Children's blood tests and vaccinations
A clinical blood test in the Russian Federation is included in the standard examination before vaccination. My opinion is that most often it is completely unnecessary if, for example, the child appears healthy and there are no complaints. Nevertheless, the analysis is carried out and the results are often interpreted completely inadequately.
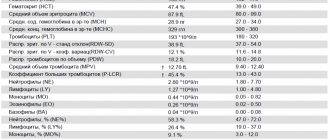
Many laboratories simply forget about the fact that the interpretation of the results of a child’s blood test has its own characteristics. And they simply write analyzes on standard forms, where “norms” are printed in a column next to the analysis results. But children’s indicators cannot be compared with these standards!
About children's hemoglobin standards
How much hassle these forms with “deviations” from the norm cause parents! How many alarming calls and letters fall upon the pediatrician! My colleagues and I are forced every day to dispel the fears of parents who are trying to independently evaluate the results of their children’s tests.
For example, hemoglobin
. In adults, its norm is from 120 to 150 g/l. For children, everything is more complicated. If immediately after birth “normal” hemoglobin is 180–220 g/l, then by 2–3 months of life its level rapidly drops to the lower limit of normal, which starts at 90 g/l. This is the so-called physiological anemia. And since this is the norm, there is no need to treat it.
How to decipher the leukocyte formula?
Leukocyte formula, microscopy of leukocytes, five fractions of leukocytes, differentiation of leukocytes - in doctor’s prescriptions you can find many names for the same thing. Where can I find it and how to decrypt it?
What are leukocytes?
Leukocytes (white blood cells) are a large group of blood cells. Their main purpose is to protect the body from infections. All leukocytes are part of the immune system; they are involved in allergic, autoimmune, and tumor processes. Each type of white blood cell has its own role and is important for the body.
A general blood test without a leukocyte formula speaks only about the total content of leukocytes and does not reveal what type of leukocytes is responsible for the increase (leukocytosis) or decrease (leukopenia) of white blood cells. The leukocyte formula determines five types of leukocytes and is assessed in a comprehensive general blood test. To decipher the leukocyte formula, you need to evaluate the content of each type of leukocyte and their ratio to each other.
The leukocyte formula is calculated by an automatic blood analyzer. Taking the content of all white blood cells as 100%, it gives the percentage (%) of each type of white blood cell. It also automatically measures their content in blood volume (per liter). Sometimes a “hand count” and visual assessment of the blood smear under a microscope is required. For example, when the white blood cell count is altered, there are strange or immature cells, there are signs of anemia or a decrease in platelets in the general blood test. In this case, you can only see the percentage of the leukocyte formula.
Granulocytes - shock forces
The largest part of leukocytes is represented by granulocyte cells. They got their name due to the presence of inclusions (granules). The granules contain immune chemicals. In the leukocyte formula you can see three types of granulocytes: neutrophils, eosinophils, basophils. They differ in the structural features of the core and the coloring of the granules with different dyes. Granulocytes are important in the development of inflammation and immune defense of the body. They are capable of absorbing and digesting proteins and chemicals. All granulocytes mature in the bone marrow, maintaining a supply of mature cells there for 3-4 days. Granulocytes circulate in the blood for no more than 6 hours, moving into the tissues where they perform their function.
Neutrophils make up the largest number of leukocytes circulating in the blood. Every day, 1010 neutrophils enter the bloodstream. Neutrophilia (an increase in the number of neutrophils in the blood) is an indicator of a bacterial infection. The more severe the infection, the more neutrophils come out to fight. Due to their low life expectancy (about 4 days), younger, immature forms of cells (band cells, metamyelocytes, and others) begin to enter the blood. Doctors call this a “leukocyte shift to the left.” When there are very few neutrophils in the blood (neutropenia), the body is not protected from infections.
Eosinophils in the blood make up no more than 5% of the total number of leukocytes. Their concentration fluctuates throughout the day due to the influence of adrenal hormones. In the morning it is maximum. They accumulate in the submucosal layer of the gastrointestinal tract. Eosinophilia (increased eosinophilia in the blood) occurs with parasitic infections, allergic and autoimmune processes.
