Most often, sudden cardiac death occurs outside a medical institution, with 80% of cases occurring in public and work places where there is no possibility of providing emergency resuscitation care [1, 2].
The probability of survival in patients with ventricular fibrillation, according to modern literature, decreases by 7–10% in each subsequent minute. Primary resuscitation measures (ABC) cannot convert fibrillation into hemodynamically effective heart contractions in such patients without electrical pulse therapy (EPT). Therefore, early defibrillation in such situations is a chance to restore an effective heart rhythm, i.e. save the patient's life.
In recent years, there has been increasing support among experts for the concept of early defibrillation using an automatic external defibrillator (AED). This concept implies the presence of AEDs in public places (airports, supermarkets, educational institutions, etc.), which will allow even an unqualified eyewitness to help a patient with sudden cardiac arrest before the arrival of an emergency medical team (EMS).
I would like to remind the reader that electropulse therapy is a procedure for stopping cardiac arrhythmias (arrhythmias) by exposing the myocardium to an electrical discharge. There are two types of EIT: defibrillation and synchronized electrical cardioversion (ECV). These two types of EIT differ significantly in the mechanism for applying an electric discharge.
Defibrillation is the application of a pulse of direct electrical current with sufficient energy to depolarize the myocardium, which allows the first order pacemaker to resume control of the heart rhythm. Defibrillation is one of the integral components of resuscitation measures and should be carried out, if necessary, by nursing staff.
Electrocardioversion is the effect of a direct electric current pulse on the myocardium, synchronized with the least vulnerable phase of the electrical systole of the ventricles. Electrocardioversion can be planned - restoring the rhythm with stable hemodynamics, when preparing the patient for the procedure, and emergency - performed for various tachyarrhythmias with unstable hemodynamics.
Defibrillators-cardioverters
A defibrillator is a device that generates a single charge of direct electrical current that can be passed through the myocardium to eliminate ventricular fibrillation.
An automatic external defibrillator is a device that generates a single charge of direct electrical current and is used to conduct an electrical impulse through the chest wall to the heart. The AED is a computer that evaluates the patient's heart rhythm and decides whether EIT is necessary. Specificity in recognizing the rhythm subject to EIT approaches 100%. Currently, AEDs guide unskilled rescuers through the entire resuscitation process, from assessing the patient's viability to performing CPR. The AED operation protocol includes a sequence of visual and voice prompts that are aimed at helping the rescuer during resuscitation, and also has a function for recording the course of events, which allows you to subsequently retrospectively analyze the use of the device. The effectiveness of AEDs has been proven and recommended for use by the ERC (2010) [4].
An implantable defibrillator cardioverter ( IDC) is The IDK constantly monitors the patient’s heart rhythm and, when life-threatening arrhythmias are detected, stops them using differentiated electrical impulses. The choice of electrical impulse by the device depends on the type of rhythm disturbance. Heart rate analysis and therapy takes seconds for the IDC. The effectiveness of the device has been confirmed by SMASHVT studies [5] in the USA and Europe. IDC can significantly prolong the life of patients with episodes of hemodynamically ineffective rhythms. The need to replace the device every 5–8 years (Gem III VR, Maximo VR).
Cardioverter is a complex of a defibrillator and an electronic synchronizer device, which makes it possible to deliver a discharge at a certain phase of the electrical systole of the ventricles (usually 20–30 ms after the apex of the R wave). When eliminating tachyarrhythmia, there is a danger of applying an electrical pulse in the most vulnerable phase of cardiac activity (the period of repolarization of the ventricles of the heart on the ECG corresponds to the apex of the P wave), which can cause ventricular fibrillation (VF). To prevent VF in the treatment of tachyarrhythmia, a cardioverter is used.
Recommendations on the form and energy of the electrical shock for defibrillation are set out in the ERC (2005).
High technologies in the treatment of cardiac arrhythmias
Republican Scientific and Practical Center "Cardiology"
D. Goncharik, leading researcher at the laboratory of cardiac arrhythmias, candidate of medical sciences, associate professor
Irregular or fast beating of the heart is called arrhythmia. There are many different types of arrhythmias - from the usually harmless atrial extrasystoles to the truly life-threatening paroxysms of rapid ventricular tachycardia. An episode of acute rapid heartbeat is called paroxysm. Many arrhythmias can respond well to treatment with medications or disappear with rest (vacation), reducing alcohol consumption, caffeine, and quitting smoking.
