected using an electrocardiogram. However, the arrhythmia may not be constant and the electrocardiogram at a given time will be normal. For long-term recording of an electrocardiogram if atrial fibrillation is suspected, Holter monitoring is used. It is a portable device that is worn continuously for one to several days to record long-term electrocardiograms.
Treatment of atrial fibrillation
Treatment of atrial fibrillation is aimed at:
- restoration, maintenance of sinus rhythm;
- relapse prevention;
- heart rate control.
Treatment of the paroxysmal form of atrial fibrillation involves the use of:
- "Novocainamide";
- "Cordarona";
- "Quinidine";
- "Propanorma".
Medicines are taken under constant monitoring of blood pressure and ECG. Also, for paroxysmal atrial fibrillation, Anaprilin, Digoxin, and Verapamil can be prescribed. These medications provide a less pronounced effect, but also improve the patient's well-being and reduce the heart rate.
If drug treatment does not produce positive results, electrocardioversion is used. A pulsed electrical discharge is applied to the heart area, which stops the attack.
If the paroxysm lasts longer than 2 days, anticoagulant therapy for atrial fibrillation (Warfarin) is carried out to avoid the formation of blood clots. For preventive purposes, when sinus rhythm has already been restored, Propanorm, Cordarone Sotalex, etc. are used.
Treatment of permanent atrial fibrillation involves long-term use of:
- "Digoxin";
- adrenergic blockers (“Egilok”, “Atenolol”, “Concor”);
- "Warfarin";
- calcium antagonists (Verapamil, Diltiazem).
Surgical treatment of atrial fibrillation
Surgical treatment of atrial fibrillation is carried out if:
- antiarrhythmic therapy was ineffective;
- relapse prevention;
- During paroxysms, circulatory disturbances occur.
Most often, cardiologists use the following surgical treatment methods:
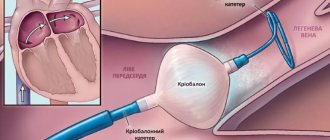
- Radiofrequency ablation of sources of atrial fibrillation. A special thin tube is passed through the femoral vessels to the heart. A radiofrequency pulse is sent through it, which eliminates possible sources of arrhythmia.
- Radiofrequency ablation of the atrioventricular node and installation of a pacemaker. The operation is performed if a chronic form of fibrillation is diagnosed and it is not possible to obtain a normal heart rate with the help of medications. This is a last resort. The radiofrequency pulse completely destroys the node responsible for transmitting the impulse from the atria to the ventricles. To ensure normal heart function, a pacemaker is installed, which supplies electrical impulses to the heart and creates a normal artificial rhythm.
- Installation of an atrial cardioverter-defibrillator. A cardioverter defibrillator is a device that is sewn under the skin in the upper chest. An electrode goes from it to the heart. The device blocks attacks of atrial fibrillation instantly by delivering electrical shocks.
- Open heart surgery. It is carried out if there are other serious heart diseases. At the same time, the sources of atrial fibrillation are affected in parallel.
Treatment of atrial fibrillation with folk remedies
Traditional medicine recipes can be used to normalize heart rate:
- Hawthorn tincture (sold in pharmacies). Take 20 drops 2-3 times a day.
- Infusion of viburnum fruits. 1 tbsp. l. pour a glass of boiling water over the viburnum fruit. Simmer over low heat for 5 minutes. Strain. Drink half a glass 2 times a day after meals.
- Infusion of dill seeds. Pour 1/2 teaspoon of seeds into a glass of boiling water. Leave for 30 minutes. Strain. Drink the resulting portion in three doses. You can add natural honey to the infusion.
Etiology of AF and cardiovascular risks
Atrial fibrillation is defined as a supraventricular tachyarrhythmia characterized by chaotic electrical activity of the atria at a high rate (350-700 per minute) and an irregular ventricular rhythm1. Previously, the term “atrial fibrillation” was widely used, which quite accurately conveys the essence of atrial fibrillation.
According to foreign studies, AF is the most common form of tachyarrhythmia in the world and occurs in 2% of the population2. There are valvular and non-valvular AF (NVAF). In the first case, AF is associated with damage to the heart valves and overload of the left atrium with pressure or volume, due to which fibrillation begins. The most common cause of valvular AF is rheumatic mitral valve stenosis or replacement1. All other cases of atrial fibrillation are defined as non-valvular.
NFP occurs against the background of a number of diseases and conditions, such as coronary heart disease, hypertension, primary myocardial diseases, diabetes mellitus, pheochromocytoma, as well as alcohol abuse, excess body weight and hypokalemia3. Due to the chaotic movement of blood in the fibrillating left atrium, the prerequisites are created for the formation of blood clots, which can spread through the left ventricle throughout the systemic circulation. Thromboembolic complications are the most dangerous complications of AF. These include:
- ischemic cardioembolic stroke;
- heart attacks of internal organs;
- thromboembolism of the vessels of the extremities.
In a cardioembolic stroke, an embolus (thrombus) located in the left atrium breaks off and enters the arterial system of the brain.
According to a number of epidemiological studies, NFP increases the risk of stroke by 2.6-4.5 times, depending on the clinical parameters of patients4. Moreover, for women, these risks, other things being equal, are higher than for men5.
A stroke that occurs during NAF is severe and more often leads to disability than a stroke in patients without AF6. The basis for the prevention of thromboembolism in NFP is oral anticoagulants. They reduce the activity of blood clotting and thus prevent the formation of emboli (blood clots). 10 years ago, the drug of choice was the vitamin K antagonist warfarin, but direct oral anticoagulants (DOACs) appeared, in particular apixaban, which have a number of advantages over warfarin, which allowed DOACs to become the standard for stroke prevention in NAF.
Diet
With atrial fibrillation, the patient should eat foods rich in vitamins, microelements and substances that can break down fats. This means:
- garlic, onion;
- citrus;
- honey;
- cranberry, viburnum;
- cashews, walnuts, peanuts, almonds;
- dried fruits;
- dairy products;
- sprouted wheat grains;
- vegetable oils.
The following should be excluded from the diet:
- chocolate, coffee;
- alcohol;
- fatty meat, lard;
- flour dishes;
- smoked meats;
- canned food;
- rich meat broths.
Apple cider vinegar helps prevent blood clots from forming. 2 tsp. You need to dilute it in a glass of warm water and add a spoonful of honey. Drink half an hour before meals. The preventive course is 3 weeks.
Prevention
Primary prevention of atrial fibrillation involves proper treatment of heart failure and arterial hypertension. Secondary prevention consists of:
- compliance with medical recommendations;
- conducting cardiac surgery;
- limiting mental and physical stress;
- giving up alcoholic drinks and smoking.
The patient must also:
- eat rationally;
- control body weight;
- monitor blood sugar levels;
- do not take medications uncontrollably;
- measure blood pressure daily;
- treat hyperthyroidism and hypothyroidism.
This article is posted for educational purposes only and does not constitute scientific material or professional medical advice.