Basophils make up the smallest number of leukocytes in the blood (less than 1%) and are involved in allergic reactions by releasing histamine. This substance is responsible for bronchospasm, itching, swelling, and redness. Depending on where the basophils get to, there will be manifestations of allergic reactions: an attack of bronchial asthma, skin rash, urticaria, Quincke's edema (swelling of the larynx).
Monocytes are tissue hunters
The second link of leukocytes is monocytes. In the bone marrow, having formed in 5 days, they do not form a reserve. In the blood, monocytes make up about 10% of the mass of leukocytes, quickly disappearing into the tissues. Tissue macrophages, and this is what monocytes will be called, are mainly found in the liver, spleen, and lungs. Their life expectancy is very long (60 days). They are the main hunters of the immune system, because... absorb and process thousands of foreign proteins, turning them into antigens accessible to immune cells.
Monocytosis (an increase in monocytes in the blood) is associated with chronic infections, as well as with infections whose pathogens are hidden in the body’s cells (viruses, chlamydia, mycoplasma).
Lymphocytes are reliable defenders
Antigens processed by monocytes-macrophages and other immune cells attract lymphocytes. Lymphocytes provide acquired immunity by producing antibodies and memory cells to protect against re-infection.
Lymphocytes are formed in the bone marrow and circulate both in the blood and in the lymphatic system. Important organs of cell maturation are the thymus (thymus gland) and lymph nodes. Lymphocytes perform various immune functions, representing the second largest group of leukocytes. There is a special blood test (immunophenotyping) that allows you to identify different types of lymphocytes. This can be important for diseases of the immune system, HIV infection, etc.
In the leukocyte formula, both an increase in lymphocytes (lymphocytosis) - more typical for viral infections - and lymphopenia (a decrease in their number) are important. A lack of lymphocytes reduces the body's defenses and is observed in immunodeficiencies (including HIV infection).
In the Lab4U laboratory you can take the following tests with a 50% discount:
- General blood test with leukocyte formula (automatic counting)
- General blood test with microscopy (manual leukocyte count)
Leukocyte formula (with mandatory microscopy of a blood smear) - counting the total number and different types of leukocytes, as well as studying their morphological features through microscopy of a peripheral blood smear.
Synonyms Russian
Leukoformula.
English synonyms
Leukocyte Differential Count, WBC Count Differential, Diff, Blood Differential, Differential Blood Count, White Blood Cell Differential.
Research method
Flow cytometry.
What biomaterial can be used for research?
Venous, capillary blood.
How to properly prepare for research?
- Eliminate alcohol from your diet for 24 hours before the test.
- Children under 1 year of age should not eat for 30-40 minutes before the test.
- Do not eat for 2-3 hours before the test; you can drink clean still water.
- Avoid physical and emotional stress for 30 minutes before the test.
- Do not smoke for 30 minutes before the test.
General information about the study
Leukocytes are a heterogeneous population of nucleated blood cells that are an essential part of the human immune system and play a role in inflammation, allergies and antitumor defense. There are five types of leukocytes, each of which performs its own specific functions: three types of granulocytes (eosinophils, basophils, neutrophils), monocytes and lymphocytes. The study of the leukocyte formula in a peripheral blood smear is a count of the number of different types of leukocytes and an assessment of their morphological properties. Both venous and capillary blood can be used for research.
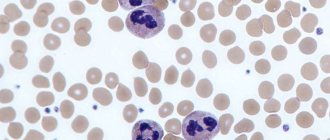
Staining a blood smear with special dyes makes it possible to distinguish cells and intracellular structures; in addition, different types of leukocytes are not equally susceptible to certain dyes and are stained differently, which, together with differences in their morphological properties (shape of the nucleus, size and presence of intracellular granules), makes it possible to differentiate the main types of leukocytes when examining a smear using a microscope. Traditionally, the count is carried out per hundred cells and the resulting numbers are recorded as percentages. Knowing the total number of leukocytes, percentages can be converted into absolute values, which much more objectively reflect the state of the leukocyte population.
