One of the most common diseases is spinal osteochondrosis, which affects every second person in the world, regardless of body type, social status and other characteristics. Speaking about the symptoms of this disease, we can note unpleasant sensations in different areas of the back in the form of pain, heaviness and discomfort. The reason for this is dystrophic changes in the intervertebral discs and joints, due to which destructive processes develop, swelling appears and the surrounding tissues become inflamed, which leads to pain.
The most important “highlight” of osteochondrosis is that during destructive processes, nerve endings and fibers in the sympathetic nervous system are damaged, impulses moving through the blood vessels weaken, and therefore spasms occur in the vascular system and blood supply is disrupted. Taken together, this slows down metabolism, worsens the quality of internal organs, and without competent treatment can lead to irreparable consequences. Thus, with such an insidious disease as osteochondrosis, it is important to use vasodilating drugs that are included in the prescribed set of medications.
When monitoring the development of osteochondrosis, one can often notice that the reaction to irritation of pain receptors is vasospasm, which complicates the patient’s situation. Also, such a reaction can occur when blood vessels are compressed by the vertebral processes. For the same reason, there is an increase in inflammatory tissue edema and progression of ischemic disease. As a result, the degree of damage to cartilage and bones worsens. This is why medications that dilate vascular walls are so important for those who have been diagnosed with osteochondrosis.
Vasodilators for osteochondrosis of the neck
In the article we will understand how vasodilators work for osteochondrosis of the neck, what their types are and how to take them correctly.
The main causes of pathology and stages of its development
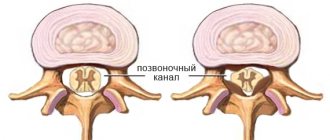
Near the spine, blood vessels, rich in oxygen and nutrients, pass from the heart to the brain. The lateral processes of the vertebrae form a canal through which the vertebral arteries pass, the function of which is to supply blood to the occipital, temporal lobes and inner ear. These areas of the brain are responsible for the perception and processing of visual and sound information, as well as for the analysis of taste and smell. The center of balance is in the inner ear.
Note! A pathological change in the vertebrae can be called a situation when they slightly change their position, therefore, the channels narrow, which leads to disruption of blood flow and a sense of balance. However, osteophytes, the same bone growths, irritate nerve endings and blood vessels and provoke their spasms. This is the essence of osteochondrosis.
There are three stages of pathological changes in blood circulation in osteochondrosis of the cervical spine.
- At the first (initial) stage, the patient experiences dizziness, headache spasms, ringing and noise in the ears, problems sleeping, decreased productivity and focusing on anything.
- In the second stage (subcompensation), the patient is characterized by forgetfulness, lethargy, problems with controlling his actions and speech, and his mental and physical activity is noticeably reduced.
- During the third stage (decompensation), the patient’s central nervous system experiences irreversible changes that make the person conditionally incapacitated, that is, from that moment on, he is unable to independently care for himself and his life.
There are several stages of development of cervical osteochondrosis
Eating disorders and the development of ischemic changes can provoke the occurrence of symptoms that are typical for the symptoms of osteochondrosis of the neck. A person begins to feel pain in various parts of the head, tinnitus, and also complain of problems with vision and hearing. There is the most severe manifestation of this disease, the symptoms of which are similar to those of ischemic stroke.
If negative influencing factors are periodically repeated, then even many years of remission will not be able to protect against the return of the diagnosis.
The most common reasons will be presented below, but this does not mean that there are others. Most residents of large cities are at risk of developing this disease or are already taking special medications for cervical osteochondrosis.
- Overeating and, as a consequence, excess weight, since there is no disease that would not be complicated by the presence of excess fat.
- Problems with posture.
- Constant and long-term work at the computer.
- A sedentary or lying lifestyle is one of the main factors. If a person does not move enough, then his muscles weaken due to “uselessness”. They usually take on most of the load on the spine. But in a weakened state of the muscles, the spine will not be able to cope with heavy loads for long.
In order to prevent and prevent further development of the disease, it is customary to prescribe treatment with vasodilating drugs.
Treatment and hospitalization of pregnant women with hypertension
In order to confirm the diagnosis and select adequate treatment, pregnant women with hypertension syndrome must be hospitalized three times. Antihypertensive drugs during pregnancy are prescribed strictly by the attending physician, who takes into account the duration of pregnancy and possible complications of intrauterine development of the fetus.
- the first hospitalization is carried out in the early stages (up to 12 weeks) - for the purpose of diagnosing hypertension;
- a second hospitalization is planned in the period from 26 to 30 weeks - in order to change therapy;
- The third hospitalization is prescribed a couple of weeks before the birth - to prepare for it.
When gestosis develops against the background of arterial hypertension, the woman requires immediate hospitalization, regardless of how far along the pregnancy she is at that moment.