*****
However, in some patients, arrhythmias occur so frequently that they interfere with normal life or cannot be treated with medications. In such cases, modern cardiology has a wide arsenal of highly effective minimally invasive and surgical treatment methods. “Minimally invasive” means that elimination of arrhythmia is achieved using special catheters that are inserted into the heart through the vessels of the legs, without cutting the chest, and the patient is conscious only under local anesthesia, without experiencing pain.
This procedure is called ablation, a complex, high-tech heart surgery. On average it takes several hours. Such minimally invasive operations are the most effective method of treating heart rhythm disorders, as they allow patients to completely get rid of arrhythmia.
First, several catheters are inserted into the patient through the veins and/or artery of the thigh under local anesthesia - thin wires that make it possible to record an electrocardiogram of the heart directly from the inside. This is necessary to correctly establish the diagnosis and further treatment tactics. The doctor can control the movement of the catheter tip inside the patient's body using a special device. Such intracardiac cardiograms, recorded from several points, make it possible to most accurately diagnose arrhythmia and determine its source.
After the doctor determines the point in the heart that is responsible for the arrhythmia, it can be eliminated using a special ablation catheter. An ablation catheter differs from other catheters inserted into the heart in that its tip can heat up to 45 - 60 C and “cauterize” the source of the arrhythmia.
All ablations have some risks, although they are usually not particularly dangerous. Fortunately, complications occur in only about 1% of patients. The most common types of arrhythmias that can be successfully treated with catheter ablation in a single procedure are atrioventricular nodal and some other atrial tachycardias, atrial flutter and fibrillation, WPW, and some types of ventricular tachycardias. Unfortunately, not all types of arrhythmias can be successfully eliminated using modern treatment methods, but science and technology do not stand still and new technologies are being introduced every year.
*****
One of the most common types of tachycardia (fast heartbeat) in young people is atrioventricular nodal paroxysmal tachycardia. With such an arry inside the atrioventricular node (connection). To prevent repeated paroxysms of tachycardia, prophylactic administration of special medications may be required. However, most patients do not want to take medications for a long time: they stop taking them or take them irregularly, so attacks of arrhythmia recur. Lasting recovery of patients suffering from such tachycardia can be achieved by cauterization (ablation). To do this, it is necessary to cauterize a small area in the atria in the area of the AV junction and thus break the ring along which the arrhythmia “runs.” After this, it completely disappears and the patient feels like a completely healthy person.
Another arrhythmia that often requires calling an ambulance is arrhythmia in patients with Wolff-Parkinson-White syndrome (or WPW syndrome). WPW syndrome is a congenital defect—an additional abnormal conduction pathway (besides the normal atrioventricular junction) through which impulses can also travel from the atria to the ventricles and vice versa, causing severe cardiac arrhythmias. Some of these arrhythmias can be truly life-threatening.
Patients with WPW syndrome often require special medications to prevent heart rhythm disturbances. It should be noted that although medications can usually provide some control of arrhythmia attacks, complete resolution of symptoms cannot be achieved with medications alone. Therefore, many doctors recommend catheter ablation as the best treatment method.
It is often difficult to localize this additional pathway, but modern computer equipment can significantly increase the efficiency of operations.
One of the most common cardiac arrhythmias in middle-aged and elderly people is atrial fibrillation. In atrial fibrillation (AF), the upper chambers (atria) of the heart contract chaotically and uncoordinatedly (fibrillate) at a rate of approximately 400 times per minute. This chaotic heart rhythm has an adverse effect on the heart, which ultimately leads to the formation of heart failure.
In most cases, patients experience palpitations, dizziness, shortness of breath and fatigue. For some, atrial fibrillation is completely asymptomatic. The tricky thing about atrial fibrillation is that it can cause strokes.
A new episode of arrhythmia is called paroxysm. When AF paroxysm persists for a long time, blood clots (thrombi) can form in the atria, which travel through the bloodstream into the arteries and cause their blockage. The area of tissue that does not receive oxygenated blood dies. The most dangerous is the entry of blood clots into the arteries of the brain, which is accompanied by a stroke. To prevent strokes, patients must take blood thinners such as aspirin or warfarin.