Granulocytes are so called because they contain granules in their cytoplasm, which contain biologically active substances necessary for leukocytes to perform their protective functions. There are three types of granulocytes:
- Mature neutrophils have a nucleus and granules segmented into 4-5 lobules, which turn purple when stained according to Romanovsky-Giemsa. Segmented neutrophils make up the bulk of peripheral blood leukocytes. In much smaller quantities in the blood, neutrophils of the previous stage of maturation can be found - band neutrophils (with a nucleus not yet divided into lobules). Cells of earlier stages of maturation (metamyelocytes, myelocytes and others) can appear in a blood smear in exceptional cases - for example, in severe infectious diseases, when the bone marrow throws out not yet mature cells to fight the infection (this is called a shift of the leukocyte formula to the left), and also in chronic myeloid leukemia.
- Eosinophils are involved in antiparasitic immunity and the development of allergic reactions. Their granules, which are orange-pink in color, contain mediators of allergy and inflammation. Eosinophils also differ from neutrophils in the structure of their nucleus - it is bilobed.
- Basophils are granulocytes that take an active part in immediate allergic reactions. They have an S-shaped non-segmented nucleus, which is often not visible due to large granules of intense blue color containing allergy mediators.
- Lymphocytes are cells with a large nucleus, practically devoid of cytoplasm. When stained according to Romanovsky-Giemsa, their nucleus is stained in an intense purple-violet color, and the cytoplasm is blue-blue. Lymphocytes participate in more complex immune reactions associated with the recognition of their own and foreign antigens and the production of antibodies. There are three classes of lymphocytes: T lymphocytes, B lymphocytes and NK cells (natural killer cells), but standard staining does not allow them to be distinguished; more technically complex methods are used for this (for example, immunophenotyping).
- Monocytes are relatively large leukocytes containing an unsegmented bean-shaped nucleus and, unlike lymphocytes, a large amount of cytoplasm. When stained according to Romanovsky-Giemsa, the nucleus acquires a purple-red color, and the cytoplasm becomes a cloudy bluish-gray. The main function of monocytes is phagocytosis, that is, the absorption and digestion of microorganisms, their own dying cells, etc.
The above types of leukocytes are found normally in a peripheral blood smear. In some diseases, cells that normally should not be in the smear may enter the blood from the bone marrow: for example, blasts are the morphological substrate of acute leukemia. In the conclusion to the study, the number and, if possible, morphological features of atypical cells must be indicated.
In addition to counting the number of cells, a laboratory diagnostic doctor, using microscopy of a blood smear, notes changes in the morphology of leukocytes:
- Toxogenic granularity of neutrophils - dark large coarse granules are present inside the cells, which are formed as a result of coagulation (“welding”) of the cytoplasmic protein under the influence of intoxication products.
- Vacuolization of the cytoplasm is also caused by severe intoxication, under the influence of which fatty degeneration occurs in the cell, and when the smear is fixed with alcohol, droplets of fat dissolve and the cells acquire a characteristic appearance.
- Knyazkova-Dele bodies are large pale blue areas of the cytoplasm of neutrophils, free from specific granules. Also found in inflammatory diseases, sepsis.
- Hypersegmentation of neutrophil nuclei - more than five segments in the nucleus of a segmented neutrophil. It may be a congenital feature (in which case it has no clinical significance), but a consequence of a deficiency of vitamin B12 or folic acid.
- Pelger's leukocyte anomaly is a congenital disorder of neutrophil maturation, manifested by a decrease in the segmentation of their nuclei. Mature neutrophils contain an unsegmented or two-segmented nucleus. This is not accompanied by a violation of the physiological properties of neutrophils.
- Botkin-Gumprecht shadows are dilapidated nuclei of leukocytes with remnants of nucleoli, obtained in the process of preparing a smear from tumor cells in chronic lymphocytic leukemia.
What is the research used for?
- To determine the number of individual types of leukocytes and their relationship with each other, assessing the morphological characteristics of leukocytes.
When is the study scheduled?
- If an infectious disease is suspected, as well as a pathology of bone marrow hematopoiesis.
- If the number of leukocytes deviates from the reference limits according to a blood test performed on a hematology analyzer.
What do the results mean?