Arterial hypertension in pregnant women requires constant drug support. Women are prescribed medications, and not only antihypertensives. During pregnancy complicated by high blood pressure, it is recommended to take sedatives, calcium antagonists, beta-blockers, alpha-blockers. In addition, symptomatic therapy is carried out.
In addition to drug therapy, a woman is recommended to follow a special regimen and diet throughout pregnancy.
There are a number of recommendations for pregnant women suffering from arterial hypertension:
- Observing the correct sleep and rest schedule helps to normalize the emotional state - you need to sleep at least 9 hours a day;
- you need to exclude any physical activity;
- A pregnant woman with arterial hypertension syndrome needs to constantly measure her blood pressure.
The nutrition of a pregnant woman, even despite toxicosis, should be complete and nutritious, with a sufficient amount of vitamins, microelements, proteins and antioxidants. It is recommended to include seafood and other foods containing polyunsaturated acids in your diet.
Mechanism of action
Medications specializing in vasodilation and used in the treatment of neck osteochondrosis are divided into 2 general groups.
- Centrally acting drugs that act on the vasomotor center, which, in turn, is located deep inside the brain.
- Peripheral-acting drugs, which are divided into a couple of subgroups:
- drugs that are used to weaken the pain nerve impulse. They belong to the group of neutropic principles of action: they block the impulse, thereby stopping its harmful effect on smooth vascular muscles and preventing spasms;
- drugs that are used to directly or indirectly influence the vascular muscles, thereby helping to increase the lumen of the vessel. The need for this therapy is that it helps to cope with spasms of the smooth muscle walls that regulate the lumen of blood vessels. The lumen of the blood vessels should not narrow, as this makes it difficult to nourish the tissues.
You only need to contact a specialist to select the right medicine - based on the tests, he will prescribe the right drug
Only a doctor who specializes in this is able to correctly draw up a treatment plan and select a set of medications that will help cope with this pathology. It is important to note that taking these medications cannot be long-term. When the natural course of transmission of nerve signals to the blood vessels is normalized, their reception can be completed. If you follow the doctor’s treatment plan, you can avoid unwanted severe consequences and complications for your body and health when treating cervical osteochondrosis with various drugs.
Classification of peripheral vasodilator drugs
Peripheral vasodilator drugs are classified according to their chemical structure and origin into:
- 2-amino-1-phenylethanol derivatives: isoxsuprine;
- nicotinic acid preparations: nicotinic acid;
- purine derivatives: xanthinol nicotinate, pentoxifylline;
- ergot alkaloids: nicergoline;
- Vinca alkaloids: vincamine;
- others: naftidofuryl, bendazole, bencyclane.
In addition, magnesium sulfate, hydralazine, antihypertensive drugs - calcium antagonists (amlodipine, nifedipine, felodipine, isradipine, nitrendipine), nitric oxide donors (sodium nitroprusside), potassium channel activators (minoxidil, diazoxide) have a peripheral vasodilating effect.
There are also combination preparations of the peripheral vasodilator bendazole with the myotropic antispasmodic papaverine.
About precaution
Do not overuse vasodilators.
Note! You cannot take all drugs of this effect at once. Making a treatment plan on your own can be very risky and dangerous. It is the treating specialist, and not someone else, who must analyze the symptoms, make a diagnosis, and then prescribe the necessary medications.
Every doctor has his own opinion about vasodilator drugs. This may be due to the fact that any small error can cause harm to a person, so it is important to know that such medications:
- provoke the removal of calcium from the body, which can have a negative effect on the restoration of bones and intervertebral discs;
- act not only on affected vessels, but also on healthy ones, and this leads to the opposite effect;
- often lead to a “stealing effect”, i.e. they dilate and improve the condition of healthy blood vessels, and not those for which the therapy was carried out.
Vasodilators have some contraindications and side effects
It is clear that vasodilation as the main treatment for ischemia and atherosclerosis cannot be considered a good option.
Like any medicine, drugs for vasodilation have certain contraindications. Some of them are like this.
- Pregnancy and breastfeeding.
- Epilepsy.
- Cardiac disorders.
- Hypertension, that is, constant high blood pressure.
- Kidney failure.
You should also stop taking medications if you have allergies or individual intolerances.
Causes of high blood pressure during pregnancy
Arterial hypertension syndrome in women during pregnancy can be triggered by several factors. Blood pressure in pregnant women increases due to the following changes:
- the location of the heart changes;
- hormonal changes occur - the level of progesterone and estrogen in the blood increases;
- placental blood circulation increases;
- body weight increases;
- the mobility of the diaphragm is limited.
The development of all hemodynamic changes during pregnancy leads to a complex of problems that trigger arterial hypertension syndrome.
List of special substances for vessels
Vascular medications for osteochondrosis of the cervical spine are prescribed by a doctor. Various drugs are used to normalize blood flow.