Restoring the rhythm in a patient with atrial fibrillation can be achieved with pills or intravenous medications, or with an electrical shock (electrical shock therapy).
It is extremely important not to delay restoring the rhythm, because if paroxysm persists for a long time, this can be difficult. For example, if a patient's paroxysmal AF persists for more than 48 hours, clots may form in the heart. Before restoring the rhythm, the doctor must make sure that the patient does not have thrombi (blood clots) in the cavities of the heart. For this purpose, transesophageal echocardiography (ultrasound of the heart using a probe similar to a gastric tube) is performed or the drug warfarin is prescribed for 3 to 4 weeks immediately before the cardioversion procedure to thin the blood.
Although electrical cardioversion can restore normal heart rhythm in approximately 90% of patients, unfortunately, in a significant proportion of patients, the rhythm is re-disturbed within a year for various reasons. If AF recurs repeatedly, the doctor decides whether it is advisable to restore the rhythm again in a particular situation or whether it makes sense to transfer AF to a permanent (chronic) form.
Some patients cannot maintain rhythm with medication. There are modern surgical and minimally invasive treatment methods for them.
*****
The labyrinth type surgery is performed under general anesthesia while the heart is stopped. The right and left atria are cut with a scalpel and then stitched together. In this way, it is possible to form a normal “path” for the propagation of a normal rhythm from the atria to the ventricles. However, this operation is complex and requires cutting into the chest.
Physicians with experience in treating cardiac arrhythmias are constantly developing new methods to identify the sources of arrhythmia without cutting into the chest (mapping) or cauterizing the sources of atrial fibrillation so that AFib disappears once and for all.
The mapping and cauterization procedure has been in use since the late 1990s, with new variations being introduced every year. During the ablation procedure, doctors use special catheters to eliminate the sources of arrhythmia in the atria, and if there are too many such areas, they “isolate” them from healthy heart tissue by drawing circular ablation lines. This is a rather complex and lengthy procedure, lasting several hours. Sometimes it is carried out in several stages. The advantage of this invasive operation is that it is performed under local anesthesia; the patient is conscious, there is no need to cut the chest.
Currently, the best results are achieved using a special catheter navigation system inside the heart cavity (CARTO system), which allows you to control the catheter that cauterizes arrhythmia inside the heart cavities with an accuracy of 1 mm. This catheter allows you to build a map of arrhythmia.
The procedure is more effective for patients with frequent short paroxysms of AF; the effectiveness against long-standing AF is significantly lower.
The AF ablation procedure is not without risks. About 2 to 3% of patients experience serious complications such as blood leaking into the heart (tamponade), strokes, nerve damage, narrowing of the pulmonary veins, or a hole forming between the atria and esophagus (atrioesophageal fistula). Many of these complications are treatable but require the patient to remain in the clinic for an extended period of time.
Therefore, to decide on the advisability of a procedure, the doctor weighs the potential benefits and possible risks for a particular patient, choosing the optimal solution for the given case at the time.
*****
Atrial flutter is often an arrhythmia related to atrial fibrillation, in which the atria contract at a high rate of up to 200 to 300 beats per minute, and this rapid rhythm is conducted to the ventricles and causes them to contract at a rate of 100 to 150 beats per minute. This leads to rapid disruption of the normal pumping function of the heart. Treatment of atrial flutter with medications is usually ineffective.
The best treatment for atrial flutter is ablation (cauterization), which produces positive results in approximately 90% of patients.
Excessively fast heartbeats that originate from the heart's ventricles are called ventricular tachycardia (VT). This arrhythmia often poses a serious threat to the patient's life, often leads to loss of consciousness and requires the use of special medications, the use of invasive (catheter ablation) or even surgical treatments.
Typically, severe ventricular tachycardia is treated by sewing a special device under the skin - an implantable cardioverter-defibrillator (ICD), which allows you to interrupt severe attacks of arrhythmia using an electrical discharge from the inside.