Reference values
Leukocytes
| Age | Reference values |
| Less than 1 year | 6 - 17.5 *10^9/l |
| 1-2 years | 6 - 17 *10^9/l |
| 2-4 years | 5.5 - 15.5 *10^9/l |
| 4-6 years | 5 - 14.5 *10^9/l |
| 6-10 years | 4.5 - 13.5 *10^9/l |
| 10-16 years | 4.5 - 13 *10^9/l |
| More than 16 years | 4 - 10 *10^9/l |
Neutrophils
| Age | Reference values |
| Less than 1 year | 1.5 - 8.5 *10^9/l |
| 1-2 years | 1.5 - 8.5 *10^9/l |
| 2-4 years | 1.5 - 8.5 *10^9/l |
| 4-6 years | 1.5 - 8 *10^9/l |
| 6-8 years | 1.5 - 8 *10^9/l |
| 8-10 years | 1.8 - 8 *10^9/l |
| 10-16 years | 1.8 - 8 *10^9/l |
| More than 16 years | 1.8 - 7.7 *10^9/l |
Lymphocytes
| Age | Reference values |
| Up to 1 year | 2 - 11 *10^9/l |
| 1-2 years | 3 - 9.5 *10^9/l |
| 2-4 years | 2 - 8 *10^9/l |
| 4-6 years | 1.5 - 7 *10^9/l |
| 6-8 years | 1.5 - 6.8 *10^9/l |
| 8-10 years | 1.5 - 6.5 *10^9/l |
| 10-16 years | 1.2 - 5.2 *10^9/l |
| More than 16 years | 1 - 4.8 *10^9/l |
Monocytes
| Age | Reference values |
| Up to 1 year | 0.05 - 1.1 *10^9/l |
| 1-2 years | 0.05 - 0.6 *10^9/l |
| 2-4 years | 0.05 - 0.5 *10^9/l |
| 4-16 years | 0.05 - 0.4 *10^9/l |
| More than 16 years | 0.05 - 0.82 *10^9/l |
Eosinophils
| Age | Reference values |
| Up to 1 year | 0.05 - 4 *10^9/l |
| 1-6 years | 0.02 - 0.3 *10^9/l |
| 2-4 years | 0.02 - 0.5 *10^9/l |
Basophils: 0 - 0.8 *10^9/l.
Blood smear microscopy
Neutrophils - rods: 0 - 5%.
Neutrophils - segment.
| Age | Reference values |
| Up to 1 year | 16 — 45 % |
| 1-2 years | 28 — 48 % |
| 2-5 years | 32 — 55 % |
| 5-7 years | 38 — 58 % |
| 7-8 years | 41 — 60 % |
| 8-12 years | 43 — 60 % |
| 12-16 years old | 45 — 60 % |
| More than 16 years | 47 — 72 % |
Lymphocytes, %
| Age | Reference values |
| Up to 1 year | 45 — 75 % |
| 1-2 years | 37 — 60 % |
| 2-4 years | 33 — 55 % |
| 4-6 years | 33 — 50 % |
| 6-8 years | 30 — 50 % |
| 8-10 years | 30 — 46 % |
| 10-16 years | 40 — 45 % |
| More than 16 years | 19 — 37 % |
Monocytes, %
| Age | Reference values |
| Up to 1 year | 4 — 10 % |
| 1-2 years | 3 — 10 % |
| More than 2 years | 3 — 12 % |
Eosinophils, %
| Age | Reference values |
| Up to 1 year | 1 — 6 % |
| 1-2 years | 1 — 7 % |
| 2-4 years | 1 — 6 % |
| More than 4 years | 1 — 5 % |
Basophils,%: 0 - 1%.
An increased level of neutrophils can be observed during acute bacterial infections, intoxications and myeloproliferative diseases.
Neutropenia can be caused by severe infection, sepsis, toxic effects on the bone marrow (cytostatics, ionizing radiation, myelotoxic drugs), aplastic anemia, as well as congenital diseases (Kostmann's neutropenia, cyclic neutropenia).
The most common causes of eosinophilia are allergic diseases, parasitic infections, and myeloproliferative diseases.
An increase in basophils may indicate allergic reactions or myeloproliferative diseases.
Absolute lymphocytosis occurs in viral infections, including infectious mononucleosis and cytomegalovirus infection, chronic lymphocytic leukemia.
to a decrease in the number of lymphocytes .
Monocytosis is possible with infections, granulomatous diseases (tuberculosis, brucellosis, sarcoidosis), blood tumors, systemic connective tissue diseases.