Aminophylline (“Eufillin”)
Today, one of the most well-known active ingredients of vasodilator drugs is aminophylline. An example of such a medicine is “Eufillin”. It is usually prescribed as tablets, but there is also a type of medicine for intramuscular and intravenous therapies. It is also widely used with electrophoresis for pathological processes in the spine. The main function is based on the fact that it relaxes vascular smooth muscles, so taking this drug helps prevent the development of blood clots and improve circulation. Ultimately, the pain is relieved and blood circulation improves as the muscles relax.
You should only take this medication if it has been prescribed by a specialist, because it has several unpleasant side effects. For example, convulsive syndrome, pain in the heart, blood pressure may suddenly drop, dizziness and some others.
Rules for taking Eufillin
Nicotinic acid, or vitamin PP
Nicotinic acid is used to dilate small vessels, even those in the brain. The use of this drug has a good effect on blood circulation, allows you to achieve a special effect and lowers the cholesterol level in the blood. Basically, the substance is used intramuscularly, but there are cases when it is administered intravenously.
Side effects of vitamin PP include dizziness, slight redness of the face, flushing of the upper body, and a feeling of flushing in the head. There is no need to worry if this medicine has been prescribed, since all the “side effects” listed above are short-lived, which means they will quickly disappear.
Rules for taking nicotinic acid
Lipoic acid, or berlithione
Lipoic acid is used in medicine to improve endoneurial blood flow. Berlition stimulates the strengthening of blood vessels and leads to cell restoration.
In tablets, take 0.05 g after meals 3-4 times a day.
Pentoxifylline
Pentoxifylline helps get rid of spasms in blood vessels and has a good effect on clotting. Also, the use of this drug has the following effect: it stops platelet aggregation and makes the blood less viscous, which leads to increased bleeding in problem areas.
The drug is used both intravenously and in tablets. Bad consequences include hypotension, arrhythmia, heart pain, and headaches.
Features of treatment with peripheral vasodilator drugs
Due to the high risk of shock and collapse - a sharp drop in blood pressure with loss of consciousness - peripheral vasodilator drugs are prescribed with caution to people with hypotension (low blood pressure).
Peripheral vasodilator drugs, lowering blood pressure, with a sharp change in the horizontal position of the body to a vertical one, can lead to an outflow of blood from the brain, which is manifested by dizziness and even loss of consciousness. This condition is called orthostatic hypotension. To prevent the development of such an effect after taking peripheral vasodilator drugs, the patient should lie down or sit for about half an hour, without getting up suddenly.
Since peripheral vasodilator drugs thin the blood, having an antiplatelet effect, their use is contraindicated in patients with reduced blood clotting and uncontrolled bleeding.
When using peripheral vasodilator drugs, you should stop drinking alcohol and smoking.
Treatment of neck osteochondrosis with ointments
When treating osteochondrosis, special ointments are often used to alleviate the patient’s illness. Their peculiarity is that they have a very small number of contraindications (possible pressure changes, headaches, nausea, dizziness and drowsiness), act gently and do not cause discomfort. Abiflor ointment is very effective and popular among people, which helps to expand and strengthen vascular walls, as well as regenerate their patency and reduce pain. The composition includes the following components: perfume oils, emulsifiers, fir water extract, vitamin E and some others.
At the same time, there are other ointments with the effect of dilating the walls of blood vessels, which have a warming effect:
- "Nicoflex";
- "Menovazan";
- "Gevkamen" and others.
The use of vasodilating ointments gives no less effective results
The main thing to remember is that before taking vascular medications, be they tablets, ointments, or drugs for intravenous or intramuscular administration, you must consult with a qualified medical specialist in the field. You can see different reviews about the above medications, and thanks to them and a specialist, it is possible to choose the very “panacea” that will free a person from unpleasant symptoms.
Principles for choosing antihypertensive drugs
A.A.
UPNITSKY ,
Russian National Research Medical University named after. N.I. Pirogova, Moscow Arterial hypertension (AH) and its complications are widespread in the population today and carry a high risk of disability and death among the population, mainly of working age (cerebral stroke, myocardial infarction, chronic heart failure, end-stage renal failure, cardiac arrhythmias, etc.) .
At the same time, the effectiveness of blood pressure control in patients with hypertension remains unacceptably low for various reasons. This article presents an attempt to streamline the prescription of antihypertensive drugs by applying a specific algorithm for their prescription, including adequate monitoring of the ongoing antihypertensive therapy. The article uses the latest ESC/ESH-2013 recommendations, as well as the American JNC-8 of December 2013 for the treatment of hypertension (JAMA-2014, December, online). The work provides an original algorithm for choosing antihypertensive therapy, including methods and timing for assessing both the effectiveness and safety of antihypertensive therapy. At the beginning of the article, it is appropriate to provide a classification of arterial hypertension according to blood pressure level ( Table 1
).