Some forms of ventricular tachycardia are less life-threatening and occur in people with nearly normal heart function. Although these forms of the disease can be treated with medications, a permanent cure can be achieved with the help of an ablation procedure and save the patient from repeated breakdowns once and for all. Sophisticated computer systems make it possible to create a map of cardiac excitation during such tachycardia, which makes it possible to identify its source.
Often, a paroxysm of ventricular tachycardia develops into an even more severe arrhythmia - ventricular fibrillation (VF), in which the heart contracts uncoordinatedly at such a high speed that it is unable to pump blood, and this is tantamount to cardiac arrest. With ventricular fibrillation, a person always loses consciousness.
There are many causes of VT and VF, but most often it occurs due to disruption of the blood supply to the heart muscle due to narrowing of the coronary arteries or the presence of scars in the heart muscle. The most effective means of stopping repeated paroxysms of ventricular fibrillation (rhythm restoration) are implantable cardioverter defibrillators (ICDs).
An ICD is an implantable device (similar to a pacemaker) that monitors the heart's rhythm. Unlike a pacemaker (which prevents the heart from beating too slowly), an ICD can also detect and interrupt excessively fast heartbeats - ventricular tachycardia, as well as ventricular fibrillation. If a severe arrhythmia occurs, the cardioverter-defibrillator commands the restoration of the normal rhythm (using a series of rapid electrical impulses or an electrical discharge from the inside). Information about each episode can be downloaded using the programmer and can be read from the ICD memory without cutting the skin. The clinic of the Republican Scientific and Practical Center "Cardiology" has sufficient experience in treating such patients.
In general, the lives of patients with ICDs are almost no different from the lives of other people. Although ICDs successfully treat VT and VF but do not prevent them, patients should avoid situations where they might lose consciousness in a life-threatening situation, such as during unaccompanied swimming, etc. If the patient is touched by another person at the time of the shock, You may feel a slight, momentary tingling sensation, but it poses absolutely no danger. Modern ICDs last for four to six years before the generator needs to be replaced.
Electrical system of the heart
The heart has its own electrical (conducting) system, consisting of an electrical impulse generator - the main pacemaker (sinus node) - and conduction pathways (atrioventricular junction, His bundle and its branches) connecting the entire electrical circuit. The main pacemaker (sinus node), located in the right atrium, generates regular electrical impulses at a certain frequency, like a metronome. In response to each impulse, the heart contracts in a strict sequence - first the atria, then normally through a single connection (atrioventricular, in which its short-term delay occurs), the impulse passes to the ventricles, spreading through the system of fibers, causing the ventricles to contract synchronously.
Bradycardia and pacing
At rest, our heart beats at approximately 50 to 90 beats per minute, although athletes and patients taking certain medications, such as beta blockers, may contract slower. Heart rate increases during exercise, and the maximum varies greatly among individuals.
A slow heartbeat (bradycardia) may cause no symptoms or may cause dizziness, blurred vision, shortness of breath, or fatigue. Bradycardia can occur due to problems with the main pacemaker of the heart (sick sinus syndrome) or a delay in the impulse at the atrioventricular junction (heart block).
Patients with high-grade heart block and sick sinus syndrome usually have a pacemaker fitted.
Pacemakers
A pacemaker is an implanted device that monitors a person's heartbeat and prevents the heart from beating too slowly.
It consists of a “pulse generator” (the pacemaker itself) to which one or two wires (electrodes) are attached. Typically, the pacemaker is placed under the skin or in the muscle just below the collarbone. Almost all modern pacemakers work “on demand”, that is, they turn on only when necessary - when the heartbeat is too slow to set the correct rhythm. The rest of the time, the device only monitors the patient’s own heart rhythm without interfering with its work.
There are many different types of pacemakers available today. Belarusian clinics have all the necessary types. There are physiological pacemakers: they can recognize when the patient is sleeping or, conversely, doing hard work. In response to exercise (fast walking or running), the stimulator increases the heart rate, and at night, on the contrary, it works even slower than during the day at rest.
The service life of modern pacemakers under standard conditions is approximately 7 - 10 years, but can be much longer for a particular patient. The expiration date of the pacemaker battery can be easily predicted during the next scheduled check of the pacemaker.
The pacemaker imposes almost no restrictions on the patient's daily life. Household appliances and mobile phones do not interfere with the operation of the device, although you should not store a mobile phone in a pocket near a pacemaker.