Table 1. Classification of arterial hypertension by blood pressure level
| Category | Systolic blood pressure, mm Hg. Art. | Diastolic blood pressure, mm Hg. Art. |
| Optimal | <120 | <80 |
| Normal | <130 | <85 |
| High normal | 130-139 | 85-89 |
| Hypertension 1st degree | 140-159 | 90-99 |
| Hypertension 2nd degree | 160-179 | 100 -109 |
| Hypertension 3rd degree | ≥180 | ≥110 |
Relationship between blood pressure and damage to the cardiovascular system and kidneys
The relationship between blood pressure and cardiovascular and renal complications and mortality has been studied in a large number of observational studies. Their main results are as follows:
1. Office BP is directly associated with the incidence of stroke, myocardial infarction, sudden death, heart failure and peripheral arterial disease (PAD), as well as end-stage renal disease (ESRD). 2. In individuals over 50 years of age, SBP appears to be a better predictor of clinical events than DBP. In elderly and senile people, pulse pressure (the difference between SBP and DBP) plays a possible additional prognostic role. This is also evidenced by a particularly high cardiovascular risk in patients with elevated SBP and normal or low DBP - isolated systolic hypertension (ISAH). 3. Blood pressure values measured outside the office, such as those obtained during ABPM and home blood pressure monitoring (HBP) are also related to clinical events. 4. The relationship between cardiovascular morbidity and mortality varies depending on the presence of other concomitant cardiovascular risk factors listed below.
Risk stratification criteria for arterial hypertension (recommendations of VNOK-2004)
Risk factors
Basic
- Men > 55 years old.
- Women > 65 years old.
- Smoking.
- Cholesterol > 6.5 mmol/L, or low-density lipoprotein cholesterol >.4.0 mmol/L, or high-density lipoprotein cholesterol < 1.0 mmol/L.
- Family history of early CCP (women <65 years, men <55 years).
- AO (OT ≥ 102 cm for men or ≥ 88 cm for women).
- CRP ≥ 1 mg/dl.
Additional
- NTG.
- Low physical activity.
- Increased fibrinogen.
Target organ damage (stage II hypertension) Left ventricular hypertrophy (ECG, echocardiography, radiography).
Microalbuminuria (30-300 mg/day). Ultrasound signs of thickening of the arterial wall (thickness of the intima-media layer of the carotid artery ≥ 0.9 mm) or atherosclerotic plaques of the great vessels. A slight increase in serum creatinine 115-133 µmol/l for men or 107-124 µmol/l for women. Associated clinical conditions (stage III hypertension)
Cerebrovascular diseases
- Ischemic stroke.
- Hemorrhagic stroke.
- Transient ischemic attack
Heart diseases
- Myocardial infarction.
- Angina pectoris.
- Coronary revascularization.
- Congestive heart failure
Kidney diseases
- Diabetic nephropathy.
- Renal failure (creatininemia > 2.0 mg/dL).
- Proteinuria (>300 mg/day).
Peripheral artery diseases
- Dissecting aortic aneurysm.
- Symptomatic peripheral artery disease
Hypertensive retinopathy
- Hemorrhages or exudates.
- Swelling of the optic nerve nipple.
Thus, to reduce cardiovascular risk and prevent the above-mentioned consequences of hypertension, along with a number of non-drug measures (control of body weight, metabolic profile, smoking control, limiting salt intake, cyclic aerobic exercise of sufficient intensity and duration, a full night’s sleep), it is necessary to achieve target blood pressure levels using primarily antihypertensive drugs.
So, how to choose them correctly? Requirements for the treatment of hypertension [1]:
- Smooth decrease in blood pressure.
- Patient compliance.
- Regression of target organ damage.
- Increasing life expectancy and improving its quality.
- Stable maintenance of blood pressure at the target level.
Target blood pressure is the blood pressure level at which the minimum risk of cardiovascular morbidity and mortality is recorded ( Table 2
).
Table 2. Target blood pressure levels
| Patient group | Target BP |
| General population of patients with hypertension | <140/90 mmHg Art. |
| Hypertension + diabetes, proteinuria <1 g/day | <130/85 mmHg Art. |
| AH + DM, proteinuria > 1 g/day | <125/75 mmHg Art. |
| AH + chronic renal failure | <125/75 mmHg Art. |
| Patients over 60 years of age | <150/90 mmHg Art. * |
| * JNC-8, JAMA, December 2014, online. | |
We propose to select antihypertensive drugs according to a certain scheme - an algorithm consisting of three main fundamental stages. The use of such an algorithm should help the doctor treating such patients to achieve maximum effectiveness and at the same time minimize the risk of side effects of the pharmacotherapy.
The first stage of choosing an antihypertensive drug is pathogenetic ( Fig. 1
). In a patient with hypertension, we suggest two steps at this stage. The first is compiling a list of drugs that effectively affect the pathogenesis of the symptom - high blood pressure. In other words, the doctor should try in each specific case to determine which hemodynamic factor “warms up”, so to speak, increased blood pressure [1-3].
Figure 1. Pathogenetic stage of selection of antihypertensive drugs
Selection of drugs depending on the cause of increased pressure
| Increased cardiac output | Increased peripheral resistance | Increased circulating blood volume |
|
|
|
Selection of drugs in accordance with their organoprotective properties
| Cardioprotective drugs | Cerebroprotective drugs | Nephroprotective drugs |
|
|
|
This factor may be, for example, increased cardiac output (in the “hyperkinetic” version of hypertension, as in hyperthyroidism, or in the early stages of hypertension in young and sometimes middle-aged people).
In patients with “experienced” hypertension, cardiac output is extremely rarely increased, and increased peripheral resistance comes to the fore in maintaining elevated blood pressure. First, it is caused by transient increases in peripheral arterial vascular resistance in response to increases in blood pressure (the meaning of this phenomenon is the protection of peripheral organs and tissues from hyperperfusion). Over time, hypertrophy of the middle muscular layer of arterioles—resistance vessels—develops, and increased peripheral resistance is fixed at the organic level. Another component of this “equation” may be an increased circulating blood volume (CBV), the so-called. volume-dependent hypertension. As a rule, these are patients with obesity (there are many small vessels in the adipose tissue with additional blood volume), with swelling or pastiness of the legs, if they are not caused by chronic venous insufficiency.
According to the assessment of the hemodynamic variant of hypertension by the attending physician, in the first case, the list of effective drugs will include those that reduce cardiac output (beta-blockers, centrally acting drugs, “rhythm-slowing” calcium antagonists) [1, 4]
In the second, this will be a list of drugs that reduce total peripheral vascular resistance (TPVR): ACE inhibitors, angiotensin II receptor antagonists of the 1st subtype (sartans), calcium antagonists (all), centrally acting drugs (I1 receptor agonists - rilmenidine, moxonidine etc.), sympatholytics (dopegit), beta-blockers with a vasodilating effect (carvedilol, nebivolol, etc.), long-acting alpha-blockers (doxazosin, terazosin, etc.), diuretics (with regular use for at least 2-3 weeks .). The latter reduce OPSS due to the removal of sodium from the vascular wall, which leads to a decrease in OPSS both by reducing its edema and by reducing its response to vasoconstrictor stimuli.
In the third case, preference will be given to diuretics. It should be remembered that mixed hemodynamic options are possible, and in such cases, drugs are combined [5].
But, given the importance of target organ damage in hypertension and organ protection, the doctor must identify in each patient with hypertension his version of target organ damage: this could be the brain and its vessels (“cerebral” version according to the old classification), the heart - in the form changes in the left sections (hypertrophy or dilatation of the left atrium and ventricle), as well as damage to the coronary arteries with an obvious or latent form of myocardial ischemia (cardiac form of hypertension); kidneys (microalbuminuria); hyperazotemia indicates advanced stages of kidney damage in hypertension. It is also possible to detect changes in the vessels of the retina or arteries of the lower extremities (also often asymptomatic, but detected during a targeted examination).
In accordance with the identified “target” organ (“targets”), the doctor compiles, still at the same first stage, a list of antihypertensive drugs that have appropriate organoprotective properties for hypertension (cardio-, cerebro- or nephroprotective).
ACE inhibitors, angiotensin II receptor antagonists of the 1st subtype (sartans), beta-blockers, calcium antagonists (to varying degrees), indapamide have proven cardioprotective properties; centrally acting antihypertensive drugs have moderate effects [1, 6–8].
Calcium antagonists (nimodipine) have cerebroprotective properties in hypertension, although this issue is not yet completely clear.
Nephroprotective properties in hypertension have been proven for ACE inhibitors, especially with a combination of hypertension and diabetes mellitus, angiotensin II receptor antagonists of the 1st subtype (sartans), as well as calcium antagonists.
Having now compared both lists (“hemodynamic” and “organoprotective”), the doctor should leave in the final list of the 1st stage only those drugs that are present in both lists simultaneously. This will be the final list of the 1st stage - a list of drugs that are effective in this particular case, but not yet taking into account their safety for the patient.