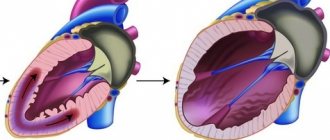
Heart failure
With severe damage to the heart by various diseases, its pumping function gradually decreases. When the pumping function is significantly reduced, the heart is unable to pump the required amount of blood, which is called heart failure.
Most cases of heart failure are caused by the fact that the main pumping chamber of the heart (the left ventricle) cannot contract with sufficient force, but usually the right and left ventricles continue to contract synchronously (almost simultaneously).
Resynchronizing pacemaker
As heart failure increases, the right and left ventricles begin to contract at the same time - the contraction of the left ventricle or part of it is greatly delayed in relation to the right ventricle. Asynchronous contraction further reduces the efficiency of the heart's pumping function. To treat such patients, special stimulants are used. The goal of cardiac resynchronization therapy (CRT) is to stimulate the ventricles so that they contract simultaneously, thereby improving the pumping function of the heart.
In general, the implantation procedure is similar to the procedure for implanting a conventional pacemaker. The only difference is that an additional electrode is inserted to set the correct rhythm to the left ventricle and synchronize the work of the right and left ventricles.
Currently, implantation of pacemakers, including physiological ones, is performed in all regional centers of Belarus. Implantation of more complex devices - resynchronizing pacemakers and cardioverter-defibrillators - is carried out in the republic.
It is important!
Attacks of dizziness and loss of consciousness
Approximately 30 - 50% of people experience fainting or blackout at some point in their lives. Fainting occurs for a variety of reasons, but the immediate common cause is usually a sudden drop in blood pressure, which in turn leads to a short-term reduction in blood flow and oxygen delivery to the brain.
Usually, but not always, a person immediately before losing consciousness feels lightheaded or dizzy, and also complains of darkening of the eyes and ringing in the ears. In addition, nausea, vomiting, sweating, and rapid or slow heartbeat may occur.
Fainting among people of all ages is so common that many do not immediately perceive it as a serious threat to life and may seek professional help from a doctor only after a series of fainting spells, which is a mistake.
The most common type of fainting is due to improper reflex interaction between the cardiovascular and nervous systems, as a result of which the cardiovascular system selects a heart rate and degree of relaxation of the body’s blood vessels that is inadequate to the current situation. In addition to the so-called functional, or “reflex” forms of fainting, patients may also lose consciousness due to organic heart diseases: excessively fast or slow heartbeat, dysfunction of the heart muscle or heart valves, as well as diseases of the nervous system and overdose of drugs that lower blood pressure. Differential diagnosis usually requires an electrocardiogram, as well as an ultrasound scan of the heart or “echocardiogram”, etc.
Doctors may recommend that patients who complain of recurrent “reflex” fainting avoid certain situations that lead to fainting (for example, standing up on a crowded train in hot weather), wear medicated compression stockings, prescribe certain medications, and in some cases, get a pacemaker. if such fainting is accompanied by an excessive slowing of the heart rate.
To diagnose disease of the heart muscle and/or heart valves, certain non-invasive tests are available, such as 24-hour continuous recording of heart rate and rhythm using an ECG (Holter ECG monitoring). In some cases, invasive tests may be required, such as coronary angiography (cardiac catheterization) and/or specialized tests of the heart's electrical system, known as an electrophysiological study, or EPS.
In patients suffering from organic heart muscle disease, fainting often occurs due to an excessively fast heartbeat. In such a situation, the heart simply does not have time to emit the amount of blood necessary to ensure normal functioning of the brain, and the doctor may raise the question of a special heart operation to eliminate or cauterize the source of such arrhythmia. In some cases, it may be decided to implant a special device under the skin, similar to a pacemaker, which will restore excessively fast heartbeats using an electrical current discharge from the inside (ICD).
The main thing is that if fainting occurs, you should not wait for it to recur many times (since the second or third may already be the last), but quickly seek help from a specialist.
Indications for electropulse therapy
At the prehospital stage, indications for EIT include cardiopulmonary resuscitation (CPR), unstable hemodynamics, increasing symptoms of acute left ventricular failure, syncope, severe anginal attack with various types of supraventricular and ventricular tachyarrhythmias (atrial flutter or fibrillation, paroxysmal supraventricular tachycardia, ventricular tachycardia) . In emergency situations, the main indication for EIT is the picture of unstable hemodynamics or CPR.