This aspect of drug selection is the subject of the second stage, in which the list of antihypertensive drugs that are effective for a given patient in a given situation, compiled at the first stage, should be considered from a different angle, namely: whether all effective drugs from this list will be safe for this patient. To solve this problem, we must return to the anamnesis (indications in the anamnesis of intolerance or unsatisfactory tolerability of certain drugs, including those related to those prescribed). Next, you should review the list of concomitant diseases in this patient - contraindications to taking certain medications may also be identified here. For example, if you have a history of bronchial asthma, drugs from the group of beta-blockers are contraindicated. These same drugs, with the exception of beta-blockers, which have vasodilating properties, are contraindicated in patients with stenosing atherosclerosis of the arteries of the lower extremities, with intermittent claudication. Beta-blockers are also contraindicated in cases of atrioventricular block above degree I/bradycardia less than 50 per minute. Alpha-blockers are contraindicated in case of concomitant angina pectoris, as they can cause an increase in anginal attacks. Sympatholytics, which have recently been used extremely rarely, are contraindicated in persons with peptic ulcer disease. Calcium antagonists are contraindicated in patients with gastroesophageal reflux disease (GERD) because they cause relaxation of the lower esophageal sphincter and thereby may worsen the symptoms of GERD. Calcium antagonists, primarily verapamil, can significantly aggravate constipation and are therefore contraindicated in this category of patients. Diuretics can increase the level of uric acid in the blood, and therefore hyperuricemia and gout are contraindications for them. For carbohydrate metabolism disorders, the only safe diuretic is indapamide. A number of antihypertensive drugs can have a negative effect on the course and outcome of pregnancy. Therefore, a limited range of antihypertensive drugs is prescribed for it [1, 6, 7]:
- Methyldopa.
- Labetolol.
- Pindolol.
- Oxprenolol.
- Nifedipine SR.
- Hydralazine.
- For kidney disease - diuretics.
Thus, after the 2nd stage of selection, only drugs that are effective and at the same time safe for a patient with hypertension will remain on the list.
The third and final stage of choosing an antihypertensive drug is the stage of individualization of pharmacotherapy.
The first step is to decide what pharmacotherapy is indicated for this patient (mono-or combined). When resolving this issue, one should proceed from the degree of increase in blood pressure and the duration of hypertension. With long-term hypertension, with high numbers, you should start with a combination of antihypertensive drugs from the very beginning. At the same time, rational and irrational combinations of antihypertensive drugs are distinguished ( Fig. 2
).
possible combinations (only dihydropyridine calcium antagonists can be normally combined with β-blockers) Red continuous line: not recommended combination |
In cases of mild hypertension, not corrected by non-drug treatment methods (see above), and moderate hypertension, monotherapy is possible in some cases.
However, in the treatment of hypertension there is a rule: combinations of antihypertensive drugs with different mechanisms of action are preferable to high-dose monotherapy. Firstly, in combination, the effect is achieved by influencing different parts of the pathogenesis of hypertension, and secondly, with the right combination, the side effects of the drugs are mutually neutralized. For example, “escape” of the hypotensive effect due to the activation of counter-regulatory mechanisms manifests itself when taking arteriolar vasodilators by increasing cardiac output; when taking all antihypertensive drugs, except diuretics, due to sodium and water retention in the body; when taking diuretics – due to the activation of the body’s neurohormonal systems, in particular the renin-angiotensin-aldosterone system [1, 5, 6]. The choice of method of administration of an antihypertensive drug is determined by the clinical situation: in case of an acute rise in blood pressure, drugs are administered parenterally (intravenously or intramuscularly), as well as sublingually (Capoten, Prazosin, Corinfar, etc.) ( Table 3
). It should be noted that these drugs have a short onset of effect and at the same time a short half-life. That is, they should be used specifically in acute situations, and are much less suitable for long-term use. The fact is that when taking short-acting drugs, there are constant fluctuations in their concentration in the blood, and after them, fluctuations in their hypotensive effect, which is accompanied by significant variability in blood pressure during the day. The latter is an unfavorable factor; in particular, the risk of hypertension complications increases. In addition, when taking the last dose of such a drug, even before bedtime, it still does not prevent the morning rise in blood pressure.
Table 3. Medicines for self-relief of blood pressure rise (according to M.V. Leonova, 2012, as amended)
| Drug (INN*) | Method of administration | Start of action | Maximum effect | Duration of action | Doses |
| Captopril | Inside, under the tongue | 15 minutes | 1-2 hours | 4-6 hours | 12.5-50 mg |
| Clonidine | Inside, under the tongue | 30 min | 1-2 hours | 8-12 h | 0.075-0.15 mg |
| Nifedipine | Orally or chew | 15 min 5 min | 30 min 15 min | 4-6 hours 4 hours | 10-20 mg |
| Prazosin | Inside, under the tongue | 15-30 min | 1-2 hours | 8 hours | 1-2 mg |
| Nitroglycerine | Under the tongue, lingual spray | 1 min | 15 minutes | 30 min - 1 hour | 0.3-0.5 mg |
| * International nonproprietary name. | |||||
Here it should be recalled that in case of exacerbation of hypertension, one should try to identify its cause.
In this case, we may encounter the patient’s abuse of table salt, alcohol, taking non-steroidal anti-inflammatory drugs to relieve pain (arthrosis, arthritis, sciatica, headaches, etc.), constant lack of sleep for some reason, non-compliance with the recommended pharmacotherapy (skipping medications). Therefore, long-acting drugs with a long half-life are indicated for continuous maintenance antihypertensive therapy. Another important advantage of drugs with a long duration of action is the possibility of taking them once or twice a day, which helps to increase patient adherence to treatment (according to some data, in the treatment of hypertension during the year it is about 40%). Obviously, this does not mean adequate blood pressure control.
In this regard, the antagonist of angiotensin II receptor subtype 1, candesartan, is of interest; it has the longest half-life of all drugs in this group (more than 24 hours), which makes it possible to achieve blood pressure control also in the morning. In addition, candesartan has advantages over other drugs in cases of combination of hypertension with chronic heart failure, type 2 diabetes mellitus, diabetic nephropathy, proteinuria, and left ventricular myocardial hypertrophy.
To date, the results of 14 placebo-controlled studies with candesartan in 3,377 patients with hypertension are available. Daily doses of the drug ranged from 2 to 32 mg with a follow-up period of 4 to 12 weeks. Baseline blood pressure (diastolic) (DBP) ranged from 95 to 114 mmHg. Art. Within this dosage range, 2,350 patients received active candesartan therapy and 1,027 patients received placebo. In all studies, a significant hypotensive effect of candesartan was noted, which was dose-dependent, i.e., it was more pronounced the higher the dose of candesartan.
From a safety standpoint, the absence of a “first dose effect” was demonstrated, i.e., when taking the first dose of candesartan, there was no sharp decrease in blood pressure. As with other antihypertensive drugs, the hypotensive effect of candesartan increased during the first two weeks and by the end of this period was already clearly expressed. Similar to other antihypertensive drugs, the maximum effect was observed at the end of the 1st month of therapy. Moreover, the hypotensive effect of candesartan did not depend on the age or gender of patients, as well as on race and ethnicity. Of particular note is the good tolerability of candesartan even at a daily dose of 32 mg.
As for the stability of the hypotensive effect, in studies lasting up to one year there was no evidence of the hypotensive effect of candesartan.
Comparative studies of candesartan and losartan in hypertension were also conducted (CANDLE, CLAIM I and II studies, meta-analysis by Zhenfeng Zh, Huillan Shi, Junya Jia et al.), which demonstrated the advantage of candesartan in terms of the severity of blood pressure reduction and its tolerability by patients.
Thus, candesartan has a long-term pronounced hypotensive effect, which depends on the dose of the drug.
The intervals between doses of antihypertensive drugs, with the exception of diuretics, are 2-3 half-lives of the drug and are indicated in the instructions for it. At the same time, one should keep in mind the possibility of reducing the duration of action of antihypertensive drugs when they are accidentally simultaneously prescribed with drugs that are inducers of hepatic metabolism, accelerating the metabolism of antihypertensive drugs in the liver and their excretion from the body. Inducers of hepatic metabolism include, in particular, phenobarbital, other anticonvulsants, rifampicin, etc. In such cases, the intervals between doses of antihypertensive drugs should be reduced [1, 6].
Duration of treatment. With a certain “experience” of hypertension in the body, a “reconfiguration” (“resetting”) of blood vessels, kidneys, brain, and heart occurs to work at elevated blood pressure. In addition, the body retains mechanisms that support hypertension (except for rare cases of surgical treatment of arterial stenosis, removal of adrenal aldosteroma, pheochromocytoma, thyroidectomy and some others). That is why, after normalization and stabilization of blood pressure, antihypertensive therapy should not be stopped. Another thing is that over time, especially in the warm season, it is permissible to reduce the dose and amount of antihypertensive drugs under the control of blood pressure and well-being, provided that all non-drug methods of lowering blood pressure are followed. Criteria for assessing the effectiveness and safety of antihypertensive therapy
To assess the effectiveness, along with assessing the dynamics of the patient’s well-being, office BP measurements should be used, as well as additional methods: 24-hour BP monitoring - ABPM, home measurement (HBP) by the patient.
When measuring office blood pressure, this should be done repeatedly at intervals of 2 minutes, following certain rules. In addition, to assess the safety of antihypertensive therapy, especially alpha-blockers, diuretics, ACE inhibitors and their combinations, blood pressure should be measured in clinostasis (lying down, after 5 minutes) and in orthostasis (after 2 minutes in an upright position). A pronounced decrease in blood pressure in orthostasis (by 20 mm Hg or more) increases the risk of cardiovascular complications and may adversely affect the patient’s well-being.
Additional methods of blood pressure control (ABPM and DMBP) make it possible to avoid unnecessary and unsafe therapy for the patient in the case of “white coat hypertension”, to identify patients with a predominantly nocturnal rise in blood pressure or with an insufficient or excessive decrease in blood pressure at night. The information obtained is valuable for the correct selection and evaluation of antihypertensive therapy [1, 2, 6–8].
To help the practitioner, we provide a list of some fixed combinations of antihypertensive drugs ( Table 4
).