Effect of physiotherapy
Physiotherapeutic procedures have a normalizing effect on metabolism, redox processes, regulation of internal organs, lymph and blood circulation. In addition, they mobilize the body's defenses.
Physiotherapy is part of the comprehensive treatment of diseases. As a rule, its methods are used at the stage of remission, but can also be used in the acute stage. The main advantage of this direction is the absence of exposure to drugs and chemicals. Thus, the high effectiveness of physiotherapy is combined with the safety of its use.
Success of EIT
The effectiveness of EIT largely depends on the transthoracic impedance (transthoracic resistance). Typically, 10–20% of the discharge energy passes through the heart; an increase in transthoracic impedance leads to a decrease in the current reaching the myocardium, which impairs the effectiveness of EIT. Transthoracic resistance is influenced by chest size and hair cover; size and location of the electrodes, the force of their pressing to the chest; conductive material between the electrodes and the patient’s skin; number of shocks applied; previous surgical interventions on the chest by the patient and a number of other factors. Modern cardioverters have the option of automatic compensation of transthoracic impedance, which allows a discharge close to the optimal one to be passed through the heart.
You should lubricate the defibrillator electrodes with a special conductive gel or use special disposable electrodes, this will reduce the resistance between the electrodes and the patient's skin.
The electrodes must be pressed tightly against the patient’s body with a force of 10 kg, since even a small layer of air between them and the skin is a good insulator, and this will lead to burns.
The discharge must be applied during the exhalation phase; the lungs filled with air increase the resistance of the chest tissues.
EIT in “wet” patients is ineffective, since water on the chest dissipates the charge over the surface and the current discharge will spread in the superficial tissues and, therefore, will not reach the myocardium.
Indications for using pulsed current
In the treatment of various types of pathologies, doctors use pulsed current. The impact is carried out in a rhythm specified by a special device, which corresponds to the rhythm of the functioning of the internal system or a specific organ. The pulse frequency may also change.
Pulsed currents in physiotherapy are used to treat the following diseases and pathological manifestations:
- Lesions of the neuromuscular system;
- Diabetes;
- Painful sensations of various origins;
- Obesity;
- Hyperthyroidism;
- Pathologies in the endocrine system;
- Impaired intestinal motility;
- Diseases of the genitourinary system and pelvic organs;
- Skin problems of a cosmetic nature.
Indications for the use of pulsed current may include injuries and diseases of soft tissues: bruises, myositis, sprained muscles and ligaments. This technique is used for damage to the spine and joints, as well as peripheral nerves as a result of disease or injury. The effect of current helps to cope with rhinitis, otitis, sinusitis, remove stones from the ureter, and cure lymphatic edema of the lower extremities.
In dentistry, fluctuating currents are used to treat neuralgia of the glossopharyngeal, trigeminal and other nerves, alveolitis, periodontal disease, arthritis of the temporomandibular joint, inflammatory and purulent processes in the submandibular and maxillofacial areas, including after surgery.
Rational implementation of electropulse therapy
— Before performing EIT, all patients with preserved consciousness must be provided with complete pain relief. Inhalations are carried out with 100% humidified oxygen. As a premedication, 0.1 mg of fentanyl is prescribed, and for elderly or weakened patients, 10–20 mg of promedol.
— Medicinal sleep is carried out with the help of sibazon (Seduxen, Relanium), 5 mg of which is administered intravenously in a slow stream, and then 2 mg is added every 1–2 minutes to medicinal sleep. It is advisable to use intravenous anesthesia with propofol 2–2.5 mg/kg. In exceptional cases, in the absence of these drugs, the use of ketamine (0.5–1 mg/kg) is acceptable.
— Before and after EIT, an ECG is recorded in leads that are informative for rhythm analysis (II, V1, according to Lian).
— The required discharge energy to stop the rhythm disturbance is selected depending on the type of arrhythmia: for supraventricular tachycardia and atrial flutter - 50 J, for atrial fibrillation - 75 J, for ventricular tachycardia - 100 J, for the diagnosis of polymorphic ventricular tachycardia or ventricular fibrillation - 200 J .
— If EIT is ineffective, repeat after administration of an antiarrhythmic drug indicated for this arrhythmia.
— After EIT, the heart rhythm is assessed. If the arrhythmia continues, a second shock is given at a higher energy level; if ventricular fibrillation is detected, then defibrillation is performed; if sinus rhythm is recorded, then an ECG is recorded and the patient is hospitalized in a hospital.
Indications for hospitalization
All patients who experienced clinical death in the prehospital stage should be urgently hospitalized after hemodynamic stabilization. Hospitalization should be carried out with reliable venous access, with the obligatory possibility of performing EIT during transportation. Patients who have experienced clinical death are transferred “hand to hand” to the resuscitator on duty.
Safety precautions
Persons who have studied the safety rules when working with electronic medical devices are allowed to work with a defibrillator-cardioverter. Remember, a defibrillator is a device of increased, and sometimes fatal, danger! During EIT, it is important not only to help the patient, but also to protect yourself and others. The discharge of the released electrical energy can cause fatal rhythm disturbances in the rescuer or in the person who inadvertently touched the patient.
Necessary:
- remove all strangers (neighbors, relatives, etc.) from the premises;
- wipe the patient’s chest dry;
— remove oxygen from the defibrillation zone.
Prohibited:
— Hold both electrodes of the device in one hand!
— Charge the defibrillator if the electrodes are not placed on the patient’s chest!
— Direct or indirect contact with the patient during EIT!
How to use a defibrillator
1. Turn on the defibrillator.
2. Apply a sufficient amount of conductive gel to the electrodes. If there is not enough gel under the electrodes, burns will occur.
3. Select the required energy level.
4. Install electrodes: one - under the right clavicle marked Sternum, the second - above the area of absolute cardiac dullness marked Apex; with force (10 kg) press the electrodes to the patient’s chest.
5. Give the command “Get energy!”
6. Avoid touching the patient while the shock is being applied.
7. Give a loud command “Discharge!” Perform a discharge by simultaneously pressing both trigger buttons on the electrodes.
8. Check the result of the EIT. Register an ECG.
9. If necessary, resolve the issue of repeated discharge.
Complications of cardioversion include: ventricular fibrillation; aspiration of gastric contents; laryngospasm; hypoventilation; skin burns; electric shock to medical personnel.
Selecting a device for EIT
A wide range and price differences make choosing a device for EIT a difficult task. First of all, you need to decide who will use this device: a paramedic, an emergency rescue worker or a doctor. An AED is a necessary tool for performing high-quality CPR, which does not require extensive personnel training. The price is determined by the quality of electronic components and batteries. Professional cardioverter defibrillators are multifunctional devices that are equipped with an ECG monitor, a built-in thermal printer, an external pacemaker module, and a pulse oximeter for determining SpO2 saturation.
It is necessary to clarify the availability of children's electrodes. Remember that modern devices for EIT generate a biphasic pulse shape, and monophasic defibrillators have not been produced since 2005.
There are no contraindications to the use of emergency cardioversion in a critically ill patient.
Contraindications and effects
It is important to remember that there are certain contraindications for the use of physiotherapy methods using pulsed currents:
- Tumors of various etiologies;
- Individual intolerance to exposure;
- Pregnancy (second trimester);
- Hemarthrosis in the acute stage;
- Kidney and cholelithiasis;
- Spastic state of muscles;
- Dislocations, bone fractures;
- Bleeding.
Current pulses have an exciting, stimulating and irritating effect on the human body. Passing through the tissues of the body, the current causes increased functions of cell membranes and tissue tension. Cells are activated, their vital activity improves, the functioning of joints, blood vessels and nerve fibers is restored. This helps speed up the treatment of many diseases, as well as avoid all sorts of complications.
In general, as a result of exposure to pulsed currents, the following occurs:
- Reducing congestion in the pelvis;
- Metabolism improves, the body's defenses increase;
- The synthesis of organ secretion is activated;
- The permeability of cell membranes increases.
Physiotherapeutic procedures using pulsed current activate blood flow, so the drugs used penetrate the tissues faster, and the effectiveness of treatment increases.