Table 4. Fixed combinations of antihypertensive drugs
| Angiotensin-converting enzyme inhibitor + calcium antagonist |
| Enalapril 5 mg + felodipine 5 mg Benazepril 10/20 mg + amlodipine 2.5/5 mg Perindopril 5/10 mg + amlodipine 5/10 mg Trandolapril 1/2/4 mg + verapamil SR 180/240 mg Enalapril 10 mg + diltiazem 180 mg Lisinopril 10/20 mg + amlodipine 5/10 mg Ramipril 5 mg + felodipine retard 5 mg |
| Angiotensin II receptor antagonist + calcium antagonist |
| Valsartan 80 mg + amlodipine 5 mg |
| Angiotensin-converting enzyme inhibitor + diuretic |
| Lisinopril 10/20 + hydrochlorothiazide 12.5/25 mg Captopril 25/50 + hydrochlorothiazide 12.5/25 mg Enalapril 20 mg + hydrochlorothiazide 12.5 mg Enalapril 10 mg + hydrochlorothiazide 25 mg Enalapril 10 mg + hydrochlorothiazide 12.5 mg Quinapril + Hydrochlorotiazide 12.5/25 mg Lisinopril 10 mg + hydrochlorotiazide 12.5 mg ramipril 5 mg + hydrochlorotiazide 12.5 mg fosinopril 20 mg + hydrochlorotiazide 12.5 mg moexipril 15 mg + hydrochlorotiazide 25 mg cylized 5 mg + hydrochlorotiazide 12.5 mg Perindopril 2 mg + indapamide 0.625 mg Perindopril 4 mg + indapamide retard 0.5 mg |
| Angiotensin II receptor antagonist + diuretic |
| Losartan 50 mg + hydrochlorothiazide 12.5 mg Valsartan 80 mg + hydrochlorothiazide 25 mg Eprosartan 600 mg + hydrochlorothiazide 12.5 mg Irbesartan 150/300 mg + hydrochlorothiazide 12.5 mg Telmisartan 80 mg + hydrochlorothiazide 12.5 mg Telmisartan 40/8 0 mg + hydrochlorothiazide 12.5 mg Candesartan 8 mg + hydrochlorothiazide 12.5 mg |
| β-blocker + diuretic |
| Pindolol 10 mg + clopamide 5 mg Bisoprolol 2.5 mg + hydrochlorothiazide 12.5 mg Propanolol 40/80 mg + hydrochlorothiazide 12.5 mg Bisoprolol 2.5/5/10 mg + hydrochlorothiazide 6.25 mg Metoprolol 50/100 mg + hydrochlorothiazide 25/50 mg Atenolol 100 mg + chlorthalidone 25 mg Atenolol 50/100 mg + chlorthalidone 12.5/25 mg Calcium antagonist + |
| β-blocker |
| Felodipine retard 5 mg + metoprolol succinate 50 mg Amlodipine 5 mg + atenolol 50 mg |
In conclusion, we urge all doctors involved in the treatment of hypertension in outpatient and inpatient settings to approach the diagnosis and treatment of patients with hypertension thoughtfully, clearly understanding the sequence of actions for diagnosis and selection of antihypertensive therapy, and we wish them good luck on this thorny path.
BIBLIOGRAPHY
1. Recommendations for the treatment of arterial hypertension. ESH/ESC 2013. Russian Journal of Cardiology, 2014, 1: 5-92. 2. VNOK. Prevention, diagnosis and treatment of arterial hypertension. Russian recommendations (fourth revision). M., 2010. 3. Recommendations of VNOK. Diagnosis and treatment of arterial hypertension. M., 2009: 5-34. 4. Bauchner H, Fontanarosa PB, Golub RM. Updated guidelines for management of high blood pressure: Recommendations, review, and responsibility. JAMA, 2013, December 18. 5. James PA, Oparil S, Carter BL et al. 2014 Evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA, 2013, December 18. 6. Peterson ED, Gaziano JM, Greenland P. Recommendations for treating hypertension: What are the right goals and purposes? JAMA, 2013, December 18. 7. Sox HC. Assessing the trustworthiness of the guideline for management of high blood pressure in adults. JAMA, 2013, December 18. 8. Wood S. JNC 8 at Last! Guidelines Ease Up on BP Thresholds, Drug Choices. Medscape, December 18 (https://www.medscape.com/viewarticle/817991).
Prevention of osteochondrosis
Prevention of various diseases always takes place in the life of any person, and osteochondrosis is no exception. To do this, it is enough to try to adhere to a healthy lifestyle, do gymnastics and be in physical shape. Stress and other emotional shocks can give a good start to the development of osteochondrosis, so it is necessary to avoid stressful situations or cope with them without breaking points. Proper nutrition is a truly important part of the prevention and treatment of neck osteochondrosis.